CBT's Impact on Fibromyalgia Management
Introduction/background
This review was aimed at examining the effect of CBT in the management of fibromyalgia symptoms in people of 18 years and above. In that regard, the study critically analysed evidence on both concepts: fibromyalgia and CBT. Fibromyalgia is a syndrome which involves chronic, widespread pain (Jackson, 2018). The rationale behind this review is based on the large number of patients on clinical placements with fibromyalgia. These patients, in most occasions, have had their extensively expressed concerns over cognitive behavioural therapy as a potential treatment to their condition. Fibromyalgia affects people of all ages. There are around 1.5 to 2 million people in the UK with fibromyalgia. It is thought to be more common than the statistics report since many people do not seek medical help and some are simply misdiagnosed (Walitt et al, 2015). Fibromyalgia, just as rheumatoid arthritis, is as common and more painful. Some severe symptoms occur where a person finds that they have to greatly modify their activities of daily living or, not being able to hold on to a job or enjoy much of a social life (Galvez- Sanchez et al, 2019). This condition is not commonly understood by experts. It is however known to have its basis on the chemical changes in the brain. For instance, body pains pulses are first transmitted to the brain (Bernardy K ,2017). There is usualy no particular source of pain when it comes to patients who suffer from this kind of condition. As a result, the elimination of pain is difficult as there is no other sickness or injury involved. In other articles, it has been suggested that patients with fibromyalgia actually have more pain carrying cells than those that would be present on a normal person (Jadad, A. R.,2016). From this basis, people with FMS may even hurt more from just minor bumps or bruises as compared to people without the condition. These persons would also feel pain from things that may not even have the capability to hurt at all (Ratini,2017). Although experts may not have definite standings on the causes of FMS, some of the reasons for such situations to occur include:

Literature review:
Whilst chronic pain is commonly associated with fibromyalgia, sleep disturbance, fatigue, headache, mood disorders and IBS are also symptoms that can be associated with the syndrome (Galvez-Sanchez et al, 2019). These symptoms can be difficult for individuals with fibromyalgia to cope with and significant lifestyle changes would often be required (Rodriguez, 2015). There are no pharmacological interventions for fibromyalgia recognised in the UK, although anticonvulsants (pregabalin) and antidepressants (duloxetine) have been investigated and have been found to have positive results. Both have been found to result in the reduction of pain, anxiety and depressive symptoms. However, improvements from medications that reduce pain in individuals with fibromyalgia are seen independently from changes in depression and anxiety. Simple analgesics such as tramadol can also be considered (Bernardy et al, 2013). These therapies have however demonstrated to have mixed effects in symptom management. For over two decades, CBT has been used in the management of different chronic pain conditions. CBT is underpinned by the theoretical assumptions of the interrelation between thoughts, emotions and behaviours (Luciano et al, 2014). Following this suggestion, a change in one of these areas should produce a change in the other two. The aim of CBT is to understand a patients’ thoughts and behaviours and in so doing helping in achieving positive outcomes. While attending their sessions patients are taught how to identify, evaluate and challenge unhelpful thoughts using cognitive behavioural experiments (Hauser, Bernardy, Uceyler, & Sommer, 2009).
Take a deeper dive into Understanding Risk Management in Military with our additional resources.
Methodology one:
In order to undertake a successful systematic literature review, a systematic electronic database search was carried out by using databases MEDLINE, CINAHL, and AMED. This enabled finding relatable papers regarding the search criteria entered on the database. The PRISMA flow group flowchart was also used (Appendix 2). For this search, keywords were as follows: fibromyalgia, cognitive behaviour therapy, FMS and CBT. The inclusion criteria for narrowing the results included: Both male and female research subjects, aged 18+ and suffering from fibromyalgia. Articles must have also focused on cognitive behaviour therapy and having been published in 2000 or above. There were exclusions for this review such as establishing that there were no systematic reviews for primary research that focused on CBT of symptom management success rates. In order to define the research review question, ‘PICOS’ was used, seen in table 3; this was also used to develop keywords for the literature search (Fink, 2014).


After this process, a total of 286 papers were matched against the inclusion/exclusion criteria. After exporting these reports to end note, a total of 56 papers were excluded due to being duplicates and a total of 226 reports were omitted through hand searching due to non-applicability of titles. This resulted in 4 reports for review (table 4). Table 5 illustrates an overview of the final papers that were used to undertake this review.

Methodology two:
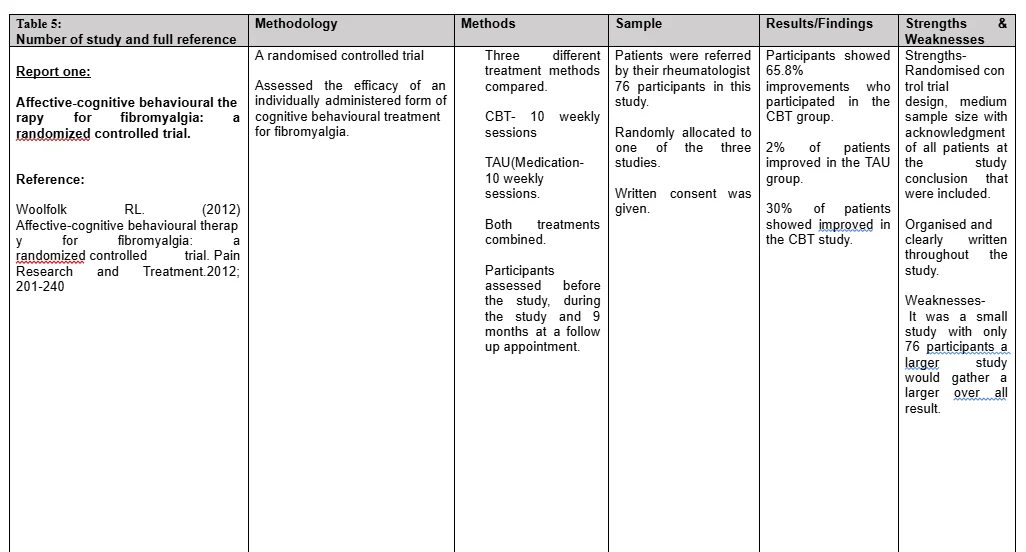
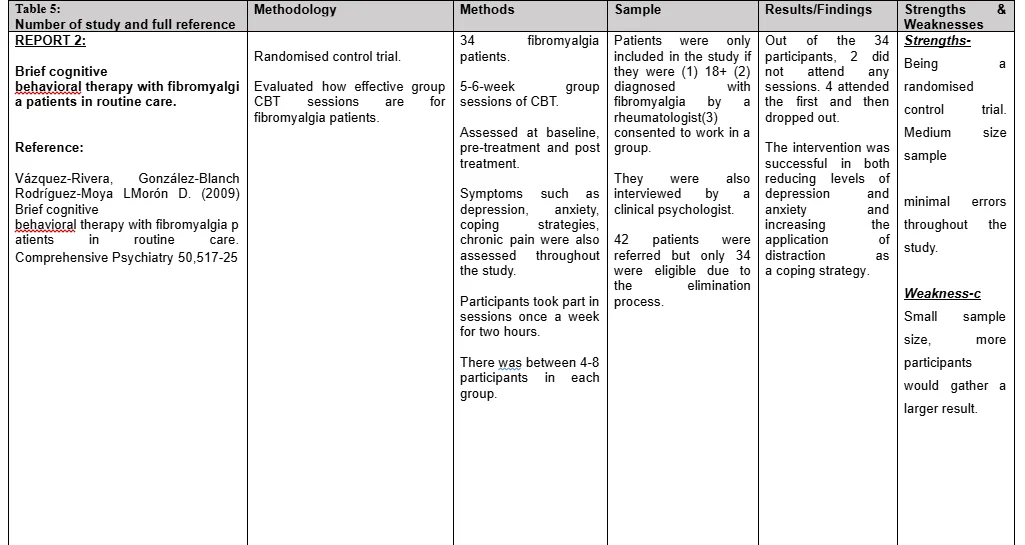
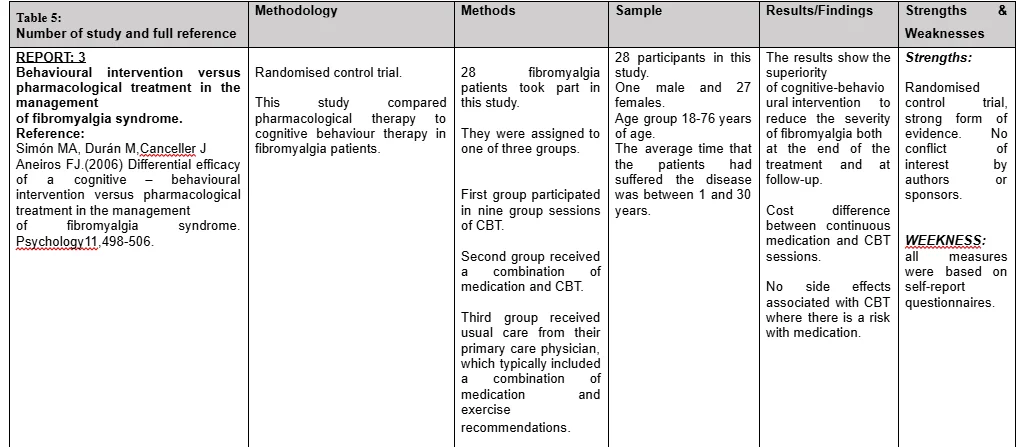
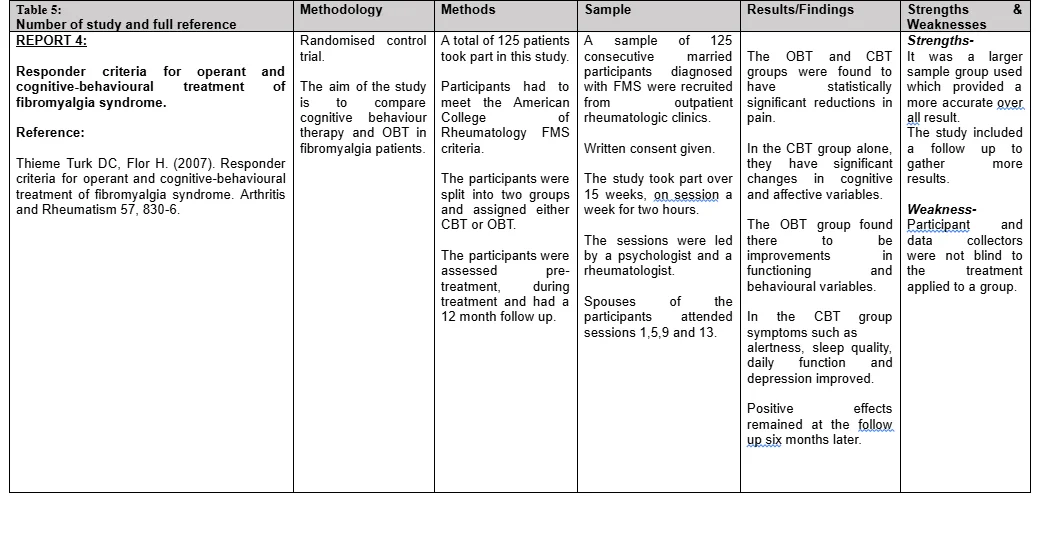
After carrying out a literature search, there were four papers which corresponded to the research question. All four papers were critiqued using the Critical Appraisal Skills Programme (CASP) tool (See Appendix 1). The CASP tools aims is to assist to understand research evidence, allowing one to critically appraise evidence and to validate its reliability (Nadelson and Nadelson, 2014). Specifying an issue or problem initiates the research process, followed by formulating a research question and finding a collection of relevant studies relating to the question/issue. A very reliable way of establishing valid evidence and credible conclusions is to look at the measurements, select samples and undertaking data analyses, for instance in the use of statistical techniques in the summary and interpretation of findings (Dowling and Brown, 2012). Each study focused on cognitive behaviour therapy and the effect it has on the management of symptoms of patients with fibromyalgia, each study highlights its strengths and weaknesses. Reports one by Woolfolk R, (2012) was a randomised control trial which compared cognitive behaviour therapy with the normal treatment for fibromyalgia patients (Woolfolk R, 2012) The sample size is important for planning and interpreting results, this study had a small sample size of 79 participants. A good element of this study was a follow-up appointment that was organised nine months after the baseline. This allowed for the assessors to see if CBT had benefited the participants after the therapy ended. It was reported that 30% of the participants felt as if their symptoms had reduced after the therapy. Report two by Vázquez-Rivera et al. (2009) also adopted a randomized control trial design. There were thirty-four outpatients with fibromyalgia participating in a 5- to 6-week group CBT program. From May 2006 to October 2007, a sample of 42 potentially eligible patients was interviewed by a clinical psychologist. Thirty-four patients were selected for this study. Patients were included in the study if the following criteria were fulfilled: older than 18 years and diagnosed of fibromyalgia by a rheumatologist. Each assessed for depression anxiety, coping strategies, chronic pain and physical functioning. They were assessed at baseline, pre-treatment and post treatment; using a pre-post, quasi-experimental design. One weakness of this study was the lack of follow-up assessments hence it could not reliably determine the stability of the gains or additional changes over time. Report three by Simón et al (2006) was also a randomized control trial. This trial compared pharmacological interventions with CBT. This was also a small sample size of only 28 participants. This report focused on participants that had been diagnosed with FM between the age of 1 and 30 years. The age of the participants at the time of the trial however ranged from 18-76. There are various strengths associated with this study, an assessment prior to the treatment, assessment after the treatment, and follow-up six months later qualify as some of these. A Quality of life assessment was used at week 8 of the study measuring health outcomes at self-care, usual activities, pain/discomfort and anxiety/depression. Weaknesses included: not being a comparative study, which would have been at a more advanced level being able to rectify and distinguish between other forms of treatment that is available for fibromyalgia patients. Although results showed a significant positive result for CBT, the size of the sample is important as with a larger sample size more information is gathered and the uncertainty of the results reduces (Carville, 2008). The results of this study, however, still justify that CBT is an effective therapy technique in the management of fibromyalgia. The study reveals that CBT is more effective than continued drug administration, which produces secondary effects besides a great economic cost long term. Report four by Thieme Turk and Flor (2007) had much significant strength such as involving the participants’ spouses in some on the CBT sessions. Involving the patients’ family can help to improve communication among family members, improving autonomy for each member, improve agreement about roles, reducing conflicts and reducing stress among the members to whom there is the patient. (Wiksell et al, 2012). A Quality of life assessment was used at week 8 of the study measuring health outcomes at self-care, usual activities, pain/discomfort and anxiety/depression. Weaknesses included: not being a comparative study, which would have been at a more advanced level being able to rectify and distinguish between other forms of treatment that is available for fibromyalgia patients.
Results/Findings
All papers were quantitative and the information relayed from them credible. Each of the studies focused on FMS and whether CBT is an effective therapy for this chronic pain disorder. All those reports reviewed in the study have been found to have similar thematic issues. The critique and analysis of the four articles are summarised above, see table 5. Report one focused on FMS patients who attended ten weekly sessions of CBT combined with usual treatment for FMS patients. This group of patients was then compared to FMS patients whom only received treatment as usual (TAU). Report two was completed over a shorter period of time with participants attending CBT sessions for only 5-6 weeks. Each participant was assessed on depression, anxiety, chronic pain, physical functioning and somatization. Report three compared the efficiency of CBT and pharmacological treatment combined with a group of participants who only received pharmacological treatment alone. Finally, report four focused on the effects of CBT and OBT (operant behaviour therapy). In all four-studies: psychological process and pain came out as major thematic concerns, the lack of knowledge and need for training also constituted some of the thematic concerns.
Psychological process
Aspects such as depression and anxiety were measured in each of the four studies. During the report, two depressive symptoms were assessed using the Beck depression inventory (BDI). BDI is a 21 self-reporting questionnaire developed by Beck et al in 1961. This questionnaire evaluates the severity of depression in normal and psychiatric patients (Van Koulil, 2010). During this study, the investigators found that anxiety and depressive moods can cause chronic pain for patients. If a patient’s mood improved from CBT, it could lead to less pain in diseases such as that from FMS. This study was successful in reducing levels of depression and anxiety symptoms by using distraction techniques during CBT sessions (Vázquez-Rivera S. 2009). Report one by Woolfolk R (2012) also used to Beck Depression Inventory (BDI) to assess levels of depression and anxiety in fibromyalgia patients. This study experienced significant changes in pain levels, but depression and anxiety levels did not change significantly throughout this study. Report three by Simon et al, (2006) reported that there was a significant difference in psychological variables during the post treatment phase and follow up. There was a significant drop in levels of depression and anxiety in the CBT group compared to the pharmacological treatment group (Simon et al, 2006). Report four reported that during this study, patients and spouses received weekly tasks to be completed alongside physical activities and reduced medication. Patients participated in relaxation exercises during and between sessions of CBT. It was concluded that due to the sessions of CBT alongside these extra activities and spouse involvement, 54% of participants had a reduced physical distress and lower levels of anxiety and depression after their CBT (Alda et al, 2011)
Pain
Aspects such as pain were measured throughout each of the four studies. Pain score was measured on a 10cm visual dialogue scale of pain (VAS). VAS is a subjective measure for acute and chronic pain. Scores are recorded by making a handwritten mark on a 10-cm line that represents a continuum between “no pain” and “worst pain” (Hauser, W.,2009). Participants were asked to rate their level of pain over the weeks they attended their sessions. During report one by Woolfolk RL., (2012) study the visual dialogue scale of pain was a key element for recording changes in pain over the course of the study. A score was taken at baseline and by the end of the study. A significant improvement in pain was recorded at the follow up session with 62.5% improvement since baseline (Woolfolk RL., 2012). Report two by Vázquez-Rivera S. (2009) participants took part in an assessment called CAD (coping questionnaires for chronic pain). CAD consisted of 5 subscales related to different coping styles. These were (1) Religion, (2) Distraction, (3) Mental self-control, (4) self-affirmation and (5) information seeking (Kroese, M.,2009). This study aimed to promote the use of distraction as a basic strategy for coping with pain. After brief CBT sessions over 5-6 weeks there was a significant change in pain scores on CAD sub-scale (Vázquez-Rivera S. 2009). It was recorded that 45% of the patients treated with CBT demonstrated a clinically significant reduction in pain and it maintained over 12 months following treatment (Vázquez-Rivera S. 2009). Report three examined different effects of pharmacological (amitriptyline or cyclobenzaprine) interventions compared to CBT (Simon et al, 2006). CBT reduced pain symptoms in both post treatment and follow up time periods. Interestingly, CBT and psychopharmacological approached did not show similarly significant improvements in pain. Report four consisted of patients who either received operant behavioural treatment (OBT) or cognitive behaviour therapy (CBT). Significant improvements were found in the CBT group on dependent measures of pain intensity, interference, depression, anxiety, self-efficacy, spousal response to pain, medication intake and pain behaviours. These improvements were demonstrated in spite of concurrent reduction in medication intake. The OBT therapy and medication management comparison group deteriorated in almost all variables measured (Thieme Turk DC, Flor H,2007).
Lack of Knowledge and need for training
Successful treatment often requires the addressing of cognitive, behavioural and affective processes in fibromyalgia. This is because of the complex and dynamic nature of chronic pain experienced by the patients (Hassett et al, 2009). Across all reviewed studies, there have been long held challenges in the treatment of patients with chronic pain conditions. In basic sense, pain is construed to be a dynamic and complex phenomenon that is greatly influenced by certain factors. These factors include cognitive, behavioural, physiological and social factors. The need for knowledge and better understanding even by the health care professionals is evident. Through such knowledge, health care providers, including the nurses, would be able to develop patient- centered programs of treatment for these kind of patients (Arnold et al, 2012). Through such treatment, self- management by the patient and ongoing education are encouraged. In most cases, this is designed for primary settings of health care (Paiva & Jones, 2010).

Discussion:
Methods that reduce and aim to control fibromyalgia are the basic management techniques of the condition. There are currently three medications approved in US by the Federal drug administration but not in the UK, but researchers have found that their effectiveness is limited (Bernardy et al, 2013). Cognitive behavioural therapy (CBT) is the main non-pharmacological intervention that has been studied. The aim of CBT is to address some of the psychological components of the disorder as it increases the patients’ belief in their ability to manage their condition (Yunus, 2012). When a patient participates in this therapy it helps to change their pessimistic thoughts and feelings regarding symptoms like pain, fatigue and sleep problems (Yunus, 2012). Techniques are thought to help the patient to manage their symptoms better and develop a different attitude towards pain. Report three in this study researchers assigned patients to one of three groups for a six-month study period: one group participated in nine group sessions of CBT; another group received a combination of medication and CBT; and the third group received usual care from their primary care physician, which typically included a combination of medication and exercise recommendations. At the end of the study period, the CBT group scored higher on measures of quality of life, Pain, fatigue and this approach also demonstrated clear cost savings. An additional bonus of CBT is that unlike in pharmacological treatments, CBT does not cause side effects or complications (Simón et al,2006) In report one by Woolfolk RL., (2012), the study concluded that there was a 65.8% improvement in pain and fatigue symptoms in the CBT group. The participants reported that they had more energy, less pain, that they were taking fewer naps and were more active in general. Vázquez-Rivera S. (2009), report two, stated that brief CBT is effective in reducing emotional distress and was successful in both reducing levels of depression and anxiety and increasing the application of distraction as a coping strategy in fibromyalgia patients. Report four concluded that brief CBT is effective in reducing symptoms of fibromyalgia such as alertness, sleep quality, daily function and depression. In this study, a significant number of people undergoing CBT have not only improved during treatment but have been able to maintain the effects at the six-month follow-up (Thieme Turk DC, Flor H,.2007). The average fibromyalgia patient is seen by fifteen doctors and struggles to be diagnosed for approximately for five years (Buckelew,2018). Most of these patients are often misdiagnosed and endure costly treatments with little benefit. Some health care professionals do not even believe that fibromyalgia actually exists (Burckhardt, 2011). Although most patients are relieved when a correct diagnosis is finally made, the patient may need to be convinced that their doctor or nurse actually knows what is wrong, and that a treatment plan has been formulated to alleviate his/her symptoms. Managing fibromyalgia can be as complex as the illness itself. Once a patient is diagnosed, they should have a multidisciplinary approach and collaboration with the patient and family. Although the ideal treatment does not exist, each plan should be individually compiled based on the symptoms of the patient (Vlaeyen, 2016). It is important that nurses should be professional, supportive and empathetic to the patient and his/her family. Effective communication is also required as the nurses should have the ability to explain to the patient and his/her family well of the condition and the necessary treatment plan (Suman, 2016).
Conclusion:
It is evident, from these studies, that patients living with fibromyalgia endure a lot of frustration with bothersome symptoms that affect their daily lives. The health care community does not understand the condition as well as they should. It is imperative as nurses that we understand the complexity of the syndrome while caring for the patient (Alegre et al, 2010). It is important to understand the reality of the symptoms associated with FMS and the possibility of management. Through such professional advice, patients may see the need to participate in non- pharma- logical treatments such as CBT. CBT has made significant gains in the field of psychological treatments for individuals with fibromyalgia. However, considerable gaps still remain in the literature. First, researchers should continue to use commonly used, reliable and valid outcome measures for monitoring outcomes such as pain, functional status, depression, anxiety, and fatigue and sleep problems (Edwards et al, 2011). Furthermore, research would be strengthened if more randomised blinded controlled studies were conducted to measure the effects of CBT and CBT with a multidisciplinary approach. Research should be compared with exercise and pharmacological therapies. In summary, while there are some limitations to this qualitative review, the evidence supporting the use of CBT to improve functioning, decrease pain, depression, anxiety and psychological distress is strong.
References
Alda, M., Luciano, J., Andres, E., Serrano-Blanco, A., Rodero, B., Lopez del Hoyo, Y., Roca, M., Moreno, S., Magallon, R., Garcia- Campayo, J. (2011) Effectiveness of cognitive behaviour therapy for the treatment of catastrophisation in patients with fibromyalgia: a randomised controlled trial. Arthritis Research & Therapy
Alegre de Miquel, C., Garcia- Campayo, J., Florez, M., Argueles. J., Tarrio, B., Montoya, M., Martin, A., Salio, A., Fuentes, J., Alberch, A., Gomez de la Camara, A. (2010) Interdisplinary consensus document for the treatment of fibromyalgia. Actas Esp Psiquiatria
Arnold, L., Clauw, D., Dunegan, J., Turk, D (2012) A Framework for Fibromyalgia Management for Primary Care Providers. The Mayo Foundation for Medical Education and Research
British Journal of Nursing, 2011. Cognitive behavioral therapy and its relevance to nursing. British Journal of Nursing 20(22), pp.1443-1447.
Buckelew, S. P., Conway, R., Parker, J., Deuser, W. E., Read, J., Witty, T. E., et al. (2018). Biofeedback/relaxation training and exercise interventions for fibromyalgia: A prospective trial. Arthritis Care Research, 11, 196-209.
Burckhardt, C. S., Clark, S. R., & Bennett, R. M. (2011). The fibromyalgia impact questionnaire: Development and validation. The Journal of rheumatology, 18, 728-733.
Carville, S. F., Arendt-Nielsen, S., Bliddal, H., Blotman, F., Branco, J. C., Buskila, D., et al. (2008). EULAR evidence-based recommendations for the management of fibromyalgia syndrome. Annals of the Rheumatic Disease, 67, 536-541.
Dowling, P. and Brown, A., 2012. Doing Research/Reading Research. Hoboken: Taylor and Francis.
Galvez- Sanchez, C., Duschek, S., Reyes, G (2019). Psychological impact of fibromyalgia: current perspectives. Psychology Research and Behavior Management. Dove Press
Hassett, A., Gevirtz, R. (2009) Nonpharmacological Treatment for Fibromyalgia: Patient Education, Cognitive- Behavioral Therapy, Relaxation Techniques, and Complementary and Alternative Medicine. Rheumatic diseases clinics of North America. HHS Public Access
Hauser, W., Bernardy, K., Uceyler, N., & Sommer, C. (2009). Treatment of fibromyalgia syndrome with antidepressants: A meta-analysis. Journal of the American Medical Association, 301, 198-209.
Jadad, A. R., Moore, R. A., Carroll, D., Jenkinson, C., Reynolds, D. J., Gavaghan, D. J., et al. (2016). Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control Clin Trials, 17, 1-12.
Luciano, J., D’Amico, F., Cerda- Lafont, M. (2014) Cost-Utility of Cognitive behavioural therapy versus U.S. Food and Drug Administration recommended drugs and usual care in the treatment of patients with fibromyalgia: an economic evaluation alongside a 6- month randomized controlled trial. Arthritis Research & Therapy
Martin SA, Coon CD,McLeod LD,Chandran A,Arnold LM. (2014). Evaluation of the fibromyalgia diagnostic screen in clinical practice.Journal of Evaluation in Clinical Practice, 20 (2), pp. 158-165.
Menzies, V., Taylor, A. G., & Bourguignon, C. (2006). Effects of guided imagery on outcomes of pain, functional status, and self-efficacy in persons diagnosed with fibromyalgia. J Altern Complement Med, 12, 23-30.
Nadelson, S. & Nadelson, L., 2014. Evidence-Based Practice Article Reviews Using CASP Tools: A Method for Teaching EBP. Worldviews on Evidence-Based Nursing, 11(5), pp.344-346.
Sephton, S. E., Salmon, P., Weissbecker, I., Ulmer, C., Floyd, A., Hoover, K., et al. (2007). Mindfulness meditation alleviates depressive symptoms in women with fibromyalgia: Results of a randomized clinical trial. Arthritis and Rheumatism, 57, 77-85.
Suman, A. L., Biagi, B., Biasi, G., Carli, G., Gradi, M., Prati, E., et al. (2009). One-year efficacy of a 3-week intensive multidisciplinary non-pharmacological treatment program for fibromyalgia patients. Clinical and experimental rheumatology, 27, 7-14.
Vázquez-Rivera S, González-Blanch Rodríguez-Moya LMorón D, 2009. Brief cognitive behavioural therapy with fibromyalgia patients in routine care. Comprehensive Psychiatry 50 (6), pp. 517-25.
Wicksell, R., Kemani, M., Jensen, K., Kosek, E., Kadetoff, D., Sorjonen, K., Ingvar, M., Olsson, G. (2012) Acceptance and commitment therapy for fibromyalgia: a randomized controlled trial. European Journal of Pain
Wigers, S. H., Stiles, T. C., & Vogel, P. A. (2006). Effects of aerobic exercise versus stress management treatment in fibromyalgia. A 4.5-year prospective study. Scandinavian Journal of Rheumatology, 25, 77-86.
Yunus, M. B. (2012) Towards a model of pathophysiology of fibromyalgia: Aberrant central pain mechanisms with peripheral modulation. Journal of Rheumatology, 19, 846-850



- 24/7 Customer Support
- 100% Customer Satisfaction
- No Privacy Violation
- Quick Services
- Subject Experts