Impact of Junior Doctors Industrial Action on UK Healthcare System
Introduction
Doctors are considered to be the most important individuals in society through which scientific understanding is communicated. They are the individuals who are licensed and authorized to diagnose a patient, prescribe medications for people suffering from various ailments and this involves the summation of knowledge regarding medicines and experiences in the clinical field. When the doctors diagnose a patient suffering from any illness they consider both the mental and physical health of the patients. They are referred as the clinical scientist who applies the principles and the procedures of medicines for the prevention of disease and to offer care to the critically ill patients and also to restore the condition of mental and the physical health (Working Party of the Royal College of Physicians, 2005). Therefore, they are the individuals who take the responsibility of keeping a community healthy by working in a multidisciplinary team (Working Party of the Royal College of Physicians, 2005). A junior doctor is any medical graduate who is still in the training procedure and is not authorized to practice independently without any supervision (Prince, et al, 2004). They are the individuals who play a key role in the accident and emergency department (A&E) (Prince, et al, 2004). It had been noticed several times that the resident doctors called for strikes because of varied reasons such as the concerning the safety issues at the workplace, for better conditions related to work and workplace, better pay structure and against different policies such as the reservation of bed based on caste and appointments to any position of the institute. In variwhich countriesous countries such as India, United States, Israel, Spain, South Africa, the doctors are also threatened to call for a strike to protect against the rising violence against them (Metcalfe, et al, 2015; Ogunbanjo, et al, 2009; Selemogo, 2014). If you are seeking healthcare dissertation help, then our team is there to provide expert guidance and support to help you achieve academic success.

The approach of predominantly capitation system in the United Kingdom has several associated problems. The positive side of the capitation system is that it has the efficiency to give confidence to the doctors to compete for patients which are based on the quality of care services provided by them and also by attracting the patients, the income of the doctor increases (Chen, et al, 2010). But the approach also depends on the capability of the patient to monitor the care which can be considered as a questionable assumption. Due to this perceived problem of the capitation system, the government of the United Kingdom have initiated a range of financial incentives which in turn encourages the primary physicians to fulfil the objectives assigned by the Public Health (Chen, et al, 2010). The alternative to the capitation system is the involvement of salaried employment. Therefore the payment structures often impact the working efficiency of the doctors which forced them to protest against the system. Due to the ethics and responsibility of the profession of the doctors, they often are required to give their services at the unfriendly working hours which affect their social, mental and their physical status. The major effect of the prolonged working hours are stress, poor balance in the work-life, lack of free time and several health associated risks in the future (Gosden, et al, 1999; Poissonnet, et al, 2000). Several authors had studied the impact of strike upon the inpatient, outpatient and emergency services of various hospitals all over the globe. In the time of meeting conducted by the American Heart Association and the American College of Cardiology, a noteworthy fall had been observed in the 30 days mortality among the patients who were categorised as high risk due to the associated problems of heart attack and cardiac failure(Sedlis, 2009; American Heart Association, 2014). Therefore, it was very important to study the impact of the strike called by the junior doctors of the United Kingdom during 2016 which will highlight the issues of staff shortages, limitation observed in the national response and also to evaluate the efficiency of the healthcare system (Jena, et al, 2015). The impact of the strike called by the junior doctors of England in 2016 was found to be massive during the end period of the industrial action as at that time the doctors also withdrew the emergency care services. The first four months of the strike in the year 2016 involved the participation of the doctors from all the specialities all over England with a span of 24 – 48 hours which culminated up to 2 days. They had participated in that industrial action due to the amendment of few modifications in the contract as imposed by the Department of Health, Government which according to the doctors would result in poor patient care service in the future (Furnivall, et al, 2018).
Continue your exploration of Homelessness on Access to Primary Care with our related content.
To evaluate the impact of the strike, data were retrieved from the national hospital administrative database for England’s National Health Service (NHS) and Hospital Episode Statistics (HES) by the authors who conducted studies on the topic before (Ruiz, et al, 2013; Furnivall, et al, 2018). Then the data were compared with the week of the strike with the week immediately previous and after it. Therefore the data allowed the researchers to investigate about the trends in the number of admissions which included inpatients and outpatients, the number of cancelled appointments for the outpatients, the attendances observed at the department of accident and emergency (A&E), the mortality rate of the in-hospital patients during the period of strike and finally all the data was compared with the numbers expected depending on the normal or non-strike conditions. The patients admitted were categorised into the emergency and elective categories by the application of “admimeth” process of admission in the HES. To obtain the rate of in-hospital mortality the discharge method field or “dismeth” had been applied. The attendances at the A&E department were determined by the A&E attendance disposal field (‘aeattenddisp’) and the method had also highlighted the number of deaths within that particular department. The outpatient data of the HES could not be used to record deaths during the time of appointment, so that data was not included within the study. Then the data were analysed using the regional analyses by the application of provider code data (‘procode’) (Furnivall, et al, 2018).
Therefore, the present study conducted a traditional literature review which is the all-inclusive, decisive and objective analysis of the existing knowledge on the topic. The literature review is considered to be an essential part of the research process which guides the researchers to determine a theoretical framework also highlights the context of the present study. It can be also termed as a qualitative systemic review (Machi, et al, 2016). The significance of the literature reviews are it elaborates how the present study is related to the statistics highlighted in the prior research, it also focuses on the novelty and relevance of the problem in the research and also justifies the proposed methodology adopted for the study (Machi, et al, 2016) It also guides the researchers to identify the gaps in the existing literature, the conflicts mentioned by the other authors in the previous studies and allows the researchers to address the open questions from the other researchers (Rhoades, 2011). Therefore, the concept of evidence-based practice is considered to be significant to offer the most effective care to the patient and in terms of the outcome of the health care service. The term “evidence-based practice” or EBP can be defined as the best possible use of the current research while making decision concerning the individualised patient care. As patients are expected to receive the best possible care which depends on the existing pieces of evidence available. EBP in nursing practice is also considered to be important as because it guides the nurses to evaluate the research and can estimate the risk or effectiveness of the treatment procedure or the care plan and the diagnostic tests. The implementation and development of EBP are stimulated by the constant rise in the professional and public demand which results in the improvement of safety and quality in the health care service. As EBP combines the existing pieces of evidence in research along with the clinical expertise, this process promotes the individualised care with the inclusion of the opinions and preferences of patients (Melnyk, et al, 2011). The EBP involves the five “A” as the critical steps: Ask the clinical question that has to be answered; Acquire the best evidences to answer the question; Appraise the existing evidences critically to evaluate the validity, relevance and applicability; Apply the evidences and the critical expertise along with the opinions and values of the patient; Assess is considered to be the final step to measure the usefulness of the above mentioned four steps and also evaluate ways to develop the above four steps (Portney, 2020; Melnyk, et al, 2011).
According to the findings of the descriptive retrospective study conducted by the researchers, the strike had an immense impact on the health care service and the quality of the patient care provided during that period as thousands of appointments got cancelled, the huge number of junior doctors did not turn up for providing any patient service, many unattended appointments which could have endangered the life of many patients (Furnivall, et al, 2018).
The study included the role of junior doctors, the definitive causes behind the strike called the English junior doctors in the year, 2016 and the potential impact of the strike on the overall health care services of the United Kingdom. Therefore, to help develop a relevant strategy to manage the strike and to prevent the impact of it on patient care, this study aims to explore the causes of the junior doctor’s strike in England in the year, 2016. One of the limitations of the above-mentioned study conducted by the researchers were they did not highlight the financial modelling concerning the impact of the industrial action both on the regional and national level. Another one was that the researchers could not examine the impact of industrial action on the health of those patients who failed to attend the hospitals. The study also did not include the qualitative analysis of the inconveniences and disappointments (Furnivall, et al, 2018; Rimmer, 2018; Toynbee, et al, 2016).
Research Questions
What were the causes behind the strike called by junior doctors in the United Kingdom in the year 2016?
What were the impacts observed on the patient care service due to the strike?
Search and Selection (Method)
Several high impact peer-reviewed journals had been studied via comprehensive search method and the approach for the evaluation of the literature review had been implemented. Following steps were followed in the methodology section of the study to conduct a systemic review:
Recognizing the research question
The research question was raised using the PICO framework. The P denotes the study population, I denotes Intervention and C denotes comparison and O denotes Outcome.
P (Population): Junior Doctors
Intervention: Industrial action called by junior doctors of the UK in the year 2016
Comparison: Other Industrial actions called by physicians all over the world
Outcome: Impact on patient care services (Melnyk, et al, 2011).
The study was conducted with a broad definition for the study population, results, interventions so that a detailed coverage can be obtained in the search strategy with the
clearly defined concept was maintained which could be continuously refined based on the number of references and scope, parameters are set (Melnyk, et al, 2011).
Selection of the relevant works of literature
Primary studies (including both published data and unpublished studies are included) and reviews were selected based on the best understanding of the central research question. Therefore, a strategy was adopted where research evidence was searched from different sources. Suitable sources were identified after reviewing multiple electronic databases which comprises a huge number of high impact peer review contents such as PubMed, Google Scholar, Medline, Taylor, Karger, Plos-One and Francis Online., Grey literature databases, utilised by the researcher for searching scientific contents were GreyNet International, Open Grey and Med Nar. The search was done with restriction to the most updated contents up to the year 2019 so that relevant and latest content could be available for the literature review purpose. One particular limitation was faced by the researcher was the non-availability of the full-length document apart from the abstract due to the registration service particulars of the University. All the in-text references of the resulted papers were also reviewed to analyse and evaluate the content of the relevant databases ((Machi, et al, 2016; Randolph, 2009)
Study selection
The inclusion and exclusion criteria were developed once the research idea becomes familiar with the literature search. To define the inclusion criteria the title of the article and abstract should contain the keywords or the definite search item. Relevant search was done to match the requisite of research question though it might not contain the keywords or the search items within the title or abstract of the articles. To define the exclusion criteria, any studies that were falling “out of scope” for the review and not matching with the set research questions were not considered. Any literatures not written in the English language were not considered for the review purpose. Therefore all the pieces of literature based on the defined inclusion and exclusion criteria were considered for the literature review.

Keywords
Junior doctors, strike, United Kingdom, the year 2016, inpatient service, outpatient service, department of accident and emergency (A&E), cancelled appointments, hospital admission or consultant episodes, the mortality rate of the in-hospital patients, consequences of the strike.
Search outcomes
Good research employs the following steps while conducting the research study: systemic planning, a time-based approach has been adopted and setting realistic objectives.
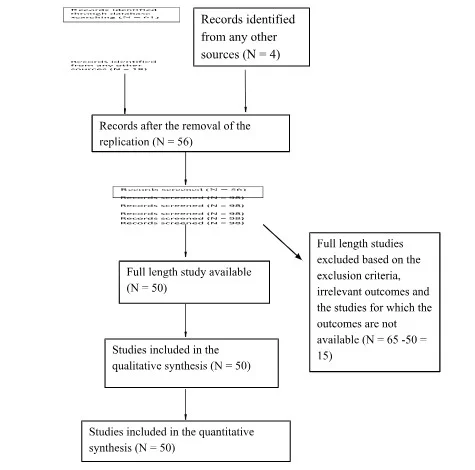
It is done by applying systematic method processes such as critical appraisal research studies, analysis of the secondary data, and the data that had been produced quantitatively and qualitatively (Saunders, et al, 2018). This particular approach had been used to obtain a detailed and exhaustive analysis of all the available kinds of literature on the electronic databases based on the inclusion criteria. The benefits associated with this method of is that it applies analytical and scientific methods for identifying and selecting the research which in turn reduces any form of bias in the study along with the productions of accurate and reliable results and conclusions concerning the research questions of the study. Therefore the researcher has to be very attentive while compiling the results from a wide range of studies to ensure the accurate validity of the results. The title of the research articles should match with the research questions and this ensures the accuracy of the abstract that has to be studied. All the pieces of evidence were included in the PRISMA flowchart in terms of retrieved, included and excluded studies (Lewis, et al, 2019; Liberati, et al, 2009).
Data Analysis
For the present study, the data analysis was done based on the Critical Appraisal Skill Programme (CASP) to ensure qualitative research. This particular tool helps to conduct critical analysis in a wide variety of settings which includes public health. The critical analysis framework is used to determine the quality of each study and to enable you to identify the strengths and weaknesses of each paper.This particular quality appraisal tool is used to analyse the Randomised Controlled Trials (RCT), Systematic Reviews, Case-Control Studies, Cohort Studies, Economic Evaluations, Qualitative studies, Diagnostic Studies, and Clinical Prediction Rule. There is a separate checklist which consist of about 10 -12 questions are available for these studies.. The appraising section of the tool focuses mainly on the validity and reliability of the scientific papers, the significance of the outcome and the application of the findings to the concerned research project (Singh, 2013). The section that deals with the “acting on the evidence” focuses on the application of the data findings to our research hypothesis, thinking about the practicality of the issues which may affect our study. The patient-centred study is also explained and provides evidence to explore that context of the research topic (Singh, 2013).
Literature Review
The expected professional roles of the junior doctors residing in the United Kingdom are categorised by the regulatory body named as General Medical Council (GMC) (Illing, et al, 2008). The activities and the curricular outcomes are prepared for the graduates who are in the beginning of their work-life and are expecting eligibility for full registration, i.e., to get the permit of practising without any supervision after completion of the first year of post-graduation (Monrouxe, et al, 2017; Tso, et al, 2014). These documents have been initiated after consulting with the stakeholders and pragmatic researchers for preparing the graduates to practice in the real world setting, and therefore the curriculum has been prepared in that manner (Illing, et al, 2008; Monrouxe, et al, 2015). However, the basic question about their role and what they are performing has not been highlighted directly (Monrouxe, et al, 2018; Burford, et al, 2014). To ensure a safe and supportive workplace for the graduates, it is very crucial to understand the detailing of the job that they are going to perform in the urban workplace and the essential factors that have to be considered to shape them for that practice. Unfortunately, very few researches had been conducted to investigate the matters methodically about the specified role of the routine doctors and how it is going to develop with time.
The findings obtained from the scientific communications have highlighted about the aspects that should be practised rather than what is in practice such as memorable ‘firsts’ besides handling tough clinical situations (Lefroy, et al, 2017; O'Halloran, et al, 1999; Lundin, et al, 2018). The authors of the studies had stated that three categories of firsts/ outcomes were identified: firsts that were envisioned and purposely arranged for in clinical school; firsts for which aggregate earlier readiness is beyond the realm of imagination because of the progression change in obligation between the understudy and specialist personalities, and firsts that spoke to encounters of disappointment. Accommodating intercessions in planning (setting) were open doors for practice and being given obligation as an understudy in the clinical group. Building self-adequacy for assignments was a significant strategy. During progress, the key relevant factor was the arrangement of fitting help from colleagues.Transition is a stage change in duty regarding which complete readiness isn't reachable. This progress is experienced as a soul changing experience when the recently qualified specialist first settles on choices alone (Lefroy, et al, 2017). The other study conducted by O'Halloran, et al, 1999 stated that different tasks should be identified for the work of preregistration house officers to provide the ground for their self evaluation. . Tipping, et al, (2010) and Boex, et al, 2003). examined the number of hours used up on work-related activities and their apparent value of education.There was a lot of difference in the methodologies adopted for the study conducted by Tipping, et al, (2010) and Boex, et al, 2003)such as categorising the activities broadly by employing several definitions, the detailing of the definite tasks performed, the exact reasons behind their execution, all these factors could not be properly examined or evaluated (Block, et al, 2013; Westbrook, et al, 2008). The use of the term “junior doctor” can be considered to be a little deceptive. Junior doctors include those doctors who have just completed their graduation from the medical school and also those doctors who have experience of more than a decade on the front line (Vance, et al, 2019). According to the study report, the starting salary of a junior doctor in the United Kingdom was nearly £23,000 per year and if the extra payments for the situations such as distant hours were taken into consideration then the salary could be easily up to £30,000. The junior doctors present at the top of the scale could easily earn up to £70,000 or excess (Martin Roland, 2004). These doctors perform the most important tasks such as decisions regarding the life and death situations of every patient and carry out crucial surgeries (Furnivall, et al, 2018; Vance, et al, 2019).
A retrospective analysis of the industrial action of the English junior doctors in the year, 2016 were done for the first time to evaluate the impact of the above-mentioned action on the in-hospital emergency services (Furnivall, et al, 2018). The study included the care of admitted patients, the accident and emergency services (A&E department) and the activity concerning the outpatient of all the hospitals of England for the evaluation purpose. According to Furnivall, et al, (2016), junior doctors of all specialities all over England went for a strike in the first four months (12th January, 10th February, 9–10th March and 26–27th April, not including the weekends) of the year 2016, to protest against the changes mentioned in the contracts imposed by the government which they thought would be harmful to patient care service in the long run. The results of the above mentioned study highlighted that there were 3.4 million numbers of admissions, the outpatient appointments were about 27 million and the attendance for over the four 3 weeks at the A&E department was 3.4 million. The patients admitted were categorised into the emergency and elective categories by the application of “admimeth” process of admission in the HES. To obtain the rate of in-hospital mortality the discharge method field or “dismeth” had been applied. The attendances at the A&E department were determined by the A&E attendance disposal field (‘aeattenddisp’) and the method had also highlighted the number of deaths within that particular department.
The outpatient data of the HES could not be used to record deaths during the time of appointment, so that data was not included within the study. Then the data were analysed using the regional analyses by the application of provider code data (‘procode’). In details the outpatients were categorised into the following categories:
0: Not applicable; 2: the appointment cancelled by the patient; 3: did not attend the appointment, no prior intimation; 4: the appointment was cancelled by the healthcare provider; 5: had attended the appointment on time; 6: arrived late but was attended by the care professional; 7: arrived late and was also not attended; 9: not known.
The authors of the study also highlighted about the exclusion of the impact of the industrial action on the financial model of the nation and regional services as one of the limitations (Furnivall, et al, 2018; Toynbee, et al, 2016).
The reason behind the strike
They demanded about 13.5 per cent hike in their basic pay structure on an average. But the hike of the salary would have to be compensated with other factors such as the other constituent of the salary structure would be curtailed which would also include the unfriendly hours. The working hours of the day on Saturday would be remunerated at a usual rate and the additional payments structured for the night hours and the rest of the hours of the weekend are comparatively lower than the current payment rates. The guaranteed increment in the payment which was associated with the working hours of the job had been fragmented and substituted by a system linked up with the development process via definite training stages. As a result of these amendments, the doctors had to work for more number of weekends to gain the extra payment as per the contract modifications. Moreover, certain modifications would need time to bring an effect to the existing system. This can be considered with the example of the amendment that the hike in the payment of the doctors which had been associated with the “time in the job” would result in a very slow rise in the income during their career as a junior medic (Thorn, et al, 2016). Moreover, the doctors who would have recently joined NHS as their starting career under the modified contract should suffer severely in comparison to those who had joined under the existing deal. According to the existing report, the Health Minister also argued about the fact that he wanted to develop the patient care service on Saturdays and Sundays. This was due to the reasons that as per the data available through research the patients who got admitted at the hospitals during the weekends were more likely to die and suffer than on the other days. This statement was supported with the evidence-based on the study reported at the British Medical Journal in September, that those patients admitted on Saturdays showed nearly 10 per cent higher risk of death and those on Sundays had 15 per cent higher risk of death in comparison to those patients who got admitted on Wednesday. In response to the study and its statements, the doctors had responded with the suggestion that the situation could be effectively controlled and avoidable by increasing the number of specialized manpower. Research reports also stated that those patients who got admitted at the weekend appeared to be sick in comparison to those who got admitted on other days and the researchers also could not give any clear statement that whether junior doctors could be accounted for the purpose. Though they had lifted tough questions regarding the quality of the service provided during the weekend, many researchers also reported about the work role of senior medics and consultants rather than the junior doctors only. According to the news, there had been only one strike in the past 40 years and that has taken place in the year 2012. The span of each of the four strikes is about 24 to 48 hours respectively, and the dates were 12th of January, 10th of February, 9-10th of March and 26-27th of April. The last strike was the only strike when the emergency care service had been withdrawn. Few hospitals also reported that near about 90% of the junior doctors populations refused to provide service in between 8 am to 5 pm to boost their strike against the modified contract formulated by Jeremy Richard Streynsham Hunt, a politician of British origin, who worked as the Member of the Parliament (MP) in the South West Surrey since 2005 (McKay, et al, 2016; Rich, et al, 2016).
Effects of the strike of junior doctors on patient care service
As a result, inconsistency appeared while providing effective routine care and this created an opportunity to investigate the effectiveness of the current system which focussed about the weakness developed in response to staff shortages. Therefore, researches were conducted to compare the activity of the hospital of the week during the time of the following strikes with that of the preceding weeks. The following categories were evaluated to assess the outcome of the strike on patient care availability: outdoor patient appointment, number of new admissions and the attendance in the A&E department. It was observed after evaluation of 12 weeks of study that there were around 3.4 million admissions, outpatient appointments were up to 27 million and attendance at A&E department was of 3.4 million. When the data were compared with the preceding week's data, it was observed that there was 9 per cent reduction in the number of admissions (31,651), about 7 per cent reduction at the A&E department (23,895) and nearly 6 per cent reductions in the number of outpatient appointments (173,462) than the expected value. The strike that was held in April had a greater impact on the patient care service as evident from the available data: about 15 per cent reductions in the number of admissions (18,194) which included nearly 8 per cent reduction in the number of emergency admissions (3383) and 20 per cent reductions in the number of planned admissions. Most of the hospitals managed well and did not experience any severe problems as the duties of junior doctors were taken up by the senior physicians at that time of crisis (McKay, et al, 2016). However, the A&E department was appeared to be more quiet than usual as patients suffering from minor illness did not turn up as per the warnings issued by NHS. It was also observed that there was 11 per cent reduction (109,915) in the number of outdoor patient appointment during the time of the strike and the numbers of patients were slightly greater than 17% (134,711). Moreover, the number of appointments of the outdoor patients cancelled by the hospital got increased by 67 per cent, i.e., 43,823. Overall the numbers of cancelled appointments of the outdoor patients were about 300,000 which is nearly 52% higher than the number expected for the period of the strike. The reason that may have contributed to the number as identified by the researchers is to provide service to severe critical patients. The impact of the strike was not the same everywhere within the United Kingdom as several regions were unduly affected. The ratio of the number of appointments cancelled in South East Coast, Yorkshire, Humber and London had increased to 66 – 68 per cent and this region also had the highest number of missed appointments (Furnivall, et al, 2018). The effect observed on the emergency admission section was smaller in comparison to the West Midlands and the South West where the impact was much more. Moreover, the number of deaths recorded during the period of the strike was not that significant and was not even higher than the expected value (Bray, et al, 2017; Furnivall, et al, 2018). The strike that happened on 26th -27th April 2016 had an impact upon the emergency services although no considerable increase in the mortality rate was observed during the period of the strike. Concerning this context, according to the researchers, the mortality rate of the hospital is considered to be the least insightful outcome to assess the quality and safety concerns. The reason behind the above statement is that death occurring due to bad quality of patient care service does not get exposed immediately and the reasons behind the worsening condition of patient health such as delayed appointments and procedures were also not clear as explained by the researchers. Therefore, these issues along with the monetary problem can be considered as an interesting subject for researching future. Another important aspect mentioned by the researchers that they did not assess the effect of the strike on patients who failed to attend the A&E department and the probable impact of the “weekend effect” on the patient who got their care service delayed (McKay, et al, 2016; Rich, et al, 2016; Furnivall, et al, 2018; Bray, et al, 2017).
Several other researchers had conducted studies about the impact of the strike of the doctors in the United States of America, Israel, Spain, South Africa, India, Croatia and the United Kingdom. None of the study they had reviewed showed any effect on the mortality rate during the time of strike except one strike that took place at South Africa, in the year, 2010 for a prolonged duration of 20 days reported a high mortality rate of about 67% at the emergency department which was much higher in comparison to the normal period (Metcalfe, et al, 2015). A total of 156 trust service related to different acute hospitals of England did not report any incident related to patient safety or due to the incapability to cope with the sudden deterioration of the issue which could have pressurized the junior doctors who are on strike to return to work settings to alleviate the fear of any harm and destruction caused by the patients due to the absence of so many medical persons at a time. According to the numbers mentioned by NHS, England, about 21,608 of junior doctors which represented about 78% of the doctors not present at their work setting had taken part in the industrial action. When compared with the figures of doctors who had participated in the previous strike held on 6-8th of April, the count was much lower than 88 per cent as reported on each day of the strike. But the figure 88% lifted a lot of questions as previously NHS England given the statement that about half of the doctors had given service on those days. The turnout figure was found to be the highest as mentioned by Barts Health, which is considered to be the biggest trust in the NHS. According to the report given by the trust of London, nearly 88.4% of the 1,000 junior doctors had participated in the industrial action (Goddard, et al, 2016). Similarly in the two hospital units maintained by the King’s College hospital trust located in the south of London, out of thirteen trainee doctors working in the obstetrician and Gynaecology setting did not turn up along with the twenty-six junior doctors who were working in the critical care unit. Moreover, about sixteen out of twenty-two junior doctors working in the emergency care setting also did not provide service as normal. The similar scenario was observed in the South London and Maudsley NHS foundation trust, where hardly 40 trainees out of total 246 had provided service which constituted nearly 84 per cent of turnout. Similar reports on turnout were observed in various parts of the United Kingdom such as nearly 81percent in Ipswich, 74 per cent observed at the Royal Free located in London, nearly 64 per cent reported from Blackpool and Stoke and 63 per cent reported from Bournemouth. Few doctors had stated that “I don’t support withholding emergency care. I don’t think it directly causes harm or affects safety, but it affects our relationship with the people we serve. Our profession has to have trust with the society we serve at its heart, and while I agree there is a longer-term view in all-out striking, for me a line is crossed. I would support continued striking, but not over acute and emergency care.” Though it was reported that approximately 13,000 numbers of operations and 113,000 numbers of outdoor patient appointments had been cancelled as a direct impact of the strike which continued for a week, the service provided by NHS had carried on smoothly without any obstruction as reported. As per the statements provided by surgeons very few trainees had turned up for the work and during this period of crisis and the consultants had managed very well to carry out the tremendous work pressure. The Prime Minister had also given remarks on the situation that the unmatched action was not rational from any point of view as the junior doctors had already been promised with a hike of 13.5 per cent in their basic pay structure as a paid-up for the unfriendly hours they had given the service. However, according to the outcome of an opinion poll conducted, approximately 59 per cent of the people residing at the United Kingdom had shown support to the junior doctors only, although they had a different opinion about the cause of the strike and tried to even frustrate Hunt (Goddard, et al, 2016; Metcalfe, et al, 2015).
Findings and Discussions
The study analysed the 3.4 million admissions, the number of outpatient appointments of 27 million, attendance at the A&E department involving 3.4 million for above 12 weeks. The study highlighted the following impact of the strike: the routine care service was withheld on the following days 12th January, 10th February, 9th – 10th March and 26th -27th April. The emergency care service including all the other services was withheld on the last two days of the strike. The total number of admissions on the following days were 53 279, 54 558, 107 243 and 99 866 respectively. The change observed in the total number of admissions were 4951(8.5%), 2633 (4.6%), 5873 (5.2%) and 18 194 (15.4%). The total numbers of emergency admissions on the following days were 20 307, 21 005, 40 908 and 40 077 and the change in the total numbers of emergency admissions were 1313 (6.1%), 30 (0.1%), 99 (0.2%) and 3383(7.8%) respectively. Similarly, the changes observed in the elective admissions were 3638 (9.9%), 2603(7.2%), 5775(8.0%) and 14 811(19.9%) on the following days. Regarding the outpatient appointments, the total change observed in the outpatient appointment by the provider were 17 641(54.6%), 12 739 (39.2%), 26 906 (42.5%) and 43 823 (66.8%) respectively on the following days. The significant change observed in the total number of attendances at the A&E department were 5219 (9.7%), 963(1.8%), 2314 (2.0%) and 17 325 (14.7%) and the number of emergency deaths observed was 616, 583, 1011 and 999 respectively. The numbers of deaths observed in the elective admission were 21, 18, 30 and 29 and deaths at A&E department were 73, 46, 127 and 110 respectively on the following days. The total mortality observed were 710, 647, 1168 and 1138 on the respective days (Refer Fig: 2 & 3) (Furnivall, et al, 2018; Ruiz, et al, 2013).

Fig: 2 the effect of all the four strikes on the hospital activities (Furnivall, et al, 2018)
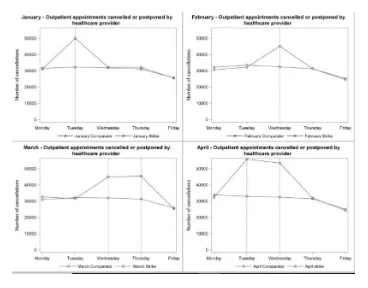
Fig: 3 the number of cancellations by the healthcare providers during the period of four strikes (the grey lines indicate the days of strike called by the doctors) (Furnivall, et al, 2018)
The study highlighted that the highest impact of the April strike on the normal operation and it lasted for approximately 48 hours. The emergency care services were also withheld during that time. The phase was also marked by the reduced number of admissions when the data were compared with the expected number for that period. The reduced percentage included the number of emergency admissions and elective admissions. The number of day cases also revealed a reduction of 18.7% or 9846 patients when compared with the previous week or subsequent week data. The fewer number of outpatient appointments along with the cancellation of the appointment from the provider and few numbers of attendees at the A&E department were the significant outcomes of the strike held at the year 2016 all over the United Kingdom. The reasons that had been attributed for the major impact of the strike were the prominent attention offered by the media during the period of strike and also due to its historic significance. Moreover, it was also highlighted by the study that the healthcare services gave prior intimation to the patients about not attending the providers until the required services were extremely necessary. However, the effect of the strike diminished during February and March 2016. The impact of the strike on the cancellation of appointments was highest during January and April which were about 54.5% and 66.8% respectively when it was compared with the expected outcomes. The regional analyses for the outpatient cancellations done by the health care providers were large in London, Yorkshire, the South East coast and the Humber. There was also a marked reduction in the total appointment attendance in the East Midlands (Goddard, et al, 2016; Rimmer, et al, 2018).
Moreover, the mortality rate of the patients did not alter during the period of strike and this observation was in accordance with the findings of the study reported about doctor’s strike. Though several authors have highlighted that death associated with poor quality of care service could not be analysed so fast. The most affected service during the time of January strike was the A&E department and this was attributed to the extreme media coverage and warnings provided by the hospitals. Previous studies had also shown the same impact of the strike called by doctors on the cancellations of the outpatient. The effect on the mortality could not be achieved because of the smaller period of study involved during the strike, the organisation had given focused on the priority of staffing during the period of crisis for the critical care patients though poor experience in the patient care service had been observed from the non-vital care. The same scenario was expressed by author Metcalfe, et al when the impact of industrial action of doctors was observed internationally. The data of the HES had been attributed with accuracy and the study conducted was the largest nation-based study to analyse the major activities of all the healthcare providers regarding the patient services. Moreover, this was the first strike where the emergency services of the UK were withheld and the researchers could study the impact on the emergency personnel. The findings of the study also highlighted that the NHS trusts responded successfully to the industrial action called by the doctors as they had effectively cancelled the appointments to prevent the services that involved higher risks. Therefore, the delay occurred for providing the health care service would result in effective cost burden due to the worsening condition of the patient, the demand of costlier treatment procedure for recovery and the negative quality of care provided immediately after the strike period (Furnivall, et al, 2018; Goddard, et al, 2016).
Limitations
The limitation of the study that should be mentioned here, is that most of the study utilized the information of the HES for conducting the study which could not be attributed as the sole source. Most of the studies highlighted the immediate effects of the strike during those particular days, but hardly any authors had reviewed about the prolonged effects of the strike or the aftermath of the strike. None of the studies highlighted the impact of the strike on the weekend to avoid the so-called “weekend effect” in association to mortality. Difficulties were faced to analyse the outcomes of the study as the counts were too small so no statistical significance was observed. The other associated parameters such as the morbidity, the opportunity cost of NHS and the patients and the financial cost were not focused within the study by any of the authors. The qualitative parameters such as the stress, inconvenience and disappointment were not measured during the period of the strike. The time constraints was another factor for the researcher to continue the study so only the effect of the strike was observed on those particular days. The study was self-funded so the data collection was also narrowed due to the registration policy of many high impact peer-reviewed journals. In those cases, only the abstracts were studied for the reference. The present work did not address the impact of the strike on the waiting time of the patient, strike associated progression of the disease and the quality of the outcome so in future studies should address these gaps in the literature.
Conclusion and Recommendations
The study provided a detailed discussion on the role of junior doctors in the society and how strike called by the junior doctors of the UK had an impact on the overall healthcare services. As doctors are the only legalized and authorized person to diagnose the diseased condition of the patient and prescribing the life-saving medications, therefore they are the indispensable part of the community or society. They play a key role in maintaining the healthy conditions of the community. There were several reasons behind the industrial action by the doctors which address some major areas such as the pay structure, the working hours, the improper infrastructure, to demand protection from the government. Previously several studies have already reported about the impact of the strike by the doctors on the health care services all over the world. The impact of the strike was found to be massive when during the end period of the industrial action when the doctors withdrew the emergency care services. The first four months of the strike in the year, 2016 involved the participation of the doctors from all the specialities all over England with a span of 24 – 48 hours which culminated up to 2 days. They had participated in that industrial action due to the amendment of few modifications in the contract as imposed by the Department of Health, Government which according to the doctors would result in poor patient care service in the future. The strike had a significant impact on the provision of healthcare, with thousands of appointments cancelled, and significantly fewer admissions and A& E department attendances than expected. Therefore, a detailed literature review of this issue would create more awareness of the danger inpatient care due to poor care concerning the doctor’s strike.
Therefore, the government should understand the demands of the doctors and should provide them with all the necessities for the efficient working of the health care system. As it is certain from the study that strike by doctors immensely damages the care services offered to the patient and this also highlighted about the gaps observed in the routine care services due to the staff shortages (Metcalfe, et al, 2015). Moreover, the industrial action is complicated due to the ethical values and the professional frameworks of the doctors. Unfortunately due to the strike, a third party who is neutral gets affected the most who in turn forces the government to accede to the demands of the strike. Several studies have also reported that doctors strike results in potential harm to their patients. Industrial action by doctors often highlights the rights of the doctors and their duty to their patients. Strikes are opposed by the medical regulators and in the UK it is considered to be an offence. The strike conducted by the doctors did not impact the mortality rate of the patients but it surely hampered the care service of the healthcare organisation and it was based on the duration of the strike and the extent up to which the doctors had participated. At the crisis moment of the strike, many senior physicians took the workload of the junior doctors. Therefore, it is extremely essential that doctors must balance their duties towards their patients and also their rights as individuals. The strikes impose political pressure on the employers and results in the financial loss for the organisation (Chima, S.C., 2013). Therefore, in future, it should be ensured that the doctors must organise the industrial action in such a way that it does not hamper the patient service. If the healthcare organisations are prepared for the emergency care service then the impact of industrial action by the doctors cannot reach a serious level. The service of senior physicians have to be increased during the time of strike to balance the workload and cancelling the number of elective admissions may increase the number of doctors to treat the available emergency cases. The emergency service should be increased or improved at the weekend level to prevent the mortality rate of the patients. However, in Israel, many doctors during the time of the official strike had also taken the responsibility of the emergency patients. The cancellations in the number of elective surgeries also reduced the rate of mortality on a temporary basis. The disruption caused by the strike was worsened by the managers as they overestimated the effect and therefore increased the staffing during the crisis period (Bhuiyan, et al, 2012). However, it was also evident from the records that most of the strike did not cause harm to the quality of the patient service offered. It was also observed the indicator for the quality care had improved or remained unchanged during the time of industrial action called by the junior doctors in Spain and New Zealand (Salazar, et al, 2001). The senior physicians who were taking the workload of the junior doctors during the crisis period were mostly at the expense of disturbance of the elective admissions. It was also noticed from the study that some doctors had also felt that the industrial action was inconsistent when compared with their professional obligations as the action had an inevitable impact upon the patient service. The industrial action by the doctors in the year, 2016 in the United Kingdom had a major impact during the end period as the emergency service was also disrupted during that period. It was also taken care during the time of the strike, that patients should not cause any serious harm by keeping the provision of emergency care services open. As observed during 1983, during the period of Jerusalem strike, the care provided to ambulatory patients had allowed the organisation to focus on the treatment of the urgent cases. As per the requirement of the General Medical Council (GMC), doctors should ensure that during the time of industrial action, patients should not be harmed or brought to any risk. Therefore, doctors should “satisfy themselves that arrangements are in place to care for their patients” during the period of strike (Irvine, D., 2006). In few cases, it was also observed that legal action was taken against the union of the doctors to break the strike, for example, a strike conducted for 18 days was 500 numbers of interns in Chicago in the year 1975, had eventually resulted to jail terms of the seven-team leaders. The strike conducted by the doctors in the UK, in the year 2012 had observed no cases against any doctors via the comprehensive search strategy using the Westlaw UK legal database (Thompson, et al, 2003).

References List
- Ogunbanjo, G.A. and Knapp van Bogaert, D., 2009. Doctors and strike action: Can this be morally justifiable?. South African Family Practice, 51(4), pp.306-308.
- Selemogo, M., 2014. Criteria for a just strike action by medical doctors. Indian J Med Ethics, 11(1), pp.35-8.
- Sedlis S. 2009. Meeting Perspectives: American Heart Association Scientific Sessions. Clinical Correlations: The NYU Langone Online Journal of Medicine. [Accessed 1Februrary, 2020]; http://www.clinicalcorrelations.org/?p=2123.
- American Heart Association. Scientific Sessions, 2014. [Accessed September 2, 2014]; http://www.exhibitatsessions.org/.
- Ruiz, M., Bottle, A. and Aylin, P., 2013. A retrospective study of the impact of the doctors’ strike in England on 21 June 2012. Journal of the Royal Society of Medicine, 106(9), pp.362-369.
- Machi, L.A. and McEvoy, B.T., 2016. The literature review: Six steps to success. Corwin Press.
- Melnyk, B.M. and Fineout-Overholt, E. eds., 2011. Evidence-based practice in nursing & healthcare: A guide to best practice. Lippincott Williams & Wilkins.
- Randolph, J., 2009. A guide to writing the dissertation literature review. Practical Assessment, Research, and Evaluation, 14(1), p.13.
- Illing, J., Morrow, G., Kergon, C., Burford, B., Spencer, J., Peile, E., Davies, C., Baldauf, B., Allen, M., Johnson, N. and Morrison, J., 2008. How prepared are medical graduates to begin practice? a comparison of three diverse UK medical schools. Final report to GMC April 2008.
- Martin Roland, D., 2004. Linking physicians’ pay to the quality of care—a major experiment in the United Kingdom. N Engl J Med, 351, pp.1448-54.
- sBhuiyan, M.M.Z.U. and Machowski, A., 2012. Impact of 20-day strike in Polokwane hospital (18 August-6 September 2010). South African Medical Journal, 102(9), pp.755-756.
- Block, L., Habicht, R., Wu, A.W., Desai, S.V., Wang, K., Silva, K.N., Niessen, T., Oliver, N. and Feldman, L., 2013. In the wake of the 2003 and 2011 duty hours regulations, how do internal medicine interns spend their time?. Journal of general internal medicine, 28(8), pp.1042-1047.
- Boex, J.R. and Leahy, P.J., 2003. Understanding residents’ work: moving beyond counting hours to assessing educational value. Academic Medicine, 78(9), pp.939-944.
- Bray, B.D. and Steventon, A., 2017. What have we learnt after 15 years of research into the ‘weekend effect’?.
- Burford, B. and Vance, G., 2014. When I say… preparedness. Medical education, 48(9), pp.849-850.
- Chen, J.Y., Kang, N., Juarez, D.T., Hodges, K.A. and Chung, R.S., 2010. Impact of a Pay‐for‐Performance Program on Low Performing Physicians. Journal for Healthcare Quality, 32(1), pp.13-22.
- Chima, S.C., 2013. Global medicine: Is it ethical or morally justifiable for doctors and other healthcare workers to go on strike?. BMC Medical Ethics, 14(S1), p.S5.
- Furnivall, D., Bottle, A. and Aylin, P., 2018. Retrospective analysis of the national impact of industrial action by English junior doctors in 2016. BMJ open, 8(1), p.e019319.
- Goddard, A.F., 2016. Lessons to be learned from the UK junior doctors’ strike. Jama, 316(14), pp.1445-1446.
- Gosden, T., Pedersen, L. and Torgerson, D., 1999. How should we pay doctors? A systematic review of salary payments and their effect on doctor behaviour. Qjm, 92(1), pp.47-55.
- Illing, J., Morrow, G., Kergon, C., Burford, B., Spencer, J., Peile, E., Davies, C., Baldauf, B., Allen, M., Johnson, N. and Morrison, J., 2008. How prepared are medical graduates to begin practice? a comparison of three diverse UK medical schools. Final report to GMC April 2008.
- Irvine, D., 2006. A short history of the General Medical Council. Medical education, 40(3), pp.202-211.
- Jena, A.B., Prasad, V., Goldman, D.P. and Romley, J., 2015. Mortality and treatment patterns among patients hospitalized with acute cardiovascular conditions during dates of national cardiology meetings. JAMA internal medicine, 175(2), pp.237-244.
- Lefroy, J., Yardley, S., Kinston, R., Gay, S., Mcbain, S. and Mckinley, R., 2017. early experiences Qualitative research using realist evaluation to explain preparedness for doctors’ memorable ‘fi rsts’.
- Lewis, J.M., Feasey, N.A. and Rylance, J., 2019. Aetiology and outcomes of sepsis in adults in sub-Saharan Africa: a systematic review and meta-analysis. Critical Care, 23(1), p.212.
- Liberati, A., Altman, D.G., Tetzlaff, J., Mulrow, C., Gøtzsche, P.C., Ioannidis, J.P., Clarke, M., Devereaux, P.J., Kleijnen, J. and Moher, D., 2009. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Annals of internal medicine, 151(4), pp.W-65.
- Lundin, R.M., Bashir, K., Bullock, A., Kostov, C.E., Mattick, K.L., Rees, C.E. and Monrouxe, L.V., 2018. “I’d been like freaking out the whole night”: exploring emotion regulation based on junior doctors’ narratives. Advances in Health Sciences Education, 23(1), pp.7-28.
- McKay, A.J. and Majeed, A., 2016. Junior doctors in England strike for the first time in 40 years. The Journal of ambulatory care management, 39(2), pp.178-181.
- Melnyk, B.M., Fineout-Overholt, E., Gallagher-Ford, L. and Stillwell, S.B., 2011. Evidence-based practice, step by step: sustaining evidence-based practice through organizational policies and an innovative model. AJN The American Journal of Nursing, 111(9), pp.57-60.
- Metcalfe, D., Chowdhury, R. and Salim, A., 2015. What are the consequences when doctors strike?. Bmj, 351, p.h6231.
- Metcalfe, D., Chowdhury, R. and Salim, A., 2015. What are the consequences when doctors strike?. Bmj, 351, p.h6231.
- Monrouxe, L., Bullock, A.D., Rees, C., Mattick, K., Webb, K.L., Lall, K. and Lundin, R., 2015. Foundation doctors, transitions and emotions: final report to the GMC: July 2015.
- Monrouxe, L.V., Bullock, A., Gormley, G., Kaufhold, K., Kelly, N., Roberts, C.E., Mattick, K. and Rees, C., 2018. New graduate doctors’ preparedness for practice: a multistakeholder, multicentre narrative study. BMJ open, 8(8), p.e023146.
- Monrouxe, L.V., Grundy, L., Mann, M., John, Z., Panagoulas, E., Bullock, A. and Mattick, K., 2017. How prepared are UK medical graduates for practice? A rapid review of the literature 2009–2014. BMJ open, 7(1), p.e013656.
- O'Halloran, C., Stewart, J., Singleton, S.J., Barton, J.R., Harrigan, P. and Spencer, J.A., 1999. Identifying appropriate tasks for the preregistration year: modified Delphi technique. British Medical Journal.
- Poissonnet, C.M. and Véron, M., 2000. Health effects of work schedules in healthcare professions. Journal of clinical nursing, 9(1), pp.13-23.
- Portney, L.G., 2020. Foundations of Clinical Research: Applications to Evidence-Based Practice. FA Davis.
- Prince, K., Van de Wiel, M., Van Der Vleuten, C., Boshuizen, H. and Scherpbier, A., 2004. Junior Doctors′ Opinions about the Transition from Medical School to Clinical Practice: A Change of Environment. Education for Health, 17(3), pp.323-331.
- Rhoades, E.A., 2011. Literature reviews. The Volta Review, 111(3), p.353.
- Rich, A., Viney, R., Needleman, S., Griffin, A. and Woolf, K., 2016. ‘You can't be a person and a doctor’: the work–life balance of doctors in training—a qualitative study. BMJ open, 6(12), p.e013897.
- Rimmer, A., 2018. Junior doctor strikes had a" significant impact" on services but did not increase deaths, study finds. BMJ: British Medical Journal (Online), 360.
- Ruiz, M., Bottle, A. and Aylin, P., 2013. A retrospective study of the impact of the doctors’ strike in England on 21 June 2012. Journal of the Royal Society of Medicine, 106(9), pp.362-369.
- Salazar, A., Corbella, X., Onaga, H., Ramon, R., Pallares, R. and Escarrabill, J., 2001. Impact of a resident strike on emergency department quality indicators at an urban teaching hospital. Academic Emergency Medicine, 8(8), pp.804-808.
- Saunders, B., Sim, J., Kingstone, T., Baker, S., Waterfield, J., Bartlam, B., Burroughs, H. and Jinks, C., 2018. Saturation in qualitative research: exploring its conceptualization and operationalization. Quality & quantity, 52(4), pp.1893-1907.
- Singh, J., 2013. Critical appraisal skills programme. Journal of pharmacology and Pharmacotherapeutics, 4(1), p.76.
- Thompson, S.L. and Salmon, J.W., 2003. Physician collective bargaining in a US public hospital. International journal of health services, 33(1), pp.55-76.
- Thorn, J.C., Turner, E., Hounsome, L., Walsh, E., Donovan, J.L., Verne, J., Neal, D.E., Hamdy, F.C., Martin, R.M. and Noble, S.M., 2016. Validation of the hospital episode statistics outpatient dataset in England. Pharmacoeconomics, 34(2), pp.161-168.
- Tipping, M.D., Forth, V.E., Magill, D.B., Englert, K. and Williams, M.V., 2010. Systematic review of time studies evaluating physicians in the hospital setting. Journal of hospital medicine, 5(6), pp.353-359.
- Toynbee, M., Al-Diwani, A.A., Clacey, J. and Broome, M.R., 2016. Should junior doctors strike?. Journal of medical ethics, 42(3), pp.167-170.
- Tso, S., Corrigall, D., Bennett, K. and Wood, E., 2014. A case study of a teacher development training programme for newly qualified foundation year doctors. Health and Social Care Education, pp.1-6.
- Vance, G., Jandial, S., Scott, J. and Burford, B., 2019. What are junior doctors for? The work of Foundation doctors in the UK: a mixed methods study. BMJ open, 9(4), p.e027522.
- Westbrook, J.I., Ampt, A., Kearney, L. and Rob, M.I., 2008. All in a day's work: an observational study to quantify how and with whom doctors on hospital wards spend their time. Medical Journal of Australia, 188(9), pp.506-509.
- Working Party of the Royal College of Physicians, 2005. Doctors in society. Medical professionalism in a changing world. Clinical medicine (London, England), 5(6 Suppl 1), p.S5.
Dig deeper into Impact of Homelessness on Access to Primary Care with our selection of articles.



- 24/7 Customer Support
- 100% Customer Satisfaction
- No Privacy Violation
- Quick Services
- Subject Experts