Government Cuts and Older People's Health in the UK
1.0 CHAPTER ONE
1.1 Introduction
The following research project will address how the government cuts on the health and social care services will affect the health and wellbeing of the older people in the United Kingdom, focuses on the significance of healthcare dissertation help. The terms older and aging will be used interchangeably in this project. In identifying who is an old person, this project will adopt the definition by the world Health Organization , that is a person who has retired from paid job and is under pension at the age of 60 -65 years ( world confederation for physical therapy, 2016). This chapter will address the following, background and rationale, aims and objectives literature search strategy and ethical consideration of the project.

1.2 Background and rationale of the study
The need to care and support the population of the aged has led to more focused efforts in the past years by the government and other non-governmental organizations to come up with the aging health care policies (Baines, 2013).
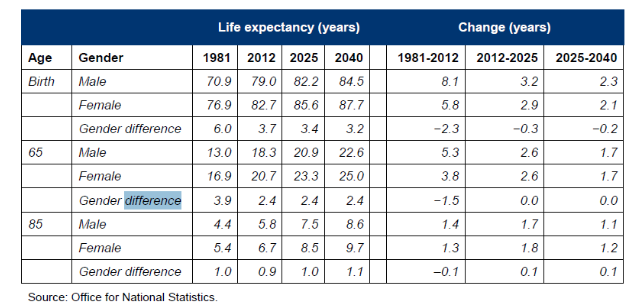
According to van der Steen, Radbruch, Hertogh, de Boer, Hughes, Larkin, & Koopmans, (2014) the wellbeing of the old people is associated with longer survival whereby 29.3% of the old people in the lowest quartile of the older people who had lived a wellbeing and healthy life. This can be summarized in the table below.
A study by Berkman, Gardner, Zodikoff & Harootyan, (2015)shows that the quality of life is affected by the state of health and social care that the individual receives. Banks, Nazroo & Steptoe (2012) revealed that health and social care is a determinant of the well-being of people aged 65 years and above. Some care programs started by the government help improve the wellbeing of the old people because they do not have the ability to work and provide for themselves (Binstock, George, Cutler, Hendricks, & Schulz, 2011). The medical services provided to the older people play a significant role in their wellbeing because of their health conditions such as coronary diseases, reduced mobility, stroke, cancer, isolation and loneliness that require professional services (Binstock, George, Cutler, Hendricks & Schulz (2011); Lothian & Philp, 2001).
Continue your journey with our comprehensive guide to Sickle Cell: Global Health Priority.
Berkam and Harootym (2013), note that the increased number of old people in the community has led to the demand for social care services from the government. In addition, as emphasized by Bolton (2016), in most cases the old people with higher levels of needs are the ones who get the medical services and social care. This has greatly affected their health in a positive way( Department of health, 2016 b). There is a reduction in social and health care service expenditure by 2.8 million pounds by 2019 (Lowndes and Prachet, 2012). Although the care Act (2014) ensures the government requirement for local authorities to address unmet needs, there is still the great concern of unmet needs; there is still the great concern of unmet need.
Given the rise of in the number of older people in the UK against the backdrop of government-reduced expenditure in health and social care services, it is imperative to explore this further. Thus this research will be significant in not just investigating the prevalence of older people usage of social care services in the UK but also understanding the effects of reduced government expenditure on social care and health services on the health and wellbeing of the older people. The study will also suggest recommendations for future policy deliberations.
1.3 Aim
To investigate the impacts of government cuts on social care and wellbeing of the old people in the United Kingdom
1.4 Objectives
a. To examine the prevalence of old people use social care services in the United Kingdom
b. To explore how government cuts on social care services provision affects the health and wellbeing of the old people in the United Kingdom
c. To assess the measures that can be adopted to emancipate the older people as far as health and social care is concerned in the UK.
1.5 Literature search and strategy
The literature search will access only evidence-based literature to give clear information and understanding in that subject area. Research involved the compilation of the vital records, family, surveys, and the records from the health care administrative from different sources. The catalogs of bodies dealing with aging people such as the European Union, Age, and Ageing were compiled. Data sources will include books, academic journals, articles and online sources. Online sources will be evaluated based on their accuracy, currency, coverage authority and objectivity before using them (Bell, 2010).
Data bases such as academic search, search complete, PubMed, social care online and Cochrane library will be used. The major search engines will be google scholar, google and google books. .
The literature strategy will also be applied to national studies that have comparison across survey done on the issue of the use of administrative data system and other data sources about health and social care on matters of the elderly. The use of the minimum database can provide the descriptive data about elderly, the disease, social care programs and facilities, medicals services access and the other related data elements concerning the issue.
Keywords
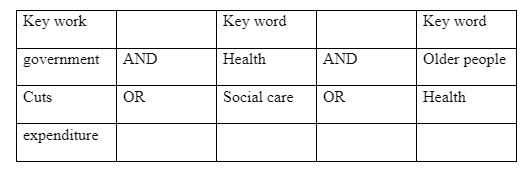
Key words include Older people , social care and health, prevalence , government, government cuts policies , wellbeing ,UK, alternatives and synonyms will be sued to generate the highest number of useful results. Moreover, Boolean operators such as the use of terms like and /or between key word will be used to improve the search as shown below.
The inclusion criteria in the literature search are data of the old people only (65 years and above) which gives clear information about the health, social care, health status and wellbeing of the individual. Demographic details, the diseases, and programs that the elderly participate in is also considered in the criteria.
The exclusion criteria involve any person under 65 years and the data explaining about men or women. The excluding data involved people less than 65 years is important because the research is about the old people only (world confederation for physical therapy, 2016)
1.6 Ethical consideration
All literature selected will be acknowledged to avoid plagiarism. Principles of ethics articulated by Baines (2013) will be ensured. This includes autonomy, respect, beneficence, not- maleficence and justice will guide in the sound reasoning of judgment. Some tension and dilemma may arise in the research. For instance the older people restriction from income support activities thus playing less active roles in the society and weakening their health. This may cause harm especially for the black minority.
1.7 Project outline
Chapter 1 will include the background and rationale, aims and objectives of the study and legislations. Chapter 2 - literature review- will examine the prevalence of older people use of social care and health services in the UK and explore the impacts of government cuts on health expenditure on the health and welling of the older people in the UK. Chapter 3- address the relevant health policies and strategies in the auk and their impacts on the health and wellbeing of the aging people in the United Kingdom. Moreover, it offers a critical focus on one social care home and critically analyses one of the intervention responding to the health and wellbeing of the ageing. Chapter 4- offers the summary of the findings and recommendations. In addition, a subjective reflection on the search process is offered here. Finally, a bibliography is given at the end of the research project.
1.8 Summary
The chapter has identified that in the United Kingdom the number of the older people is increasing daily. Moreover, it was noted that health and social care for these people is very crucial for their wellbeing. For a long time the government has been funding the health services in the UK. However, there is a tremendous decrease in government expenditure on the health and social care in the UK. This then revealed the knowledge gap that the project sought to fill.
CHAPTER TWO
2.0 Literature review
2.1 Introduction
Healthy ageing is regarded as a promotion of healthy living and prevention by the management of illness or disability associated with ageing. Normally, ageing can be thought as an accumulation of changes over the life course that increases fragility. Accordingly, if we can come up with effective and efficient measures to prevent the onset of chronic diseases and increase health life expectancy, there will be social, economic and health gains for us all. This section presents a review of the available sources that are related the prevalence of older people use of social care and health services in the UK and explore the impacts of government cuts on health expenditure on the health and welling of the older people in the UK.
2.1 Prevalence of old people use social care services in the United Kingdom
Anttonen& Sipilä (2016) notes that by 2018 approximately 7 million older people will not be able to walk up one stair without resting. Moreover, about 1.5 million people will not be able to see their friends enough across the road. Addition it is reported that over 4 million old people will experience hearing problems while up to a third of the people aged 75 years and above will be having the dual sensory loss. Again, reports indicate that over one million of the people aged 75 years and above will find it hard to get to their local hospital while a third of a million people will be having it difficult in bathing. Approximately, one million will have dementia. The trends above is an indication of the increasing prevalence of the use of social and health care services by the aged population in the United Kingdom.
On their part, Kane & Kane (2015) notes that currently, the older people account for approximately 60% of the gross current social care expenditure by local authorities. Despite the recent downward trend, those over 65 years account for nearly 40% of all hospital days with 65% of National Hospital (NHS) spend being on those aged over 65 years. The number of old people aged 65 years who need care services would rise from 9.7 million to 14.5 million in 2035 respectively. The number of those aged above 85 years is estimated to rise fast during this period by 122% from 1.3 million in 2015 to 2.5 million in 2035. The rise is attributed to the increase in male life expectancy. The number of old people using local authority funded home care services and direct payment is approximated to rise by 52% between the year 2015 and 2035. E above is necessary to ensure that peace is kept in demographic pressures. This rise can be summarized in the figure below.

Moreover, Beswick (2015) reports that the preference of old people makes up 7% of social care services. The above is because the number of the old people aged 65 years old is increasing by a 5th while those people age 85 years by a 3rd. Moreover, the preference increases due to the idea that old age groups are more likely to have health conditions. Many of those infections are preventable and manageable. However, it is significant to note that although in aggregate an increasing number of old people will lead to an increased demand for health and care services. It is crucial to realize that old ages do not automatically mean poor health. The onset of age-related conditions and-and illnesses can be avoided or delayed, or the impact on people's lives can be significantly less thus the need for social care services may not be reduced even in the later lives.
Additionally Fries, Koop, Beadle, Cooper, England, Greaves, & Wright (2016) Indicates that having a health condition does not automatically imply dependence on social care and healthcare services .this reduces the prevalence to seek for home care and healthcare related services. Statistics indicate that 50% of them do not regard themselves to be living with a life limiting long-term condition. The above then implies that even if they have a one or two health conditions. The above is not regarded to have a significant impact on their lives. In addition, it is noted that the number of old women in need of health and care services is more compared to their male counterparts. The above is based on the idea that mothers receive more care and love from their children when they grow old as compared to the fathers.
Grewal, Lewis, Flynn, Brown, Bond & Coast (2016) notes that the prevalence of health and care services depend on some factors which include: changing patterns of employment, economic factors, social changes and cultural diversity, for instance, the terms of employers impact or influence the availability of resources. Individuals and their families to purchase their assistance in old age. On the other hand, increase in divorce, remarriages and increase in the number of children born outside marriages. The above implies a tremendous growth in reconstituted families. In this way, children may have several parents and grandparents figures and family obligations.
2.2 How government cuts on social care services provision affects the health and wellbeing of the old people in the United Kingdom
For a long time in the United Kingdom, there h been supplementing health and social care for the older and aged people. The policy was very instrumental in ensuring that the old people get quality and better services. The national health received funding from taxation and was free at the point of need. However, in the recent past, the government has reduced or cut its spending on health and social care for the aged people.
McKee argue (2010) notes that for six consecutive years, cuts to the local authority budget the rising demands for the services, and the shortage of the staff has left the social care system incapable of meeting the wants of the ageing people who depend on it. The above situation is placing an unacceptable load on unpaid caregivers and is an increasing number of ageing individuals who have difficulty with the fundamental activities of daily living such include: washing, dressing and getting out of bed without any support at all.
Wilkinson & Marmot (2013) note that there is evidence that the decline in fee given by local councils and other cost limitations such as the national living wage are processing the income of residential and home care providers. The report contends that a rise in the number is most likely to quit the market or go out of the business. As a result leaving older people without the care, they need. The reduction in a budget of care providers is also driving some affluent region to step back from providing care for people financed by local authorities. This situation has those who depend on council financing relying on amplifying threats are safety. In addition to this, more individuals are forced to pay for their care due to the cuts to local authority services.
Lowndes & Pratchett (2012) contends that Statistics also indicate that a growing gap exists within the inefficient system that will at least reach 2.8 million pounds by the financial year 2019/2020 as the public spending on adult social care declines to less than one percent of the Gross Domestic Product (GDP). It is significant to note that failure by the government to reform the social care and increase the funding has led to a system that leaves older people, their families and care providers pick up the places. As much as the local authorities have tried their best save while protecting funding for the poorest, care providers are struggling on the low fee the council can afford. Deficiencies and shortages of home care staff and at cost friendly home places imply that often, ageing individuals are often stuck in hospital putting their both lives and vital national health services in jeopardy. Unmet needs are rising, and the service providers are threatening to pull out of the contract.
Taylor‐Gooby (2012) argues that the social care for the older people in the United Kingdom is experiencing massive pressure. There is an increasing number of old people who need health and social care services. The trend has put a lot of strain increased workload and pressure on the caregivers and providers. With this, the people are left with no option. It has reached a situation where people access to care services is based on what the individual can afford and where they reside. The demand for these services no longer depends on what they require or need. The above then implies that there is a gap in the provision of care. The older people are not receiving support on their needs.
Under investments in the national health services is undermining the policy objective of ensuring the people are independent and out of residential care. According to the care act, 2014 has created a new demand and expectations. However, funding has not kept pace. Indeed local authorities have little room to make further savings and most will soon be not able to meet the basic legal responsibilities.
Fries, Koop, Beadle, Cooper, England, Greaves, & Wright (2016) notes that the cuts have increased stress on and primary expanded the workload of health caregivers. There has been an increase in uneven treatment by the central government with local authorities that have more deprived people who suffer disproportionally high cut level. Social care spending has fallen significantly in the most deprived region by about 14% while in real terms, the least deprived communities have to spend 28% more on social care.
Kickert (2012) notes that greater cuts were witnessed in most deprived authorities have made small changes in the range of services offered. For instance, many have cut the library and leisure opening hours. Although small, these changes have impacted on access to those services on the ageing people who spend their time happily with those services. The author also contends that for the rich ageing people, this may not be a big problem since they can seek for those services privately at an extra cost. However, for the poor ageing individuals, there is a huge challenge due to their financial inability. They will end up having a service gap, as they cannot meet the extra cost for private services.
Exworthy, Blane & Marmot, (2003) notes that stressed services have also come due to the cuts affecting service access to the ageing people in the United Kingdom. Some service users report busier offices with long queues, complications in placing/ appointment and at times withdrawing specialists from care centers leading to poor quality service provision. Staff reduction has led to a rise in the workload of the remaining staff. The above has led to the limited time that a care officer can spend on the public working face and decrease the number of staff in operational roles. Even the staffs are concerned with the suffering of services. They report that there is a reduction in the standard of services offered to the clients. In addition, there is less time to assist the service seekers coupled with little collaboration with the colleagues. In the end, there is less time to think how to improve the services leading to long term suffering of the ageing population in the United Kingdom seeking for these services.
Goldberg (2013) argues that the cuts have led to social care services to the aged becoming a last resort. The above implies that there are attempts to narrow down service provision to the most vulnerable or needy. The above trend can raise the risks of residualization. Normally several studies have revealed that residualised services are normally of poor quality. Additionally, despite the attempts to get rid of residualization, it will gain momentum and base unless the pace and scales of government cuts on the social care services are reduced.
Health and Social Care Information Centre (2016b) reports that there is reduced face-to-face contact with staff and care service seekers. There is also conflict between the service users and givers with clients leaving offices and harassing the staff who have failed to apologize for keeping them for long on waiting. Lack of qualified staff in care homes will jeopardize the safety of care seekers. There is also loneliness and depression in the elderly population since families have less contact with the elderly. Reduction in health and social care will limit the chances of the older people interacting with one another in care homes leading to feelings of loneliness and depression.
2.3 Strategies in tackling social care needs of the older people in the United Kingdom
Since time in memorial, the United Kingdom has been relying on immigrant labour in social work for the ageing population. The above has its limitation, especially with reduced cuts. The above then implies that the United Kingdom has to make use of the UK-born workers with EU-non-workers immigration policy (Hughes, McMurdo & Guthrie, 2013). The UK aims at reducing the entry of non-EU workers to the UK. The above will limit the degree to which social caregivers can make use of non-EU workers as a workforce to carry o in caring for the older people. In the end, these limitations will amplify the efforts to recruit other workers within the UK.
Institute of Public Care, (2016) notes that The UK government has set up several strategies to address social care for the older people in the UK. About this, on 13 June 2014 Fuller working lives: a framework for action was published. The framework explains how working longer can benefit people, businesses, the community and economy at large. The framework sets out several actions that are geared towards helping the older people have fuller working lives. In 2014, again the government made steps towards challenging the outdated perceptions about the order. Workers within the business community this was achieved by appointing Dr Ros as the business champion for the older workers. In 2015 Dr Ros, recommendation was published with the aim of improving the lives of older workers (50 years).
Ryan, Netten, Skåtun, &Smith (2006) notes that such initiatives of enabling the older people to stay in work and if they wish after state pension age can help to support them financially, health and social wellbeing of these individuals in later life. The government has also erased the default retirement age. In addition, about this, people cannot be forced to retire simply because they are 65 years old. Another strategy is getting older people online. The above is based that this century is a digital era. Accordingly, everything from providing services to social interaction is undergoing changes. As information and services become digital, we need to ensure that the older people are not left behind and that they can fully increase independence that comes with digital competence.
A celebration of older people’s day is another strategy. Normally, this is held on 1 October annually to coincide with the United Nations International day of older persons (Leutz, 2009). The major goal of this day is to celebrate the achievements and contributions of the older people to our society and economy. By so doing, these celebrations handles the negative attitude and stereotypes that people (especially) young social care workers have concerning the older people.
Localism is another strategy, being used localism is advantageous since the local health and targeted initiatives can tackle social priorities and innovative strategies can be established to promote and enhance integrated working between departments (Exworthy, Blane & Marmot, 2003). However, it also has the potential of worsening the pesticides lottery. Here the quality and availability of NHS of the older will be defined by where they lived.
2.4 Summary
In this chapter, it is revealed that there is a general increase trend in the number of the older people in the United Kingdom. With such increasing figures, it is evident that there is a high prevalence of the older people to make us of health and social care services. The above is based on the idea that as the individual get old they become weak and more susceptible to health conditions, moreover it is revealed in the chapter that female old people are less likely to require social and health services as compared to their male counterparts.
The chapter also reveals that for a long time the government has been funding health and social care services in the UK for the older people. However, in the current century, there is a decline trend in the government expenditure on these services. The above has led to negative impacts of the health and wellbeing of the older people in the United Kingdom. Poor quality service delivery, overcrowding, inaccessibility and to special care services are some of the major impacts of government cuts on health and social care services. It was also revealed that there are several strategies adopted to enhance the health and wellbeing of older people in the united kingdom .Such include the fuller working life framework , celebration of older people’s day and localism.
3.0 CHAPTER THREE
3.1 Introduction
This chapter address the relevant health policies and strategies in the UK and their impacts on the health and wellbeing of the aging people in the United Kingdom. Moreover, the chapter offers a critical focus on one social care home and critically analyses one of the intervention responding to the health and wellbeing of the ageing.
3.1 Relevant policies/ strategies/ legislation addressing the health issue]
3.1.1 Anti-smoking policy
The United Kingdom has passed some health and social care policies and legislations. For example, we have the (anti-smoking policy 2010-2015). Smoking was regarded as one of the contributors to deteriorating health of the aged people in the United Kingdom. Martin (2014) notes that there were nearly 80,000 deaths associated with smoking in England in the year 2011. Additionally Whitehead (2011) notes that each year the United Kingdom hospitals admit patients with smoking illnesses approximately 9500. Accordingly the government set itself to reduce smoking rates in the country. To achieve the policy, media advertising and promotion of tobacco were banned. The above strategy reduced the eye-catching the display of tobacco thus sensitizing the order and the masses on the negative impact of tobacco usage.

Moreover Whitehead (2011) notes that the taxes of tobacco have risen. The above is to make them less affordable to the older people who depend on family to provide money. The above in turn discourages consumption. There are also anti-smoking campaigns such as smoking free campaign that encourages people to alter their actions. The campaigns are geared towards making people aware of the dangers associated with smoking especially among the older and the young people. They also aim at making people stop smoking and avoid public smoking.
3.1.2 Obesity and healthy eating
Another policy is the 2010-2015 government policy on obesity and healthy eating. Studies such as Dare, Mackay & Pell (2015) indicates that in England, many people are obese. The aged make up 61.9% of the adults (Kind, Dolan, Gudex, & Williams, 2008). Health studies indicate that people who are obese have a higher risk of getting diabetes type 2, heart disease and other types of cancers. Excess weight can also make it difficult for the older people to move around and even climb stairs. The step can affect negatively on their self-esteem and mental health.
Through this policy, the government aimed at reducing the number of obese people. The above is achieved through the change of life programs, improving labelling on food and drinks to help people to make healthy choices (Ferlie & Shortell, 2016). They also offer guidance on physical activities. The policy has helped increase healthy living among the older people in the United Kingdom. The public health responsibility deal has four elements, (food, alcohol, health at work and physical activities). It encourages businesses to sign up for its conditions and motivate people to eat more healthy to prolong their life expectancy. They are encouraged to reduce fats and fat contents that if people eat, it will harm them and help people take fewer calories and more healthy foods.
3.2 Case Study: Cedar Lawn Home Care
3.2.1 Justification
For this case study, cedar lawn is discussed. Cedar Lawn is located in Stratford- upon- Avon. Majority dedicated for the older people. The Organization has chosen here since the workforce in the Organization demonstrates a very clear understanding of the needs and interests of the older people. Additionally, the staff here understands how to engage with the older people in a positive manner. The residents are treated with respect and dignity thus leaving them happy and relaxed in the company of the staff. Additionally, the Organization has freedom for the residents. For instance, they chose the time they go to bed and wake up in the morning. The Organization also offers delicious meals and residents have a choice to choose what they want to eat. Additionally, the workforce here provides the residents with a choice of whether or not to join in the activities such as board games. Local schools also visit the residents at the home care on a regular basis. The above conditions then necessitate the choice of cedar lawn for this case study. The above is due to the idea that this study is majorly focusing of healthy ageing in the United Kingdom.
3.2.2 Background
Cedar lawn was started in 1970 and opened its link with Sheldon trust. The Organization has over 50 care homes in England and Wales. In 1997, an extension was added raising the home to carry a capacity of 24 to 34. The Organization claims one resident. The NHA’s Stratford home is well named because of a cedar tree, that is expensive and caring. It shelters you from all elements (Home cares, 2016). Cedar Lawn home care offers comfort, compassion and friendship. The core goal of the firm is to treat the residents with dignity and respect. They deserve 24hours whether in privacy or company of others. Cedar Lawn staff ensures that they have given their residents the support they need. The environment in the home makes it more appealing to the residents. The gardens invite residents to fresh air or even tend to plants if they so wish. The farm has the latest safety and security design features. It also has a prayer room.
Some of the services offered at Cedar Lawn home care include traditional home cooking, hairdressing, physiotherapy, chiropody, dental, optical and personal laundry services. There is also a provision of entertainment services within and outside the home as well as local pubs, shops and churches for the residents (Home cares, 2016). In addition, there is a successful kitchen garden set up by the staff and the residents for growing vegetables of various types. The above makes the residents feel the fruits of their labour.
3.2.3 Major Programme by Cedar Lawn home care
One of the major programs in Cedar Lawn is the provision of residential health and social care to the old people who require a residential care due to general infirmity and who experience dementia and mental health difficulties. The Programme is relevant to this topic of study because my project focuses on older people‘s health and social care in the United Kingdom. The major aim of the Programe is to offer the older people perfect health and social care living in their old age. It also aims at making her residents feel at home loved and identified with the community (Sentel healthcare, 2016). This Programme is based on the freedom of the residents. Major sources of funds to cedar home care include the fee paid by private residents who seek their services. Moreover, the firms get funding from the local and/or National Health Service (NHS) Trust. The national health services are government funding (Sentel healthcare, 2016). Additionally, the local authorities can offer funds to the firm. Additionally, cedar lawn home care receives funding from donors and well-wishers as well as her sponsors. Other organizations dealing with the welfare of the older people in the United kingdoms are also a source of funds to this body.
3.2.4 Strengths and weaknesses of the Programme
Its strengths include its expansive nature. The Organisation has over 50 centers across the United Kingdom. Additionally, the freedom accorded to the residents enables them to feel very at home. The situation is enhanced and promoted by the presence of the kitchen gardens that makes these older people feel the home environment. The facilities are comfortable, and the staff has expertise in handling the older people. However, the Programme has its weaknesses too much freedom on the residents is not good on the organizational goals and mission. In this way, it is as if the residents are running the firm thus limiting its goal attainment. Basically in as much as freedom required for home care residents , it should be noted that the freedom of the residents should end where the rules of the home care begins. However, it is significant to address the question on when does the individual resident rights take precedence over the rules of the firm.
3. 3Summary
In this chapter, various policies were discussed in relation to health and wellbeing in the United Kingdom. These include the anti-smoking policy and obesity and health eating policy. The policies are very relevant as far as ensuring proper health and social care of the older people is concerned. Good eating habits coupled with limited smoking improve the health of the older people making them stronger thus less need for social care services. In addition, Cedar Lawn home care was discussed. It was noted that the home care is primarily meant for the older people in the United Kingdom. If offers friendly environment for the residents thus making them feel at home. Additionally, the residents have freedom of choice and expression thus making them full participants in the activities within the homecare. Services offered by the homecare include traditional home cooking, hairdressing, physiotherapy, chiropody, dental, optical and personal laundry services. There is also a provision of entertainment services within and outside the home as well as local pubs, shops and churches for the residents. The major Programme in the homecare is the provision of residential health and social care to the old people who require a residential care due to general infirmity and who experience dementia and mental health difficulties. Major strengths of the Programme include ability to expand globally, freedom of the residents and expertise work force and adequate facilities. The ability to expand globally is an indication of a firm that can offer international or world class services not only to the aged in the UK but also from other countries. Additionally the presence of skilled and qualified workforce enables the firm to offer quality services to the service seekers. However, it should be noted that the provision of these services in addition to skill depends on the workers motivation and engagement in important aspects of the firm. It is thus with no doubt that, the works at Cider Lawn are motivated and involved in decision making processes of the firm evident in the way they treat their residents with dignity and respect.
However, too much freedom on the residents is not good on the organizational goals and mission. At times, they need to be put into truck for effective running of the firms. The above is based on the idea that controlling many people needs a set of rules to guide them to avoid each acting in her or her own ways that can negatively affect others.
CHAPTER FOUR
Conclusion and Recommendation
4.1 Introduction
This chapter offers the summary of the findings and recommendations. Moreover, the chapter presents a subjective reflection on the search process.
4.2 Conclusion
The major aim of this project was to examine social care services and wellbeing for the older people in the United Kingdom. The study was a secondary research. The inclusion criteria included work that focuses on the social care and wellbeing of the people aged 65 years and above. The exclusion criteria included those individuals who are aged below 65 years old. The searching stages included searching key terms in research engines such as Google Scholar, national health services website and other online websites that would offer relevant information to this study.
It was noted that older men in the United Kingdom prefer the use of health care services as compared to their women counterparts. The findings further indicated that the government cut on health and care services had affected negatively on the health and well-being of the older people in the United Kingdom. Social care spending has fallen significantly in the most deprived region by about 14% while in real terms, the least deprived communities have to spend 28% more on social care.
Over 40% of the aged in the UK cannot be able to access health and social care services that they need. Moreover, the homecare and health provisions centers for these people are reducing in number since almost 20% of them are closing down due to their high operational costs. Poor quality services are witnessed due to residualization of health and social care services. This puts the lives and safety of the older people seeking for the care services at jeopardy. The findings also indicated that there are several health policies that exist in the United Kingdom. This project discussed the anti-smoking policy, which aims that reducing smoking policy, the obesity policy and improved recruitment of the older people policy.
In the section two, of this study, a case study of Cedar home care was given as far as health, and social care organizations are concerned. The major sources of funds for this home care is the national health services, the local authorities, donors and well-wishers as well as international organizations that deal with the welfare of the older people. The Programme is so powerful since it is the residential center and can be expanded to other centers. However, too much freedom of the residents proved to be the major limitations.
4.3 Recommendations
This study proposes some recommendations. The movement of the United Kingdom ought to increase the funding of health and social care for the older people. The above is based on the idea that health is a very basic need for any human being. Secondly, the government ought to increase the number of the UK born citizens working as home care and healthcare workers to reduce the labour shortage in these facilities. Moreover, there is need to come up with more active and broad policies to deal with the wealth and well-being of the older people in the United Kingdom.
4.4 Personal reflection
Throughout a project the writer has learnt and gained a lot both as a student of health care and a scholarly researcher. As the researcher, I have realized that coming along conflicting opinion from different authors and sources is common and therefore critical textual analysis is needed to help in distinguishing the credible sources from incredible sources. Moreover, I have learnt that for a proper research one has to carry out the intensive and extensive reading of available resources as far as the topic under discussion is concerned.
I have also learnt that acknowledging sources is one of the major ethical considerations in research. The project has also enabled me to note that some other sources are very hard to access especially those to do with government reports and funds. Additionally, I realized that critical literature review needs a lot of time to come up with a scholarly literature. The above is due to the idea that I had to engage with each author or report identified to examine its focus, findings and if the work is relevant to this project.
In furtherance, I have realized that a good project can only be arrived at if one works with a period and stick to the activities of each time. Additionally, I realized that a research budget is very significant for any research.
As a student of health and social care, I have realized that health and social care is a calling and one ought to have passion in dealing with the older people. The field has several challenges, and the primary limitation is funding. As such one need to be patient and persevering in taking care of the older people even when the facilities are not enough or even when the workload is huge. The project also has shed light on the future anticipations of the United Kingdom society. The older people are likely to be more than the young people are. These statistics then brought something unique to the United Kingdom people.
Another crucial element that I have learnt is the negative perception provided to the people working as caregivers in the older people homes. Accordingly, I taught that it would be good if the United Kingdom launched national campaigns towards sensitizing the masses on the important of taking care of the aged individual and well as launch capacity building forums aimed at attitude towards negative perception of the older people is concerned.
Throughout the project, I have realized that the area of health and social care in the United Kingdom has several areas that need to be critically and intensively studied. Moreover, intensive research is needed on the impacts of the Brexit on the health and social care services in the United Kingdom. In fact, if am to do another research my major focus will be on the Brexit and the national healthcare provision in the United Kingdom. Scholars can also focus on the health care policies and strategies in the United Kingdom in the post-Brexit period and how these policies will influence the labour supplied by the European Union immigrants and examine some of the already existing works such as (SUMPTION,2017).
This research has given me the motivation to mobilize the youths and student who I can manage to sensitize the public on the importance of taking care of the older people in the United Kingdom.
References
- Anttonen, A. and Sipilä, J.,(2016). European social care services: is it possible to identify models?. Journal of European social policy, 6(2), pp.87-100.
- Baines, S.,( 2013). Music therapy as an anti-oppressive practice. The Arts in Psychotherapy, 40(1), pp.1-5.
- Berkman, B., Gardner, D., Zodikoff, B., & Harootyan, L. (2015). Social work in health care with older adults: Future challenges. Families in Society: The Journal of Contemporary Social Services, 86(3), 329-337.
- Binstock, R. H., George, L. K., Cutler, S. J., Hendricks, J., & Schulz, J. H. (Eds.). (2011). Handbook of aging and the social sciences. Academic Press.
- Chambliss, D.F. & Schutt, R.K., (2012). Making sense of the social world: Methods of investigation. Sage.
- Davies, M.B. & Hughes, N., (2014). Doing a successful research project: Using qualitative or quantitative methods. Palgrave Macmillan.
- Department of Health (2016). Care and Support statutory guideline: Available at http:// gov.uk (Accessed on 28th November 2016).
- Exworthy, M., Blane, D. & Marmot, M., (2003). Tackling health inequalities in the United Kingdom: the progress and pitfalls of policy. Health services research, 38(6p2), pp.1905-1922.
- Ferlie, E.B. & Shortell, S.M., (2001). Improving the quality of health care in the United Kingdom and the United States: a framework for change. The Milbank Quarterly, 79(2), pp.281-315.
- Fries, J. F., Koop, C. E., Beadle, C. E., Cooper, P. P., England, M. J., Greaves, R. F., ... & Wright, D. (2016). Reducing health care costs by reducing the need and demand for medical services. New England Journal of Medicine, 329(5), 321-325.
- Goldberg, S.E., et al.,(2013). Care in specialist medical and mental health unit compared with standard care for older people with cognitive impairment admitted to general hospital: randomised controlled trial (NIHR TEAM trial). Bmj, 347, p.f4132.
- Grewal, I., Lewis, J., Flynn, T., Brown, J., Bond, J., & Coast, J. (2006). Developing attributes for a generic quality of life measure for older people: preferences or capabilities?. Social science & medicine, 62(8), 1891-1901.
- Health and Social Care Information Centre 2(016b). NHS Work Force Statistics: March 2016 Provisional statistics. Available at http://content.digital.nbs.uk (Accessed on 1st December, 2016).
- Home cares, (2016). Cedar Lawn Nursing Homes. Available at https://www.carehome.co.uk/carehome.cfm/searchazref/20001035ROMA
- Hughes, L. D., McMurdo, M. E., & Guthrie, B.( 2013). Guidelines for people not for diseases: the challenges of applying UK clinical guidelines to people with multimorbidity. Age and ageing, 42(1), 62-69.
- Institute of Public, Care (2016). Who pays for the care? An analysis of self-funders in the social care market –Institute of Public Caro: - Oxford Brokers University. Available at http:// ipc.brookers.ac.uk (Accessed on 3rd December, 2016).
- Kane, R.L. & Kane, R.A., (2015). What older people want from long-term care, and how they can get it. Health Affairs, 20(6), pp.114-127.
- Kickert, W., (2012). State responses to the fiscal crisis in Britain, Germany and the Netherlands. Public Management Review, 14(3), pp.299-309.
- Kind, P., Dolan, P., Gudex, C. and Williams, A., (2008). Variations in population health status: results from a United Kingdom national questionnaire survey. Bmj, 316(7133), pp.736-741.
- Leutz, W.N., (2009). Five laws for integrating medical and social services: lessons from the United States and the United Kingdom. The Milbank Quarterly, 77(1), pp.77-110.
- Lothian, K., & Philp, I. (2001). Care of older people: Maintaining the dignity and autonomy of older people in the healthcare setting. BMJ: British Medical Journal, 322(7287), 668
- Lowndes, V. and Pratchett, L., (2012). Local governance under the coalition government: Austerity, localism and the ‘Big Society’. Local government studies, 38(1), pp.21-40.
- Martin Roland, D., (2004). Linking physicians’ pay to the quality of care—a major experiment in the United Kingdom. N Engl J Med, 351, pp.1448-54.
- McKeeargue, M., (2010). Budget crises, health, and social welfare programmes. Bmj, 341, p.77.
- Moule, P. & Hek, G., (2011). Making sense of research: an introduction for health and social care practitioners. Sage.
- Naidoo, J. & Wills, J., (2000). Health promotion: foundations for practice. Elsevier Health Sciences.
- Punch, K.F (2016). Developing effective research Proposals 3rd edition. London: Sage
- Ryan, M., Netten, A., Skåtun, D. and Smith, P., (2006). Using discrete choice experiments to estimate a preference-based measure of outcome—an application to social care for older people. Journal of health economics, 25(5), pp.927-944.
- Sentel healthcare, (2016). Cedar lawn care homes. Available at: http://www.sentinel-healthcare.co.uk/cedar_lawn_nursing_home.htm
- Taylor‐Gooby, P., (2012). Root and branch restructuring to achieve major cuts: The social policy programme of the 2010 UK coalition government. Social Policy & Administration, 46(1), pp.61-82.
- van der Steen, J. T., Radbruch, L., Hertogh, C. M., de Boer, M. E., Hughes, J. C., Larkin, P., & Koopmans, R. T. (2014). White paper defining optimal palliative care in older people with dementia: a Delphi study and recommendations from the European Association for Palliative Care. Palliative medicine, 28(3), 197-209.
- Walker, H., (2011). Studying for your social work degree. SAGE.
- Whitehead, M., (2011). The concepts and principles of equity and health. International journal of health services, 22(3), pp.429-445.
- Wilkinson, R.G. and Marmot, M., (2013). Social determinants of health: the solid facts. World Health Organization.
Continue your journey with our comprehensive guide to Exploring the Role of Plant Foods and Flavonoids in Cardiovascular Disease Prevention.



- 24/7 Customer Support
- 100% Customer Satisfaction
- No Privacy Violation
- Quick Services
- Subject Experts