Exploring the Role of Plant Foods and Flavonoids in Cardiovascular Disease Prevention
Flavonoids: Examining Trends in Adoption and the Protective Effect against Cardiovascular Diseases
Section 1: Introduction
Whereas cardiovascular diseases reveal a declining rate in the past two decades, it remains the leading cause of death for individuals aged 65 and above. Pharmacologic and medical interventions play a critical role in reducing mortalities associated with the condition in at risk persons, yet the high costs and some of the adverse side effects associated with such approaches continue to be reported1. Therefore, lower risks for the cardiovascular disease have been documented to exhibit a correlation with the consumption of plant foods2. The association is ascribed to the magnesium, potassium and fiber content found in these plant foods. Additional constituents such as flavonoids have also been documented to be responsible for the protective effect linked to plant foods and the prevention of the cardiovascular disease. Found primarily in cocoa, nuts, vegetables, fruits and beverages (such as wine and tea), flavonoids constitute non-nutrient, non-caloric and polyphenolic secondary metabolites in plants3. With the threat of the cardiovascular disease’s impact on the current trend in mortality rates perceived to be significant and, with this outcome coming in the wake of the adoption of flavonoids, it becomes imperative to examine the possible protective effect of the latter in addressing cardiovascular disease and their associated adversities on populations. This dissertation focuses on the trend in adoption and the protective effect of flavonoids against cardiovascular diseases. For students seeking healthcare dissertation help, getting the chance to explore the role of flavonoids in mitigating cardiovascular risks through valuable insights.
1.0 Cardiovascular Diseases
Cardiovascular diseases refer to conditions involving blocked or narrowed blood vessels that cause stroke, chest pain (angina), or heart attack. Similarly, the cardiovascular disease is associated with other heart conditions that affect the rhythm, valves, and muscles of the heart4. In most cases, the cardiovascular disease is associated with atherosclerosis. This condition develops due to the buildup of plaque in the arteries’ walls5. Upon the buildup, the arteries narrow and pose difficulty to the flow of blood. In addition, situations where blood clots are characterised by probable stoppages to the flow; causing stroke or heart attack. Apart from stroke and heart attack, other types of cardiovascular diseases include heart failure or congestive heart failure (due to the heart’s inability to pump blood normally and adequately), arrhythmia in which the heart beats irregularly, too fast, or too slow, and heart valve problems in which the heart fails to open enough to support an adequate flow of blood6. Regurgitation is also a condition related to the cardiovascular disease and occurs when the valves of the heart fail to close properly; implying that the blood is unlikely to leak through appropriately. It is further notable that related conditions or those associated with the cardiovascular or heart diseases include heart defects or congenital heart defects, and the coronary artery disease. Therefore, the condition is characterised by blocked or narrowed blood vessels and, in most cases, is linked to the nature of population lifestyles7.

1.1 Epidemiology of Cardiovascular Diseases
Proximal risks associated with cardiovascular diseases have been documented. For example, consumption patterns such as alcohol use, tobacco, and diets combine with health services, activity patterns and biological risk factors such as blood glucose, clinical disease, blood pressure and increased cholesterol to yield adversities8. The cardiovascular disease (CVD) is also a leading cause of mortality and morbidity and accounts for about 17.3 million deaths globally and annually. The figure is also predicted to increase to 23.6 million by 2030. Notably, 80 percent of the deaths are reported in middle- and lower-income countries9. As such, CVD is the largest contributor to non-communicable diseases that have a large share of mortality and morbidity in the world. However, incidents of CVD vary with factors such as ethnic background, gender, and geographical region. Similarly, incidents of CVD vary based on the prevalence of risk factors; such as those mentioned earlier.
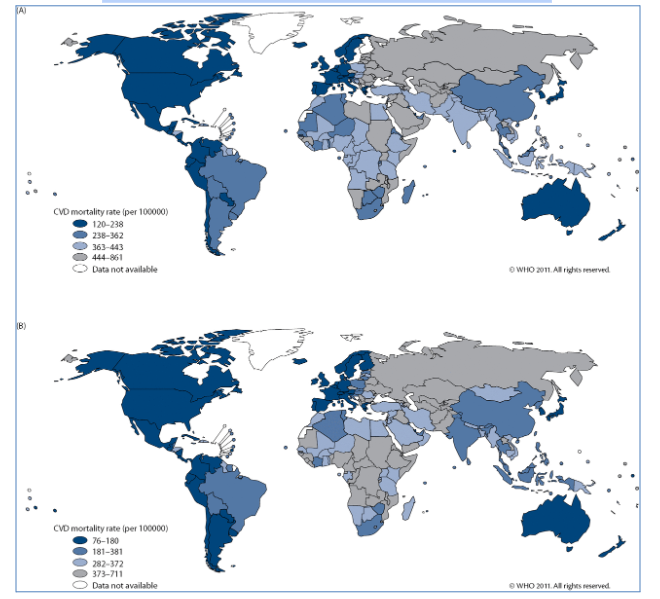
Ischaemic heart disease accounts for 38 percent of deaths due to CVD while 46 percent of CVD deaths in men are associated with the same condition. The disease is closely followed by the cerebrovascular disease that accounts for 37 percent and 34 percent of deaths in women and men respectively. It has also been affirmed that the burden of CVD remains higher in Western countries especially the trend witnessed in the 20th century but certain Middle Eastern and Asian regions have been documented top experience CVD cases10. Based on country statistics, the Russian Federation indicates the highest number of cases of stroke, CVD and the coronary heart disease (CHD) in men (308, 1,185 and 659 per 100,000 persons respectively) and women (158, 463 and 221 per 100,000 persons respectively)3. On the other hand, Israel has revealed the lowest number in men at 24, 133 and 72 per 100,000 persons respectively. In France, the conditions have been the lowest in women at 14, 51 and 12 in every 100,000 persons respectively. However, intermediate rates have been reported in the U.S. with women revealing outcomes of 22, 124 and 56 per 100,000 persons respective and men 30, 250 and 143 per 100,000 persons respectively4. The following figures fig 1, 2 illustrate these outcomes regarding CVD incidents and its related conditions, as well as the global trends in the distribution of the disease.
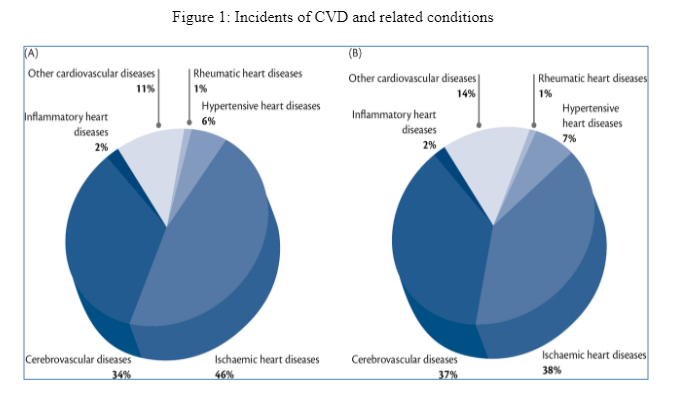
Figure 2: Global distribution of CVD incidents and related conditions
In the U.S., a dramatic increase in CVD prevalence has been reported in men aged 20 to 39; revealing a 12.8 percent increase. However, absolute mortality among women in the period after 1985 has exceeded that of men and this trend is attributed to CVD treatment and related risk factors and lifestyle improvement (such as significant reduction in cigarette smoking)10. However, some of these declines or reductions in trend are projected to be negated by increasing obesity epidemic.
1.2 Treatment of CVD (Pharmacological and Non-Pharmacological Approaches)
For patients diagnosed with CVD, treatment goals target to relieve symptoms, reverse, stop or slow plaque buildup through risk factor reduction, lower risks associated with blood clot formation, bypass or widen plaque-clogged coronary arteries, and prevent complications associated with the coronary heart disease12. In some situations, cases of CVD are addressed through lifestyle changes. For example, quitting smoking has been observed to be an ideal approach in which community groups, workplaces and hospitals have been platforms for helping people to quit smoking or avoid secondhand smoking. Following a healthy diet has also been observed to form a major contributory approach to addressing CVD. Notably, a healthy diet is that which includes a variety of fruits and vegetables13. The foods can be dried, frozen, or fresh. In addition, healthy diets constitute low-fat or fat-free dairy products, whole grains, and protein foods. The latter include peas, beans, seeds, nuts, processed soy products, seafood, poultry without skin, and lean meats14. Dietary habits have also been documented to include an avoidance of drinks and foods high in added sugar, limitations in refined grain and solid fats, and moderated alcohol consumption (if one drinks).
Physical activity is another approach to addressing CVD and its associated adversities. For instance, it has been established that regular physical activity is important due to its capacity to reduce the coronary heart disease’s risk factors that include excess weight, high blood pressure, and high LDL cholesterol15. It is further notable that physical activity raises the LDL cholesterol level (responsible for removing cholesterol from the arteries) and lowers risk for diabetes; a predictor of CVD. Some of the heart healthy exercises include walking and other moderate-intensity aerobic activities (on a weekly basis). A healthy weight can also be maintained by cutting back the intake of calories and eating smaller portions5. Negative aspects of stress and depression have also been documented to constitute critical risk factors for CVD. As such, getting angry or upset is likely to trigger heart attacks. Similarly, some of the approaches that sections of members of a population seek while coping stress (such as overeating, smoking and drinking) are not healthy to the heart. As such, stress management through relaxation is perceived to be an ideal method of improving physical and emotional health that, in turn, translates into reduced adversities of CVD. Stress relief is also achieved by sharing one’s concerns or feelings with people in their life. Given that depression exhibits the capacity to triple or double risk for the coronary heart disease, medicines may be prescribed or counseling recommended for managing the condition1.
Therefore, medicines apply in situations where lifestyle changes are not adequate. One of the objectives is to relieve CVD symptoms while reducing the workload of the heart. In addition, medicines serve to decrease an individual’s chance of dying suddenly or having a heart attack. As such, the approach lowers CVD risk factors, reduces blood pressure, and strives towards low LDL cholesterol. Furthermore, medicines serve to prevent blood clots; besides delaying or preventing the need for surgeries or procedures that include coronary bypass grafting and angioplasty. Medicines have also been prescribed for women suffering from broken heart syndromes due to the capacity of this method to manage stress hormones that constitute crucial predictors of CVD6. Specific medicines administered to curb CVD include ACE inhibitors (that widen arteries with the aim of lowering blood pressure to support the blood pumping process in the heart), aldosterone inhibitors that ease water buildup and swelling caused by the heart while enabling the kidneys to send unneeded salt and water from blood and tissues into urine), angiotensin II receptor blockers (ARBs) responsible for lowering blood pressure, and beta-blockers whose role is to prevent adverse effects of epinephrine or adrenaline. The eventuality is that beta-blockers enable the heart to work better. It is further notable that beta-blockers drop the production of harmful substances made by the body while responding to heart failure6. Additional medicines include cholesterol-lowering drugs and calcium channel blockers. Regarding the former, they address situations where the walls of arteries are characterised by a buildup of cholesterol (resulting from inflammation). On the other hand, calcium channel blockers treat high blood pressure and angina by increasing the flow of oxygen and blood to the heart and relaxing the blood vessels. Overall, calcium channel blockers are important due to their capacity to ease the heart’s workload10. Overall, medicines used for treating CVD fall in broad categories such as vasodilators, diuretics, digitalis preparations, cholesterol-lowering medications, calcium channel blockers, combined alpha and beta-blockers, beta blockers, angiotensin-receptor nephrilysin inhibitors (ARNIs), and antiplatelet agents. Others include angiotensin II receptor inhibitors or blockers and angiotensin-converting enzyme (ACE) inhibitors4. In other circumstances, procedures and surgeries such as coronary artery bypass grafting and percutaneous coronary intervention are adopted.
1.3 Role of Plants in CVD
For many decades, the treatment of most diseases has been linked to the use of drugs appearing in the form of synthetic chemicals. In addition, several traditional plant-based medicines have played critical role in health care. For example, phytochemicals form natural bioactive compounds have been used. Specifically, phytochemicals are found in roots, flowers, leaves, aromatic plants, medicinal plants, fruits and vegetables and act as defense systems responsible for combating against diseases9. Examples of phytochemicals’ ranges of chemical entities include organosulphur compounds and vitamins, steroidal saponins, flavonoids, and polyphenols. Similarly, several bioactive compounds found in terrestrial plants have been avowed to reduce population risks for the cardiovascular disease due to the effect they pose in terms of cardioprotection; with CVD documented to be the leading cause of death in the world3. Examples of such bioactive compounds include carotenoids, tocotrienols, sulforaphane, catechin, quercetin, resveratol, diosgenin, and isoflavones16. Indeed, the cardioprotective effect resulting from various phytochemicals is associated with the anti-ischemic, antiantiogenic, antihypercholesteroemic, antioxidative, and inihibition of inflammatory activities and platelet aggregation whose eventuality is a reduction of the risk for CVD12. Imperative to note is that this paper focuses on flavonoids as one of the chemical entities constituting a range of phytochemicals. Observations indicate further that the structure-function relationship of the phytochemicals mediates their multi-faceted role11. The central idea is that phytochemicals are found in plants such as seeds, nuts, beans, grains, fruits and vegetables while alternative approaches involving antioxidants can be in both animal and plant foods. Thus, antioxidants are minerals or vitamins that aid in the prevention of damage to cells15. Whereas side effects may be associated with situations where phytochemicals and some of the alternative treatment approaches that have been discussed (such as coronary bypass grafting, angioplasty, ACE inhibitors, aldosterone inhibitors, angiotensin II receptor blockers (ARBs), and beta-blockers), the overall observation is that both approaches address CVD from the perspectives of preventing its occurrence, controlling the disorder, or managing the symptoms10. The following section provides an examination of flavonoids as selected chemical entities form the range of phytochemicals will be provided. Prior to this examination, fig 3 illustrates the role played by phytochemicals in addressing CVD.
Figure 3: Phytochemicals and CVD

Section 2: Flavonoids
Flavonoids refer to a large class of plant pigments composing structures similar to or based on that of flavones. With these pigments ranging from yellow to red to blue, flavonoids are found in herbs such as peppers, dill, citrus fruits and grapes, as well as vegetables and fruits. Water-soluble and biologically active plant compounds are also characteristic of flavonoids8. An example is that which constitutes tea flavonoids that have been reported to protect populations against the heart disease and some cancers.
2.1 Types of Flavonoids
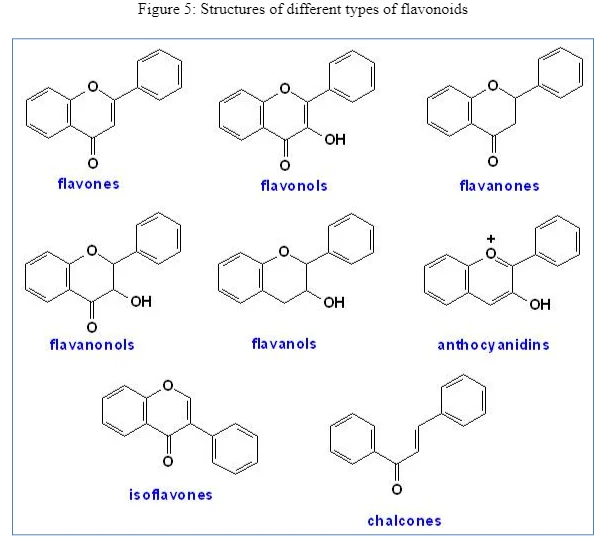
One of the categories constitutes anthocyanidins, which have been documented as the most abundant type and are responsible for the purple or blue color presence in blackberries, grapes, cherries, and blueberries. Indeed, over 500 anthocyanidins have been found in various natural sources, plants, and herbs. Another category entails flavonols2. The role of the latter lies in their capacity to treat allergies and are found in cacao; often associated with vasodilatory effects, increased synthesis, and enhanced blood flow and continue to be indicated for strokes and dementia. The third category constitutes flavanones, which are present in many fruits and herbs; with the citrus fruits taking a significant share among the sources1. The fourth type is that which involves flavanols, which are widely spread in nature and exist in leaves and plant pigments. Apart from flavonols, flavones are another category of flavonoids and, although not as widespread as the former, are found in some plants and herbs and have been documented to yield or exert certain levels of anti-tumor properties9.
Another type involves isoflavones, which are mostly present in the Leguminosae family (such as soya beans). Besides, catechins form another type of flavonoids and exist in wine, tea, pears, cherries, and apples5. Lastly, chalcones have a significant anti-inflammatory, anti-tumor, anti-fungal, and antibacterial property. It is further asserted that chalcones exhibit a further responsibility felt in terms of yellow pigmentation of anthers and petals in the early stages of flowers such as Petunia. However, these colors are converted to colorless flavanones in the later stages of such flowers.

2.2 Sources of Flavonoids
Perceived to produce antioxidant activities that play significant roles in preventing conditions such as cancer (that result from free-radical damage) and supporting cardiovascular health, flavonoids are found in certain plant-based groups of food. One of the groups entails berries such as the purple, blue and purple berries. In addition, a higher flavonoids value has been observed to exist in riper and darker berries. Quantities of the flavonol group (such as myricetin and quercetin) have also been found in cranberries and blueberries while black grapes constitute flavonoids catechin and epicatechin. Similarly, red grapes, cherries and raspberries are high in cyaniding and anthocyanidins4. Apart from berries, tree fruits form another source of flavonoids. For example, bananas contain anthocyanidins such as delphinidin and cyaniding while citrus fruits such as oranges, limes, lemons and grapefruit are high in flavonoids such as eriodictyol, naringenin, and hesperetin. Members of tree fruits belonging to the Rosaceae family have also been found to contain epicatechin and catechin and include apricots, peaches, plums, pears, and apples14.
Nuts and beans form an additional source of flavonoids. For example, dark beans that constitute kidney and black beans are high in flavonoids belonging to the anthycyanidins group (such as kaempferol, petunidin, malvidin, and delphinidin) while beans that tend to be comsumed in an immature form (such as pinto snap beans or fava beans) are rich in flavonoids belonging to epigallocatechin and epicatechin6. It has been observed further that pecans and walnuts are high in anthocyanidins while cashews and pistachios are rich in flavonols catechins. Additional sources include vegetables. The most notable have been those that entail red and green vegetables while members of the nightshade family (such as eggplants, tomatoes and peppers) are rich in the flavones luteolin. Onions (such as green and red onions) are also high in quercetin. Flavoring agents and spices, when consumed in smaller quantities, have been found to form additional sources of flavonoids. Examples include dill and thyme. Lastly, flavonoids have been reported to exist in beverages. Specific examples include red wine, fruit juices and all types of tea (green, red and black varieties) have been observed to form rich sources of flavonols that include thearubigin. The following figures illustrate these sources.


2.3 Clinical Use of Flavonoids
The role played by flavonoids in health support accounts for their adoption and usage. Major factors prompting the clinical use of flavonoids include the antioxidant benefits, anti-inflammatory benefits, cardiovascular system benefits, the support lent to the nervous system, and other health benefits. Given that most of the flavonoids (such as flavan-3-ols and flavonols have been found to be effective in the reduction of free radical damage to body components and cells, they offer antioxidant benefits17. However, it remains unclear on whether flavonoids can be categorised in the same group as other widely known antioxidant nutrients such as vitamin E and vitamin C (as their concentration in a person’s blood stream is lower). However, a consumption of flavonoids-rich foods leads to a better protection of certain cell types18. Regarding the anti-inflammatory benefits, flavonoids block the production of messaging molecules; with the latter being responsible for the promotion of inflammation. Thus, flavonoids offer anti-inflammatory benefits by inhibiting the lipoxygenase (LOX) and cyclo-oxygenase (COX) enzymes. This benefit is felt in cases where specific flavonoids are used and those in which flavonoids-containing extracts (such as herbs, spices and a variety of foods) are adopted19.
As mentioned earlier, flavonoids have been documented to exhibit cardiovascular system benefits. Given that most of the problems affecting an individual’s cardiovascular system are associated with problems resulting from inflammation and oxidative stress, food flavonoids offer anti-inflammatory and antioxidant benefits by supporting this body system directly20. Regarding the bloodstream, flavonoids help in the protection of LDL cholesterol molecules against oxygen-related damage. In turn, the LDL protection aids in lowering risks for atherosclerosis. The integrity and strength of the walls of blood vessels have also been reported to increase in situations where flavonoids such as hesperidin and rutin have been used. The eventuality is that the use of these flavonoids lowers risks of problems of the blood vessels1. Additional outcomes have seen numerous flavonoids play the role of preventing excessive clumping together of platelet cells. In turn, the prevention curbs against unwanted clogging of blood vessels; often referred to as an anti-aggregatory property (through which the cardiovascular system is supported by phytonutrients).
In relation to support extension to the nervous system, flavonoids have been observed to protect nerve cells against oxygen damage. In addition, flavonoids have been critical during the demanding and slow process of nerve regeneration (outside the spinal cord and the brain). It is further notable that the onset of sections of chronic neurodegenerative disorders such as Alzheimer’s disease and age-related dementia is likely to be delayed by a strong and long-term intake of flavonoids16. Lastly, benefits to the nervous system are felt when flavonoids support better brain functioning (such as cognitive functioning) due to their capacity to improve the flow of blood in the brain18. Other benefits include improved detoxification and better regulation of cell cycles.
Section 3: Aim and Objectives
In this study, the main aim is to determine the protective effect of flavonoids in addressing cardiovascular diseases. Other related research objectives are stated as follows:
- To determine current trends in the use of flavonoids as solutions to the adversities resulting from CVD
- To establish some of the challenges faced by health care providers and practitioners while seek to adopt and implement the use of flavonoids as solutions to CVD
- To determine the relationship between flavonoids intake and the rate of recovery among patients diagnosed with CVD
- To determine incident rates of CVD in populations documented to take foods high in flavonoids
Section 4: Methodology
4.1 Research Design
A qualitative approach has been selected to collect and analyse data. Indeed, qualitative research is used to gain an understating of the underlying motivations, opinions and reasons in a given subject, belief, culture or event and provides insight into the problem by helping the researcher to develop hypotheses or ideas17. In this study, qualitative research is deemed to be appropriate because it provides a desirable level of convenience during the process of data collection and sampling. In turn, the resultant convenience offers an opportunity through which effective and efficient organisation of the research results or outcomes is achieved. By forming a platform from which research outcomes are organised effectively and efficiently, qualitative research forms a foundation that leads to the engagement in data analysis in an appropriate way21. Similarly, the qualitative approach to research has been selected because it provides an opportunity through which elements such as trends, impacts, challenges faced, and the resultant protective effect of flavonoids can be understood. In addition, qualitative research has been adopted because the results are not apparent to the researcher. It is also worth noting that the approach has been adopted because of the capacity it exhibits in collecting detailed and comprehensive data.
Another merit arising from this outcome is that it enables the researcher to gain an inclusive mental picture from different viewpoints and leads to the formulation of more practical and realistic recommendations. Furthermore, the qualitative research approach is critical because it enhances research continuity in such a way that recommendations for future study could be made and, if implemented, could expand the health care field. Thus, the qualitative technique forms a probing approach in which inference drawing is preceded by the creation of fresh or new ideas that are independent and unique from others techniques of conducting research; including the mixed studies approach that incorporates qualitative and quantitative approaches in the same study.
4.2 Data Collection
The process of collecting data will involve the use of secondary sources. These sources include books, journals, magazines, newspapers, and e-books. The aim of this criterion is to collect data in its original form, shunning possibilities of bias during the interpretation and discussion processes. Thus, the interviewees were asked questions and requested to respond for interpretation purposes. Secondary data, which refers to the existing form of data collected and analysed by previous researchers in the same or similar field, is helpful to the study. It is further notable that secondary data leads to the understanding of some of the procedures that previous researchers may have followed, with the understanding aiding in determining the most appropriate design that could be applied in a given field.
4.3 Data Analysis
To analyse primary data outcomes, the existing scholarly contributions will be classified based on the degree of similarity in different outcomes received. To make this data more meaningful, scholarly contributions that exhibit a close correlation in terms of the protective effect of flavonoids while seeking to address cardiovascular diseases will have their responses classified and grouped together. The aim of this classification is to discern some of the forces that could account for the perceived similarities and differences in the outcomes received, with dominant outcomes expected to inform about the state of flavonoids’ protective effect in relation to cardiovascular diseases. The eventuality is that a content analysis technique will be used to analyse and interpret the results received from some of the primary research studies that have been conducted previously, with descriptive and inferential statistics aiding in arriving at reliable and viable conclusions.
4.4 Assumptions and Limitations
As mentioned earlier, this study is based on the use of a content analysis technique. One of the limitations of this approach is that the outcomes collected from secondary sources of data can be influenced or manipulated by the researcher. Such influences or manipulations could, in turn, lead to biased analysis and interpretation processes. In addition, the content analysis technique is prone to social desirability bias in situations where the previous primary research studies accounting for the resultant secondary sources of data may have been marred by subjective responses that tend to be inaccurate and fail to reflect the actual protective effect of flavonoids in addressing cardiovascular diseases21. Lastly, misinterpretations and misunderstandings are likely to result when the content analysis approach utilises articles produced by previous scholars from varying socio-cultural and linguistic contexts.
4.5 Delimitations
To curb the above limitations, the content analysis technique will examine the existing research outcomes from secondary sources in their original form without interference and manipulation. The eventuality is that misunderstandings and misinterpretations will be avoided by assuring neutrality, rather than attract social desirability bias in which the results are analysed and interpreted with subjectivity, rather than foster objectivity. An adequate number of secondary sources of data will also be used to interpret and analyse the outcomes to avoid bias or overgeneralizations based on a limited target population. Indeed, this step is expected to add to outcome validity and reliability in the current study.
4.6 Ethical Issues
This study will conform to ethical specifications in various ways. For example, the study adheres to the issues of intellectual property rights to avoid contravening the previous scholars’ contributions (by acknowledging their work and citing their opinions where necessary). In addition, data confidentiality and privacy will be enhanced to avoid interfering with the rights of the previous researchers whose work will be consulted and contribute to inference making. Overall, a content analysis technique is used to collect and analyse data before drawing conclusions and making recommendations. With aspects of intellectual property rights and data privacy (or confidentiality) assured, this study is deemed to be ethical and well placed to collect data and make reliable conclusions regarding the protective effect of flavonoids in addressing cardiovascular diseases.
Section 5: Findings, Analysis and Interpretation
As stated in section 4, this study adopts a content analysis technique in which outcomes from the existing secondary sources are used to collect, analyze and interpret data. In this section, findings about the protective effect of flavonoids against cardiovascular diseases are presented to guide the inference making process, upon which recommendations will be made accordingly. A study focusing on tea flavonoids and the cardiovascular disease was conducted by Hodgson. In the study, it was established that tea has a highly significant and positive effect on public health; especially the cardiovascular system21. Indeed, the study indicated that the significant impact of tea on the cardiovascular system arises from the presence of flavonoids (in high levels). It was also inferred that the flavonoids found in tea inhibit the development of atherosclerosis consistently among animal models. Specific findings suggested that tea and tea flavonoids lead to improvements in endothelial function, as well reduced risks of thrombosis, inflammation, blood cholesterol concentrations, oxidative damage, and reduced blood pressure.
5.1 Chocolate and CVD
The impact of chocolate in preventing cardiovascular diseases has also been studied22. Specifically, it has been hypothesized that the consumption of chocolate plays a significant role in reducing the risk of CVD because of the antioxidant flavonoids and high levels of stearic acid. Multiple lines of evidence from randomized trials and laboratory experiments have also suggested that flavonoids exhibit the protective potential against the coronary heart disease’s mortality while stearic acid may be neutral. Therefore, outcomes from short-term randomized feeding trials affirm that chocolate and cocoa may exert beneficial effects on CVD risk through decreased LDL oxidation, higher HDL, anti-platelet function, anti-inflammation, and lowered blood pressure. Furthermore, trials of stearic acid indicate that it (the acid) is cholesterol-neutral23. However, epidemiological studies focusing on dietary acid and serum remain inconclusive because of several methodologic limitations that compromise the validity and reliability of their outcomes. However, prospective studies focusing on flavonoids avow that the content found in chocolate is likely to reduce risk of CVD mortality.
In every 100 grams of milk chocolate, flavonoids have been found to constitute 170 milligrams. The predominant class is observed to constitute flavonol in chocolate and cocoa, and that cocoa has the highest amount of polyphenols and the quantity is documented to be 611 milligrams per serving while flavonoids epicatechin is affirmed to be 564 milligrams per serving. Thus, the quantity of flavonoids in cocoa exceeds that which is found in wine and tea24. Specific categories have also been found to exhibit variations in such a way that the amount of flavonoids in dark chocolate is substantially higher, compared to the amount found in milk chocolate25. For example, the former is observed to account for 951 milligrams in every 40-gram serving while the latter has 394 milligrams in every 40-gram serving. The implication is that a comparable level of epicatechin is found in dark chocolate as that in tea and wine17. Previous scholarly contributions have noted further that total phenols and catechins in dark chocolate tend to be significantly higher than the outcomes revealed when milk chocolate is analyzed. Furthermore, biologic effects posed by flavonoids found in dark chocolate have been found to be higher because the milk content in milk chocolate tends to inhibit the flavonoids’ intestinal absorption26.
Evidence that a high consumption of chocolate and cocoa yields decreased risks for CVD has also been revealed population studies. For example, a sub-study targeting a Zutphen elderly population indicated that the consumption of cocoa was linked to a decrease in the overall cardiovascular mortality, as well as a decrease in the level of blood pressure that the affected populations experienced24. Similarly, a case-control study conducted in Italy indicated that chocolate consumption exhibits an inverse association with the risk for myocardial infarction. Specifically, it has been documented that the decrease in risk for myocardial infarction lies at 77 percent among populations consuming over three portions of chocolate in every day, compared to the population that consumes less than one chocolate per day27. Several dietary intervention studies involving animals and humans have also indicated that flavonol-rich foods and beverages such as cocoa are associated with exertions of protective vascular effects. However, data for the above mentioned clinical and population studies indicates similar trends which suggest that flavanols constitute cardio-protective agents but the biochemical mechanism responsible for this state of cardio-protection is yet to be discerned to a conclusive extent28. In some vitro studies, it has been asserted that some of the flavanols’ health effects have their contributory biochemical mechanisms lying in processes such as the alteration of receptor functions and certain cell membrane properties, modulation of gene expression and cell signaling, and antioxidant effects27. Furthermore, flavanols have been associated with inhibitions of several enzyme activities. Therefore, it can be inferred that the consumption of chocolate poses a protective effect against cardiovascular diseases. However, the remaining dilemma is that the specific biochemical mechanism responsible for the chocolate’s state of cardioprotection is yet to be unpacked to a conclusive extent.

5.2 Tea, Flavonoids and Cardiovascular Health
Several epidemiological studies have examined the relation between the risk of CVD and the consumption of tea. In most cases, it has been evident that individuals who consume both black and green tea in high quantities exhibit reductions in the risk for CVD; despite the neutral results received in some of these studies29. Several meta-analyses have also sought to understand the relationship between tea and CVD risk. Some of the cardiovascular diseases on focus have included myocardial infarction, the coronary heart disease, and strokes. Specific contexts in which the studies have been conducted include Italy, the U.S., UK, the Netherlands, Finland, and Wales29. Some of these studies indicate that a range of 1-75 percent reduction in cardiovascular diseases is likely to be achieved for every three cups of tea that one consumes22. In addition, the studies have revealed that in contexts such as the UK and the U.S., a consumption of three cups of tea on a daily basis is likely to yield as significant as 11 percent reduction in the risk for myocardial infarction23. However, these studies caution that aspects such as geographical heterogeneity are likely to alter the outcomes and that an assumption of the uniform association between tea consumption and CVD across the global populations could be misleading. Compared to studies based in the U.S. context, those that have focused on continental European have been found to reveal a stronger inverse correlation between tea consumption and the risk of CVD. Apart from this variation in association due to the impact of geographical location, the nature or form of the tea consumed has been examined in relation to CVD. Outcomes indicate that the relationship between the coronary artery disease and the consumption of black tea is unlikely to reach statistical significance bait in situations where green tea is consumed, a significant association is reported and, a lower risk for the coronary artery disease (CAD) is documented21. Therefore, it can be inferred that an increase in the intake of green tea by a cup and on a daily basis is likely to yield a 10-percent decrease in CAD risk. Meta-analysis has also showed that individuals who consume about three or more cups of black (or green) tea exhibit a 21-percent reduction in the risk of non-fatal and fatal stroke19.
Epidemiological studies have also examined the relationship between the intake of flavonoids from beverages and flavonoids-containing foods such as chocolate, onions, apples, grapes and tea and the risk for CVD9. Results indicate that an increase in flavonoid intake leads to a decreased risk of cardiovascular diseases. In other studies, a 20-percent reduction in the risk for CHD death has been observed due to a high intake of flavonols dominated by tea as the main source. With two cups of tea perceived to hold about 34 milligrams of flavonols, it has been affirmed that a high intake of these products leads to a 20-percent reduced risk of stroke, compared to situations where populations are characterized by a low intake of the flavonols. Therefore, the consumption of tea poses a tertiary effect on CVD in such a way that it accounts for a higher intake of flavonoids that, in turn, lead to a significant decrease in risk7. However, it is imperative to highlight that sections of the epidemiological studies focusing on tea as a source of flavonoids that decrease the risk of CVD remain prone to the impact of various confounding factors. For example, the nature of lifestyle and health of the diet taken vary from one population and geographical location or socio-economic class group to another. Therefore, the potential trickledown effect of these variations on the risk for CVD implies that a reliance on research outcomes indicating the inverse correlation between tea consumption and the risk of CVD compromises the validity and reliability of the latter observation.
Blood pressure has been another focal subject of concern among studies that seek to understand its correlation with the consumption of tea, a major source of flavonoids. According to population studies, situations dominated by a regular and long-term ingestion of tea could translate into reduced or low blood pressure among the affected individuals3. Apart from blood pressure, dyslipidemia has been examined in relation to the consumption of tea. Specifically, most of the observational studies affirm that the intake of tea poses a beneficial effect on CVD. In other cases, intervention studies have revealed mixed outcomes regarding the effect of flavonoids and tea on improvements felt in serum lipid profile28. In some of the recent randomized controlled trials, a decrease of about one to two percent in LDL and total cholesterol has been reported in cases where green tea has been consumed. Indeed, the outcomes indicate that green tea poses a modest effect on plasma cholesterol and that the effect size remains small and may not be clinically relevant.
Given that platelet activation in an excessive manner is likely to cause an increase in susceptibility to clotting and aggregation, individuals may be prone to thrombosis and experience the latter’s tertiary effect of ischemic events that include stroke and myocardial infarction25. As such, vitro studies have been conducted to find out the role of tea rich in flavonoids in regulating these conditions. Findings suggest that high physiological concentrations of isolated flavonoids are likely to reduce both the markers of platelet aggregation and the plate aggregation process itself23. Intervention studies have also examined the impact posed by flavonoid-rich beverages and foods on platelet function. With findings found to be inconsistent (regarding the impact of tea on platelet function), it has been inferred that tea is unlikely to affect ex vivo platelet aggregation while, in some cases, some trials have shown that regular tea ingestion for a four-week period is likely to cause reductions in circulating p-selectin concentrations18. Imperative to note is that the latter is a marker of platelet activation.
Inflammation, perceived to play an important role in relation to the progression and initiation of vascular disease, has also been examined. Strong suggestive evidence in animal and vitro models indicates that tea, a source of flavonoids, yields an anti-inflammatory effect. However, mixed results have been observed (regarding the correlation between the consumption of tea and its potential effect on anti-inflammatory markers that include C-reactive protein) in situations where intervention and epidemiological studies focus on humans27. Specifically, most of the evidence from such studies does not reveal a strong anti-inflammatory effect of consuming tea.
Lastly, the aspect of oxidative damage has been examined in relation to the consumption of tea. In vitro studies, it has been asserted that tea and its flavonoids possess potent antioxidant activities. Specifically, consistent evidence indicates that the consumption of tea leads to the production of significantly higher plasma antioxidant capacities in humans. However, the physiological significance associated with an increase in plasma antioxidant capacities is yet to be determined in an in-depth manner15. Regarding the capacity of tea and its flavonoids to prevent DNA, protein and lipid oxidation in vivo, less promising evidence has been observed regarding the beneficial effects. Human and animal studies have also been conducted but limited evidence exists regarding the critical role played by tea and its flavonoids in inhibiting the oxidative damage in vivo. Therefore, current evidence fails to support in vivo antioxidant effects in situations where tea is consumed16. Overall, it has been observed that the role played by tea and flavonoids in cardiovascular health cannot be overemphasized. Specifically, population studies affirm that higher flavonoid diets and higher tea consumption leads to a decreased risk of cardiovascular diseases6, 9, 24. These findings have been complemented by intervention studies which consistently show that flavonoids and tea consumption lead to improved blood vessel function.
5.3 Vegetable and Fruit Flavonoids In Relation To CVD
Fruits and vegetables have been asserted to provide protection against diseases. Some of these diseases include cerebrovascular diseases, cardiovascular diseases, and cancer. Indeed, this state of protection has been associated with various antioxidants that the fruits and vegetables house14. In most cases, red wines are made from the grape variety, Vitis vinifera. As such, the consumption of red wines has been linked to the beneficial effect of protecting populations against developing atherosclerosis, as the flavonoids contained in the wine (whose primary or raw material is the grape fruit) exhibit an antioxidant activity. Specifically, the red wine contains flavonoids myricetin and quercetin, as well as epicatechins and catechins. It is also worth noting that the wine constitutes polymeric anthocyanins that include reservetrol, pelargonidin, malvidin, petunidin, peonidin, delphinidin, and cyaniding8. From these outcomes, epidemiological studies have demonstrated that red wine has a special protective effect; findings that have gained support from experimental research outcomes. For example, the flavonoids in red wine are avowed to protect LDL against oxidation ex vivo while inhibiting the proliferation of smooth muscles in vivo9. In both properties, an anti-atherogenic effect is mediated. Additional studies suggest that the grape seed extract has its most valuable flavonoid existing in the form of proanthocyanidins or procyanidolic oligomers. As such, grape seed extracts are reported to reduce population risks of stroke and heart attack due to the potent antioxidants that are avowed to prevent the development of plaque that could, if developed, clog one’s arteries3. Proanthocyanidins have also been observed to play a significant role that can be likened to that of aspirin in keeping blood cells from clot formation or sticking together18.
Apart from grapes, pomegranate forms another tree whose edible part of fruits constitute 20 percent seeds and 80 percent juice. Of the latter (juice), moisture accounts for 85 percent, total sugars 10 percent, and 15 percent constituting flavonoids, polyphenols, ascorbic acid, and pectin24. Indeed, pomegranate juice has been observed to possess antioxidant activities that could be three times higher in performance, compared to the antioxidant activity posed by green tea or red wine17. Indeed, this trend in the significant antioxidant activity (against lipoprotein) of pomegranate juice is attributed to the capacity it exhibits in scavenging free radicals. Similarly, the consumption of juice from pomegranate has been found to inhibit platelet activation, a risk factor for atherosclerosis and one that could yield the tertiary effect of oxidative stress. The effect of this juice has been linked to the manner in which the constituents of thus fruit interact with the surface of platelets and binds the sites for collagen. In addition, the capacity of the juice’s consumption to inhibit platelet activation has been associated with the capacity of its constituents to scavenge free radicals; attenuating the oxidative stress-induced platelet activation29.
Apples have also been found to contain flavonoids due to their richness in phytochemicals. According to most of the epidemiological studies, the consumption of apples leads to the reduction of risk for diabetes, asthma, cardiovascular diseases, and some cancers20. Laboratory results have also suggested that apples lower the cholesterol, decrease lipid oxidation, inhibit cell proliferation, and have a strong antioxidant activity. Specific phytochemicals contained in apples include epicatechin and catechin. Therefore, a consumption of these constituents of apples exhibits an inverse correlation with the coronary heart disease. The antioxidant activity of apples in vivo has also been reflected in their ingestion in such a way that decreased oxidation in diphenylhexatriene labeled phosphatidylcholine results7. Another major flavonoid in apples, quercetin, has been found to exhibit no relationship or effect on lipid oxidation among studies conducted on rats6. The implication is that this flavonoid is unlikely to account for the ability of apples to inhibit lipid oxidation solitarily. Rather, it contributes to the apples’ antioxidant activity alongside other flavonoids21.
Citrus fruits have also been studied not only as sources of flavonoids but also as potential contributors to the protective effect of flavonoids against the coronary artery disease. These fruits include lime, lemon, orange, and the grapefruit. Common flavonoids in these fruits include myricetin, quercetin, naringenin, and hesperidin. Wide ranges of properties that have been found in these fruits include the antioxidant, antitumor, and anti-inflammatory activities12. The free radical scavenging capacity of citrus fruits has been asserted to play an additionally critical role of protecting against damage to the DNA, lipids, and proteins. It is further notable that the citrus extract contains ascorbic acid and flavonoids that play the role of inhibiting VLDL oxidation, as well as the inhibition of in vitro cupric ion induced LDL27. Naringenin, which belongs to the class of flavanones, is abundant in these fruits. Indeed, its role lies in the capacity to prevent and treat diseases through their antiatherogenic compounds.
Lastly, berries have been associated with protection against the heart disease and certain cancers. For instance, redberry fruits such as bilberry, chokeberry and eiderberry have been used in regions such as North America and parts of Europe. Specifically, the phenolic compounds found in berries are dominated by the presence of anthocyanins; the main group31. In most of the types of berries, flavonols (quercetin) have been found to be in higher content than the epicatechin and catechin (or flacon-3-ols). However, the amount of flavon-3-ols has been found to be higher than that of flavonols in strawberries, red raspberries, and gooseberries. In bilberries, blueberries, cowberries, blackcurrant, and cranberries, myricetin has been detected32. According to epidemiological studies, an equal or greater effect is posed by the consumption of berries when compared to the intake of tea while seeking to lower CVD risk. This trend is associated with observations that the berries exhibit a higher flavonoid content than that which is found in tea. Specific berries that have been found to be potent free radical scavengers and good sources of antioxidants include strawberries, raspberries, and blackberries30. On the other hand, antioxidant compounds responsible for fighting arterial diseases through the prevention of LDL (bad cholesterol) oxidation have been found in blackberries, strawberries, sweetcherries and blueberries. As such, berries form not only form additional sources of flavonoids but also play a significant role in the protective effect against CVD; a property that is felt through the prevention of LDL oxidation.
Section 6: Conclusion and Recommendations
In summary, flavonoids refer to polyphenolic compounds found in various sources and exist in various types. Major sources include berries, fruits, nuts and beans, vegetables, and beverages (such as tea, cocoa and red wine). On the other hand, major types of flavonoids include anthocyanidins, flavanols, flavanones, flavonols, flavones, isoflavones, catechins, and chalcones. From this study’s outcomes, flavonoids show antiatherosclerosis properties through their antioxidant property that is observed during LDL oxidation. Therefore, a consumption of the aforementioned sources of fruits is indispensable, should populations seek to address the adversity of cardiovascular diseases, as well as their related implications. To fight diseases such as the coronary heart disease, there is a need to consume products such as fruits rich in flavonoids whose constituents are capable of fighting LDL oxidation. However, it is worth noting that the fruits highlighted tend to orient to well-known tropical and temperate zones. Furthermore, these fruits are highly seasonal. The implication to sectors such as community health practitioners is that facilitation and the allocation of resources to secure these food products is inevitable. This dissertation has also established that the study of flavonoids is complex due to the heterogeneous nature of various molecular structures, as well as the scarcity of information regarding bioavailability. Similarly, insufficient methods measuring the objective and end points, as well as the oxidative damage in vivo are insufficient. The eventuality is that there is a need for improvements in the analytical approaches used to give room for the collection of additional data about the processes of extraction and absorption. Overall, flavonoids in the aforementioned sources serve as critical agents responsible for protecting populations against CVD. As such, it is recommended that groups such as nutrition practitioners, community health care initiatives and government authorities not only embrace and engage in campaigns towards the consumption of these foods and beverages but also foster the resource provision or facilitation process towards the realization of healthy populations at local, regional and global levels.
References
- Flammer A, Sudano I, Wolfrum M, Thomas R, Enseleit F, Periat D et al. Cardiovascular effects of flavanol-rich chocolate in patients with heart failure. European Heart Journal. 2011;33(17):2172-2180.
- Greenland P, Alpert J, Beller G, Benjamin E, Budoff M, Fayad Z et al. 2010 ACCF/AHA Guideline for Assessment of Cardiovascular Risk in Asymptomatic Adults: Executive Summary. Journal of the American College of Cardiology. 2010;56(25):50-103.
- Eckel R, Jakicic J, de Jesus J, Miller N, Hubbard V, Lee I. 2013 AHA/ACC Guideline on Lifestyle Management to Reduce Cardiovascular Risk. A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2013;(2014;129:S76-S99).
- Goff D, Lloyd D, Bennett G, Coady S, D'Agostino R, Gibbons R et al. 2013 ACC/AHA Guideline on the Assessment of Cardiovascular Risk. A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2014;129(25 suppl 2):2935-2959.
- Folsom A, Yatsuya H, Nettleton J, Lutsey P, Cushman M, Rosamond W. Community Prevalence of Ideal Cardiovascular Health, by the American Heart Association Definition, and Relationship With Cardiovascular Disease Incidence. Journal of the American College of Cardiology. 2011;57(16):1690-1696.
- Smith S, Collins A, Ferrari R, Holmes D, Logstrup S, McGhie D et al. Our time: a call to save preventable death from cardiovascular disease (heart disease and stroke). European Heart Journal. 2012;33(23):2910-2916.
- James P, Oparil S, Carter B, Cushman W, Dennison-Himmelfarb C, Handler J et al. 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults. JAMA. 2014;311(5):507.
- Romero J, Wolf P. Epidemiology of Stroke: Legacy of the Framingham Heart Study. Global Heart. 2013;8(1):67-75.
- Mahmood S, Wang T. The Epidemiology of Congestive Heart Failure: Contributions from the Framingham Heart Study. Global Heart. 2013;8(1):77-82.
- 10 Palomaki G, Melillo S, Bradley L. Association Between 9p21 Genomic Markers and Heart Disease. JAMA. 2010;303(7):648-656.
- Yeboah J, McClelland R, Polonsky T, Burke G, Sibley C, O’Leary D et al. Comparison of Novel Risk Markers for Improvement in Cardiovascular Risk Assessment in Intermediate-Risk Individuals. JAMA. 2012;308(8):788.
- Corcoran M, McKay D, Blumberg J. Flavonoid basics: chemistry, sources, mechanisms of action, and safety. J Nutr Gerontol Geriatr. 2012;31(3):176-189.
- Sarriá B, Martínez-López S, Sierra-Cinos J, Garcia-Diz L, Goya L, Mateos R et al. Effects of bioactive constituents in functional cocoa products on cardiovascular health in humans. Food Chemistry. 2015;174:214-218.
- Wang Z, Nie Z, Zhou B, Lian X, Zhao H, Gao W et al. Flavonols intake and the risk of coronary heart disease: a meta-analysis of cohort studies. Atherosclerosis. 2012;222(1):270-273.
- Martinez-Augustin O, Aguilera C, Gil-Campos M, De-Medina F, Gil A. Bioactive Anti-Obesity Food Components. International Journal for Vitamin and Nutrition Research (2012). 2013;82:148-156.
- Go A, Mozaffarian D, Roger V, Benjamin E, Berry J, Borden W et al. Heart Disease and Stroke Statistics—2013 Update. Circulation; 2013 p. 146-245.
- Berry N, Davison K, Coates A, Buckley J, Howe P. Impact of cocoa flavanol consumption on blood pressure responsiveness to exercise. British Journal of Nutrition. 2010;103(10):1480-1484.
- Wong R, Howe P, Buckley J, Coates A, Kunz I, Berry N. Acute resveratrol supplementation improves flow-mediated dilatation in overweight/obese individuals with mildly elevated blood pressure. Nutrition, Metabolism and Cardiovascular Diseases. 2011;21(11):851-856.
- Widmer R, Freund M, Flammer A, Sexton J, Lennon R, Romani A et al. Beneficial effects of polyphenol-rich olive oil in patients with early atherosclerosis. European Journal of Nutrition. 2012;52(3):1223-1231.
- Militaru C, Donoiu I, Craciun A, Scorei I, Bulearca A, Scorei R. Oral resveratrol and calcium fructoborate supplementation in subjects with stable angina pectoris: Effects on lipid profiles, inflammation markers, and quality of life. Nutrition. 2013;29(1):178-183.
- Davison K, Berry N, Misan G, Coates A, Buckley J, Howe P. Dose-related effects of flavanol-rich cocoa on blood pressure. Journal of Human Hypertension. 2010;24(9):568-576.
- Hodgson J, Croft K. Tea flavonoids and cardiovascular health. Molecular Aspects of Medicine. 2010;31(6):495-502.
- 23 Khawaja O, Gaziano J, Djoussé L. Chocolate and Coronary Heart Disease: A Systematic Review. Current Atherosclerosis Reports. 2011;13(6):447-452.
- Liu Z, Ho S, Chen Y, Ho Y. The effects of isoflavones combined with soy protein on lipid profiles, C-reactive protein and cardiovascular risk among postmenopausal Chinese women. Nutrition, Metabolism and Cardiovascular Diseases. 2012;22(9):712-719.
- Johnson R, Bryant S, Huntley A. Green tea and green tea catechin extracts: An overview of the clinical evidence. Maturitas. 2012;73(4):280-287.
- Wang X, Ouyang Y, Liu J, Zhao G. Flavonoid intake and risk of CVD: a systematic review and meta-analysis of prospective cohort studies. British Journal of Nutrition. 2013;111(01):1-11.
- Sahebkar A. A systematic review and meta-analysis of randomized controlled trials investigating the effects of curcumin on blood lipid levels. Clinical Nutrition. 2014;33(3):406-414.
- Cicero A, Tartagni E, Ferroni A, De Sando V, Grandi E, Borghi C. Combined Nutraceutical Approach to Postmenopausal Syndrome and Vascular Remodeling Biomarkers. The Journal of Alternative and Complementary Medicine. 2013;19(6):582-587.
- Ras R, Zock P, Zebregs Y, Johnston N, Webb D, Draijer R. Effect of polyphenol-rich grape seed extract on ambulatory blood pressure in subjects with pre- and stage I hypertension. British Journal of Nutrition. 2013;110(12):2234-2241.
- Yubero N, Sanz-Buenhombre M, Guadarrama A, Villanueva S, Carrión J, Larrarte E et al. LDL cholesterol-lowering effects of grape extract used as a dietary supplement on healthy volunteers. International Journal of Food Sciences and Nutrition. 2012;64(4):400-406.
- Wang Z, Zhao D, Nie Z, Zhao H, Zhou B, Gao W et al. Flavonol intake and stroke risk: A meta-analysis of cohort studies. Nutrition. 2014;30(5):518-523.
- Hollman P, Geelen A, Kromhout D. Dietary Flavonol Intake May Lower Stroke Risk in Men and Women. Journal of Nutrition. 2010;140(3):600-604.
Take a deeper dive into Exploring the Impact and Prevention of Falls in the Elderly with our additional resources.



- 24/7 Customer Support
- 100% Customer Satisfaction
- No Privacy Violation
- Quick Services
- Subject Experts