Impact of Family Presence during Cardiopulmonary Resuscitation
Chapter 1 - Introduction:
The purpose of the dissertation is to look at the impact on family’s while being present during cardiopulmonary resuscitation (CPR) and how it may affect them to witness.There is increasing debate about the advantages and disadvantages of family-witnessed resuscitation, from the family and the impact it has on them (Paplanus et al., 2012). As CPR is a first aid technique when an individual’s heart has stopped beating, it makes you look at the damaging consequences for families to witness (Attin et al., 2016).This will be done by searching for relevant literature and critically critiquing it to find the effects it may have on the families surrounding the resuscitation. The overall structure of this dissertation will be organised into chapters. Chapter one will be introducing the topic, and it is important to clinical practice, Chapter two will be explaining the search strategy and how the literature was obtained. Chapter three will be reviewing the finale literature utilising a framework to critique it; chapter four will be outlining the recommendations that were found. Chapter five will look at the implications it may have on clinical practice; chapter six will summarise what has been found. If you need assistance with a healthcare dissertation help, feel free to reach out to us for getting expert guidance.
This project was conceived during the author learning about the topic for the first time while in clinical practice and hearing of witness resuscitation. Koberich (2018) states the controversially debated of witnessed CPR in the international nursing research agenda. From this, looking at the local policy and noticing that there was no policy published on family present during witnessed resuscitation or even a subheading in the resuscitation policy (Local Trust Policy (LTP), 2017). However, other trusts had their own policies, but did not obtain sufficient information to guide and adhere staff. Portanova et al. (2015) states that the public is becoming gradually more aware and educated on the options available to them and may see relatives request to witness resuscitation of their loved one. Input from media resources, e.g. internet, social media, television hospital dramas and factual television documentaries have exposed the public to the procedure of resuscitation and desensitising them to traumatic images which may also have contributed their expectation (Portanova et al., 2015).

Family Witnessed Resuscitation (FWR) is described in clinical practice when relatives can decide whether they wish to present while their loved one is resuscitated (Gray, 2002). Pratiwi (2017) also goes on to state family presence during resuscitation is defined as the presence of relatives in the area of patientcare where they can have a visual contact of the patient during resuscitation.The European resuscitation guidelines (2016) state that families should be allowed to be present during a CPR attempt in hospital, but consent must be obtained from the families and written in the medical notes, while a health professional is assigned to them to support and explained the procedures while they witness resuscitation. However, LTP (2017) outlines that FWR is not a new concept, but remains to be a controversial subject and see a divide between health care professionals on their views regarding FWRand the impact it will have on their loved ones (Royal College of Nursing (RCN), 2002). The rationale for FWR and be able to manage these situations sensitively and effectively and support any families who wish to witness resuscitation (Jabre et al., 2013).
In the 1960s, the closed-chest compressions are the initial method used for the treatment of patients who experienced cardiac arrest and this lead the first cardiac resuscitation (CPR) guidance to be published in 1966. The bystander CPR was introduced at first in 1976 in the advanced support life courses which then shortly led to the reports of the presence of family members during cardiac resuscitation (Ewy, 2018). The study by De Stefano et al. (2016) informs that physicians and nurses are against the presence of family members while performing CPR. This is because they believed that presence of distraught family member in the CPR room acts as a distraction for the health professionals and it may lead them to make mistake in performing the act leading patients to face danger. This is evident as the study by Kenny et al. (2017) which was randomised controlled trial where execution of CPR by student nurses was compared for patient under the presence and lack of family members. The findings in the study informed that nurses performed better CPR for patients under condition where no distressed family member was present in the scenario. However, the nurses applied less pressure on the chest during CPR in condition where distressed family members were patient. The study also informed that timing and pressure on the chest was effective when the CPR by the nurses were provided under the total lack of family members in the vicinity of the patient. Take a deeper dive into Tobacco Use and Health Consequences with our additional resources.
In comparison, some studies mentioned that physicians prefer the presence of family members during CPR in hospital settings. This is evident from the study by Lederman (2019) which mentions that presence of family member during the CPR process leads the physicians to prove that all possible actions are being performed by them to make the patients get back to life. This, in turn, leads the family members to avoid doubting the actions of health professionals done in regard to ensure life to the patient. The study by Brasel et al. (2016) informs that executing cardiac resuscitation behind closed doors leads the family members expect unrealistic efforts from the physicians to ensure life of the patients. However, the presence of family members during CPR leads the family members to understand the efforts being made as well as offers them the opportunity to bid the last goodbye to the patients and grasp reality regarding the death of the person helping them to avoid complicated or prolonged post-traumatic stress or pathological mourning in the bereavement process. Thus, it indicates that presence of family members during cardiac resuscitation for the patients created both advantages and disadvantages.
Dig deeper into Drug Misuse in UK Prisons with our selection of articles.
The Resuscitation UK (2010) wrote guidelines on how families should be present if their child needs CPR attempts; however, does not mention any guidelines or recommendations on adults. In additions to Resuscitation UK (2010) have now been rewritten in (2015) and have removed this section on FPDW and when contacted on any guidance on the subject, it stated it was rewriting the current guidelines and did not know when they would be available. However, other countries have guidance for FPDW including American Heart Association (2019) and in Northern Ireland where the Royal College of Nursing Institute (2013) which clearly state what is expected of health professional during this procedure and how to support the family present. Also, other part of the UK including Scotland and Wales, have their own guidance on FPDR, this can see growing concerns with the number of families wanting to be present and staff having no direction on how to make it a smooth transition and implication affecting the families from what they just witnessed. However, with the little published literature available on the impact on FWR and the research on the perspective of and experiences of family members who witnessed CPR, saw the context of this study being facilitated.
In this dissertation, a variety of definitions utilise throughout this systematic review are described below. Cardiopulmonary resuscitation or known as CPR will either facilitate chest compressions by either human hands or by a mechanical device to help restart the heart. As well as a defibrillator, and artificial respiration in an attempt to restart the heart (British Heart Foundation, 2012).The term family throughout this review will be focusing on the patient’s next of kin, which could be a partner or parent or a member of the immediate family if no next of kin is available. However, children in the family under the age of 16 is usually inappropriate during the resuscitation, and only in exceptional circumstances, the number of relatives should not exceed two (Local Trust Policy, 2017). Finally, the term resuscitation is also used to cover a wide range of events in the area hospital setting, including fluid replacement, trauma, respiratory or cardiac problems (RCN 2002).
Throughout this dissertation, trust policies will be referred to as Local Trust to remain confidential and not breach the Data Protection Act (2018), while working aligned with the Nursing and Midwifery Council (NMC) (2018) the code on confidentially.
In this dissertation, there will be a slight use of abbreviation to used to refer to specific nursing and clinical terms: Family Witnessed Resuscitation- FWR; Family Present During Resuscitation- FPDR; Nursing and Midwifery Council – NMC; Cardiopulmonary Resuscitation – CPR; Local Trust Policy- LTP; Royal College of Nursing- RCN.
Chapter 2 - Literature search strategy:
The study employed a comprehensive literature search utilising the university academics electronic database to help obtain more considerable nursing literature and appropriate for identifying directly related to FPDR in clinical area. The search was conducted between October 1st – 20th October 2019. The electronic search is essential to be executed as the online databases are seen to have diverse and current information regarding any topic to help in executing the study in successful manner (Dunn et al. 2018). The search platform which is mainly considered in executing the study is CINHAL but the others such as MEDLINE, Cochrane Library, google scholar,Wiley and PubMED was used in collecting information by using the search terms determined.
The research question in the study is formulated by using PICO tool. The PICO framework is mainly used in evidence-based studies to develop the research question by enquiring the topic of the study in details (Milner and Cosme, 2017). This is because it leads to the development of a clarified research question which helps the researchers to understand the facts to be collected to resolve the raised problem in the study. The PICO framework stands for Population, Intervention, Comparison and Outcome. The population indicates the target individuals who are to be considered for the study. The Intervention is referred to the determined actions to be assessed by the research in the study. The comparison is referred to the target group with whom the intervention is to be juxtaposed in relation to the target population of the study. The outcome is referred to as the results to be derived from the study (Torquati et al. 2017).
The keywords to be implemented in the study for searching information related to the raised research question is significant to be identified so that proper information can be collected through the electronic search. The keywords to be used in searching information include “Family members”, “Relatives”, “Parents”, “Impact of family members on Cardiopulmonary Resuscitation”, “cardiac arrest”, “impact of relatives presence during CPR “ and others. The Boolean operators such as “And” “Or” are to be used for connecting the key words to develop a proper search for collecting required information.
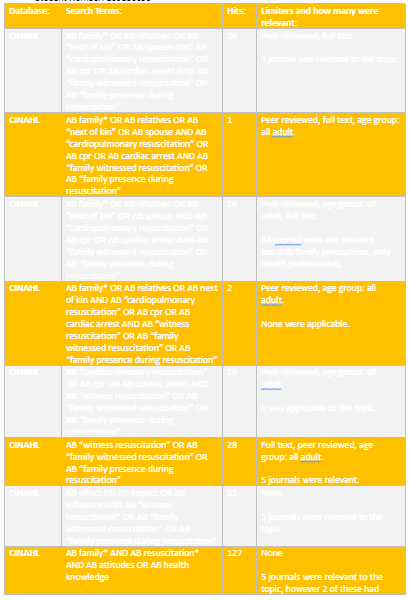
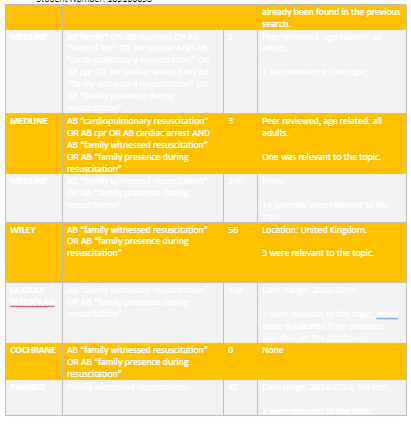
On searching for the literature articles saw very limited journals being retrieved from there not being a lot of research being facilitated on the subject. There was plenty of research on the perception on medical staff on their thorough and feeling on witness resuscitation but limited on the family’s point of view. Below is a table of the hit number of the different words used to facilitate the search and how many hits were found. Below is a table of the searches and the results that were obtained.
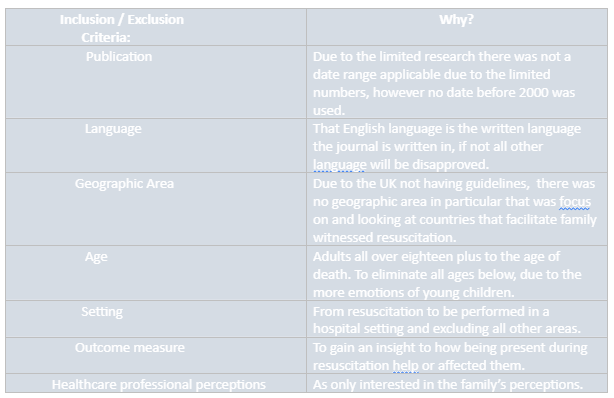
The inclusion criteria inform the characteristics which are to be considered to perform the study and the exclusion criteria are the factors that are to be avoided by the researchers to be considered in performing the study as it would lead to raise error (Doolen et al. 2016). The inclusion criteria of the study include journals that are not published before 2000, articles written in English language, participants above 18 years of age, cardiac resuscitation performed in hospital settings in the presence of the family members. The exclusion criteria include journals and articles that are written before 2000, participants below 18 years of age, journals not written in English language, cardiac resuscitation not performed in the presence of the family in the hospital settings. The journals published after 2000 to till date are included and other excluded as it would help the researcher collect most updated information regarding the topic, in turn, assisting them to avoid backdated data. The studies written in English are considered and other excluded because the researchers only have knowledge regarding the English language and therefore they are unable to derive proper information through translation of journals written in other languages. The participants who are above 18 years of age are considered and other excluded as the emotional feelings of the children may result to report hindered results that may lead to raise error in the study. The journals which focussed on cardiac resuscitation done in presence of family members in the hospital settings are to be considered as it would help to provide enriched and relevant information in the study.
The remaining full-text studies were independently reviewed by hand reading the abstracts of the articles to make sure they fit with the method of this current study in line with the inclusion criteria previously described. By evaluating the articles found from observing the titles and abstracts, a second stage was done by filtering out any irrelevant articles, by reading the full articles. Also, systematically choosing the articles that met the predetermined criteria above (Torgerson, 2003). As well as not excluding any quantitative research relevant to the topic because the author did not like the researcher approach as wanting to obtain thought and feeling and not looking at numerical data. Also, making sure a non-bias approach was taken, this saw . . . . . . . . .journal articles were narrowed down that mainly focus was on the impact of family members witnessing CPR and their opinions.Additionally, making sure all the . . . . . .journal articles were secondary research to help with using that involvesexisting data and summarising and collating to increase the overall effectiveness of research (Heaton, 2008). Also, making sure the articles were from different literature sources to have well-balanced research selections and making sure they were robust sources. Below is a table of the journal articles picked to be critically analysed.
Chapter 3 - Literature Review:
By appraising the quality of the research found, it allows to see the different findings from the results exploring the subject. To critique the evidence there are several assessment tools to utilise, these are; Critical Appraisal Skill Programme (CASP) (2018), McMaster (1998), Newcastle-Ottawa Scale (NOS) (2019) and Caldwell et al. (2011). All assessment tools will be used to help critical appraise the evidence.

References:
- Attin, M., Tucker, R., Carey, M. (2016) In-hospital cardiac arrest:An update on pulseless electrical activity and asystole. Critical Care Nursing Clinics of North America, 28(3), 387-397.
- Begley, A., and Blackwood, B. (2000) Truth telling versus hope: a dilemma in practice. Int Journal Nursing Practice, 6, 26-31.
- Caldwell, K., Henshaw, L., and Taylor, G. (2011) Developing a framework for critiquing health research: An early evaluation. Nurse Education Today, 31(8): pp. 7.
- Colwill, M., Somerville, C., Lindberg, E., Williams, C., Bryan, J., & Welman, T. (2018). Cardiopulmonary resuscitation on television: Are we miseducating the public? Postgraduate Medical Journal, 94(1108), 71–75.
- De Stefano, C., Normand, D., Jabre, P., Azoulay, E., Kentish‐Barnes, N., Lapostolle, F., & Adnet, F. (2016). Family presence during resuscitation: A qualitative analysis from a national multicenter randomized clinical trial. PLoS ONE, 11(6).
- Gray, A. (2002) ‘The advanced nurse practitioner: empowerment in witnessed resuscitation’. In Barrtter, K. Ethical Issues In Advanced Nursing Practice. Edinburgh: Elsevier Science Limited, pp101-110.
- Heaton, J. (2008) Secondary analysis of qualitative data: An overview. Historical SocialResearch/Historische Sozialforschung, pp.33-45
- Jabre, P., Belpomme, V., Azoulay, E., Jacob, L., Bertrand, L., Lapostolle, F., Tazarourte, K., Bouilleau, G., Pinaud, V., Broche, C. and Normand, D. (2013) Family presence during cardiopulmonary resuscitation. New England Journal of Medicine, 368(11), pp.1008-1018.
- Koberich, S. (2018) Witnessing resuscitation: A call for a research agenda. European Journal of Cardiovascular Nursing, 17(2), 100-101.
- Local Trust Policy. (2017)Family Witnessed Resuscitation.
- Local Trust Policy. (2018) Resuscitation Policy.
- Monks, J., and Flynn, M. (2014) Care, compassion and competence in critical care: A qualitative exploration of nurses’ experience of family witnessed resuscitation. Intensive and Critical Care Nursing, 30(1), 353-359.
- Nolan, J. P., Soar, J., Smith, G. B., Gwinnutt, C., Parrott, F., Power, S., & Rowan, K. (2014). Incidence and outcome of in‐hospital cardiac arrest in the United Kingdom National Cardiac Arrest Audit. Resuscitation, 85(8), 987–992.
- Paplanus, L. M., Salmond, S. W., Jadotte, Y. T., & Viera, D. L. (2012). A systematic review of family witnessed resuscitation and family witnessed invasive procedures in adults in hospital settings internationally–Part I: Perspectives of patients and families. The JBI Database of Systematic Reviews and Implementation Reports, 10(32), 1883–2017.
- Portanova, J., Irvine, K., Yi, J. Y., & Enguidanos, S. (2015). It isn't like this on TV: Revisiting CPR survival rates depicted on popular TV shows. Resuscitation, 96, 148–150.
- Pratiwi, I, D. (2017) Family presence during resuscitation: patient and family members’ preferences and attitudes. International Journal of Research in Medical Science; 6(2), pp. 394-400.
- Royal College of Nursing. (2002) Witnessing Resuscitation: Guidance for Nursing Staff. London: Royal College of Nursing.
- Royal College of Nursing Institute. (2013) Family-centred care during resuscitation events. Northern Ireland: Royal College of Nursing Institute.
- Resuscitation UK. (2010)
- Sandroni, C., Nolan, J. P., Cavallaro, F., & Antonelli, F. (2007). In‐hospital cardiac arrest: Incidence, prognosis and possible measures to improve survival. Intensive Care Medicine, 33(2), 237–245.
- Torgerson, C. (2003)Systematic Reviews. London: Continuum.
- Toronto, C, E., and LaRocco, S, A. (2018) Family Perception of and experience wit family presence during cardiopulmonary resuscitation: An integrative review. Journal of Clinical Nursing, 28(32): pp. 32-46.
- Ewy, G.A., 2018. The mechanism of blood flow during chest compressions for cardiac arrest is probably influenced by the patient's chest configuration. Acute medicine & surgery, 5(3), pp.236-240.
- Kenny, G., Bray, I., Pontin, D., Jefferies, R. and Albarran, J., 2017. A randomised controlled trial of student nurse performance of cardiopulmonary resuscitation in a simulated family-witnessed resuscitation scenario. Nurse education in practice, 24, pp.21-26.
- De Stefano, C., Normand, D., Jabre, P., Azoulay, E., Kentish-Barnes, N., Lapostolle, F., Baubet, T., Reuter, P.G., Javaud, N., Borron, S.W. and Vicaut, E., 2016. Family presence during resuscitation: a qualitative analysis from a national multicenter randomized clinical trial. PloS one, 11(6). pp.29-45.
- Lederman, Z., 2019. Family Presence During Cardiopulmonary Resuscitation. The Journal of clinical ethics, 30(4), p.347.
- Brasel, K.J., Entwistle, J.W. and Sade, R.M., 2016. Should family presence be allowed during cardiopulmonary resuscitation?. The Annals of thoracic surgery, 102(5), pp.1438-1443.
- Dunn, H., Quinn, L., Corbridge, S.J., Eldeirawi, K., Kapella, M. and Collins, E.G., 2018. Cluster analysis in nursing research: an introduction, historical perspective, and future directions. Western journal of nursing research, 40(11), pp.1658-1676.
- Milner, K.A. and Cosme, S., 2017. The PICO Game: An Innovative Strategy for Teaching Step 1 in Evidence‐Based Practice. Worldviews on Evidence‐Based Nursing, 14(6), pp.514-516.
- Torquati, L., Pavey, T., Kolbe-Alexander, T. and Leveritt, M., 2017. Promoting diet and physical activity in nurses: a systematic review. American Journal of Health Promotion, 31(1), pp.19-27.
- Doolen, J., Mariani, B., Atz, T., Horsley, T.L., O'Rourke, J., McAfee, K. and Cross, C.L., 2016. High-fidelity simulation in undergraduate nursing education: A review of simulation reviews. Clinical Simulation in Nursing, 12(7), pp.290-302.
Bibliography:
- Booth, M, G., Woolrich, L., Kinsella, J. (2004) Family witnessed resuscitation in UK emergency departments: a survey of practice. European Journal of Anaesthesiology, 21, 725-728.
- Bourgeault, I., Dingwall, R., De Vires, R. (2010) The sage handbook of qualitative methods in health research. London: Sage Publication.
- Fiori, M., Endacott, R., Latour, J, M. (2018) Exploring patients’ and healthcare professionals’ experiences of patient-witnessed resuscitation: A qualitative study protocol. Advance Nursing Journals, 75, 205-214.
- Sak-Dankosky, N., Andruszkiewicz, P., Sherwood, P, R. Kvist, T. (2019) Preferences of patients’ family-witnessed cardiopulmonary resuscitation: A qualitative perspective of intensive care patients’ family members. Intensive and Critical Care Nursing, 50(1), 95-102.
Continue your exploration of Government Cuts and Older People's Health in the UK with our related content.



- 24/7 Customer Support
- 100% Customer Satisfaction
- No Privacy Violation
- Quick Services
- Subject Experts