SLT in Interprofessional Education and Practice
DISCUSSION
The current study explores the discipline of SLT in Interprofessional Education and Interprofessional Collobrative Practice. The undertaken literature review clearly highlighted the positive side and barriers at systemic, organisational, and interpersonal levels (D’Amour and Oandasan 2005) in addition to the field of research as regards Interprofessional Collaborative Practice, with a singular focus on nursing and medicine with teams working in acute settings. Correspondingly, the Interprofessional Education also presents limited research in IPE outcomes. In turn, the two factors impress the significance of current research to ensure quality contribution to the existing body of research. Throughout the course of the existing study, the researcher hopes to demonstrate the theoretical and practical implications of IPE and IPCP in SLT.The discussion chapter will get into the following four parts: (i) the first section highlights the research objectives and the corresponding research question. This section thereafter addresses the research questions individually. Moreover, the research questions and responses are structured to substantiate the association between literature review and findings; further aligning them with the current research findings’ and their impact on the existing knowledge, specific to the current research area. The learning experience would be summarized with an emphasis on the research outcome’s, benefits to SLT policymakers, researchers, and other relevant impacts.Next section will discuss the meetingobjectives and addressing research questions
Meeting objectives and addressing research questions
The objective of exploring the SLTs’ experience in Interprofessional Collaborative Practice and Interprofessional Education was successfully achieved through the collection of appropriate and relevant data in semi-structured interviews addressing the research topic. The findings of data analysis and the conclusions drawn reflect the outcomes of this investigation. The objective was successfully achieved with the employment of qualitative research methodology. The participant’s responses to these questions can be explained by focusing on adult learning, reflective learning, and Interprofessional Learning theories. Exploring the roles assumed by SLTs’ in different interprofessional contexts along with the SLTs’ team experience and roles and their attitudes towards teamwork, and education was successfully achieved. Research on participant perspectives and knowledge about pre-registration preparation were explored in the interviews by asking questions about their pre-registration courses, learning styles as well as attitudes towards team working.The thematic analysis of the responses collected during interviews and their subsequent interpretation focused on pre-registration courses,and attitudes towards team working to achieve these two objectives. With a focus on reflective learning, Interprofessional Learning and adult learning theories, the objectives were further enriched. SLTs who participated in interview in a school, hospital, mental health units, and patient homes. Sometimes, the SLTs went to three different work settings according to findings.According to the findings, SLTs sometimes did not feel like being themselves when they were a part of the team, especially when working with many different teams.Overall, research objectives was successfully achieved. Next part will discuss the addressing the research questions.
Research Question 1: What are the experiences, roles, and knowledge of the recently qualified SLTs about Interprofessional Collaborative Practice?
Research Question 2: What are the outcomes of the Interprofessional Education for SLTs current interprofessional collaborative practice?
This section will address both these research questions individually and draw appropriate conclusions. According to current findings research questions was answered successfully which will discussed in-depth later on in the sections called experience of SLTs in interprofessional working and interprofessional education. The responses of the research questions assess and review the association between the literature review and the findings along with its subsequent impact on the existing research knowledge. While research tried to get data on experience of SLTs in IPE/IPCP.Next section will discuss the summary of the themes and research findings.
Continue your journey with our comprehensive guide to Factors Affecting Root Canal Success.
Summary of themes and connection between themes
Current research findings discussed earlier in findings chapter. The section below will focus on to the summary of the key findings, and then will focus on to the how these findings connected with each other’s.The first main theme is “interprofessional team working” which discussed the how the team works, what works well and what works not well, a holistic awareness, leadership and hierarchy, decision-making, and the barriers for interprofessional team working.There are certain benefits associated with inter-professional team working such as empowering team members, closing communication gaps among the members of the team, etc. The second major theme related to “Interprofessional Communication”, which discussed the communication types of interprofessional teams and how they communicate with each other’s. The third main theme related to “how it feels to be and function as an SLT” and the factors affecting it, including not being understood adequately by others. SLTs professional identities. The fourth main theme is Interprofessional Education which mentioned SLTs experience on IPE their understandings, limitation and benefits of IPE, skills required for IPE and attitudes towards IPE when preparing for practice. After a brief summary of the themes now we will focus on to the connection between themes.All themes and subthemes have some connection with each other.As a human communication scientist SLTs have very specific professional perspectives on IPE and IPCP. The IPE (Interprofessional education) occurs when multiple professions learn about, from, and with one another in improving collaboration and the quality of services and care. In the profession of nursing, the consideration of collaboration and interprofessional communication of baccalaureate education’s one of nine essential elements takes place in the practice of nursing profession. In addition, there have been certain professional organizations emphasizing the benefits of interprofessional collaborative practice (IPCP) and IPE following the commencement of clinical practice and ending of the formal education. .The role of the communication has also been highlighted as one of the essential elements of interprofessional relationships. It has been also reported that the existing literature has overlooked a discussion on communication theories. The role of communication elements and their effects on the interprofessional collaboration has not been discussed on the literature. Also,it would be really interesting to see other healthcare professional’s perspectives on IPCP. Amidst this, communication themes emerged as one of the most important themes to associate with other themes. The literature has emphasized the importance of interprofessional relationships and communication. However, current research findings showed the perspectives of Communication specialists on to the IPCP and IPE. The theme of the communication has directly and indirectly connects with others. Such as, On the first main theme “interprofessional team working” communication was one of the main elements in relationships between professionals, the discussions and disagreements with in teams, decision making and leadership process include the elements of communications. Collectively, these studies outline a critical role of communication as theme and how that connected with other themes.According to O’Daniel and Rosenstein 2008, communication helped healthcare professionals to workcollaboratively,share responsibilities for decision making and doing care plans for patients. However, lack of communication and interactions caused medical error and unsafe practice. Also, communication types and skills used within interprofessional team settings and Interprofessional Education played a key role in resolving conflicts between different professionals and improving patient outcomes.O’Daniel and Rosenstein 2008 mentioned that “Effective communication among staff encourages effective teamwork and promotes continuity and clarity within the patient care team. At its best, good communication encourages collaboration, fosters teamwork, and helps prevent errors” p3.For interprofessional relationship and team working having relevant communication skills and knowledge was mention by SLTs several times.Meanwhile subthemes like leadership and decision-making have a strong link with communication types and skills.For instance, SLTs mentioned conflicts in their teams, hierarchy and leadership issues which all directly and indirectly related to communication and conflict resolution skills.O’Daniel and Rosenstein 2008p5 point out that “In health care environments characterized by a hierarchical culture, physicians are at the top of that hierarchy. Consequently, they may feel that the environment is collaborative and that communication is open while nurses and other direct care staff perceive communication problems. Hierarchy differences can come into play and diminish the collaborative interactions necessary to ensure that the proper treatments are delivered appropriately”. Which has clearly supported relationship between communication, leadership, hierarchy and their effects on to the practice.
Have saying that complexity of the work environments and working models of SLTs had included some sort of communication elements. According to O’Daniel and Rosenstein 2008 “A large body of literature shows that because of the complexity of medical care, coupled with the inherent limitations of human performance, it is critically important that clinicians have standardized communication tools and create an environment in which individuals can speak up and express concerns” P9. The complexity of SLTs work settings and organizational structures caused communication errors and lack of collaborations. Correspondingly, subthemes like understanding of IPE and the takeaway of IPE suggest that connection between interprofessional team working and other aspects of IPE remain strong. SLTs mentioned that interprofessional education prepare them for interprofessional collaborative practice. With interprofessional education, SLTs have learnt other professional’s roles, responsibilities and knowledge is which help them to develop their interprofessional working skills. In addition, the theme of how it feels to be a SLT has a strong link between subthemes like leadership and hierarchy, communication skills, and types.SLTs mentioned that they feel alone when they work with in a team; most of the professionals do not have any ideas about their roles. In addition, issues around the leadership and hierarchy made them more isolated. Their feelings about their professional identity and other professional’s perspectives shaped their feeling on their roles.Finally, since Interprofessional Learning and working activities are primarily based on communication and interpersonal skills, communication remains one of the main interconnected themes. Which have connected with all themes and subthemes. At this section, we discussed the connection between themes and subthemes. The next section will discuss some of the key findings of current research.
Discussion of key findings
The current research made four key findings that have not been mentioned in existing literature. The first one is IPE provides SLTs with an opportunity to promote their job at the students’ level. According to SLTs some of the team which they have been worked with have not got any ideas on SLTs roles, at the practice level, SLTs felt that being recognized by other professionals was nothing short of a battle. Since they are a small professional, sometimes their roles have not yet been adequately known or understood by same professionals. However, there has been some professional which can understand SLTs roles. Such as, Occupational therapists and Physiotherapists. The second finding illustrates that IPE workshops need to be more realistic because real-world settings are different from university environments. At university level, SLT have not got enough realistic approach on IPCP. Which could help SLTs to made links between theory and practice of IPE/IPCP.At the clinical level, there were not enough opportunities to see and engage with different professionals. While the perspective of different professionals has been mentioned in existing literature, the viewpoints of SLTs have not been adequately covered. Meanwhile the third research finding demonstrates that different personalities have a great (positive and negative) impact on interprofessional relationship. For example, some challenging personalities might affect interprofessional relationships negatively and the other positive personalities could support the interprofessional relationship positively.In the literature, not enough evidence has been presented to underpin the effect of personalities on interprofessional relationships and collaborative practice. Meanwhile the final key finding from the current research has given disagreement resolutions and complexity of SLTs work environments. The research has underpinned the importance of use their communication and diplomatic skills to resolve conflict in the best possible manner. The fresh perspectives of SLTs could enable them to view things from different angles and propose actionable solutions to improve real-life outcomes.SLTs mentioned that they have used their diplomatic skills to avoid any conflicts in their teams.

The teamwork processes, much like all social activities, have been fraught with conflict or with conflict’s opportunities. The teams that are effective have been characterized with having surfaced and processes conflict when appropriate. The competencies are possessed by the team members to address the conflict constructively with other team mates and they facilitate the conflict’s team management observed by them. For example, some of the participants mentioned that when they communicate with other professionals they have carefully choosed their words and their communication types. Which mainly seen that they prefer to meet other professionals face to face to avoid misunderstanding of written language. Which again have not been discussed previous literature.In addition, SLTs work pattern and cross-sectoral works, which we have discussed at previous chapters, caused complexity in interprofessional team working. Which was not mentioned at previous literature in interprofessional field. Overall, This four findings which have not enough mentioned at previous literature. This key findings might helped IPE/IPCP and SLT literature to build up some other researches on that areas. Which will discussed on recommendations and conclusion chapters in details. Next Section will focus on to the current research findings and how that findings fit into the current international capability frameworks on IPE/IPCP with role clarification, team functioning, interprofessional communication, patient/clients/family community-centered care, interprofessional conflicts resolution and collaborative leadership.
Current research findings in some of the International IPE/IPCP Framework context
When researcher started to write discussion chapter he realized that some of the current research findings perfectly matched with current IPE/IPCP frameworks. Which will discuss on next section. According to O’keef at all 2017 there were six national and international competency framework in interprofessional education and collaborative practice fields. This are Canadian Interprofessional Health Collaborative (2010) A national interprofessional competency framework, Interprofessional Education Collaborative Expert Panel (2011). Core competencies for interprofessional collaborative practice: Report of an expert panel, Interprofessional collaborative, Washington, DC., Combined Universities Interprofessional Learning Unit (2004) Interprofessional capability framework: a framework containing capabilities and learning levels leading interprofessional capability,The University of Sheffield and Sheffield Hallam University, Sheffield,Interprofessional capability framework: A framework containing capabilities and learning levels leading interprofessional capability,Griffith Health IDEAS 2011. An interprofessional framework for interprofessional learning at Griffith Health 2011–2014, Griffith University, Griffith Queensland ,Brewer ML, Jones S. 2013. An interprofessional capability framework focusing on safe, high quality client-centred health services. J Allied Health,Faculty of Medicine, Dentistry and Health Sciences. 2010. Interprofessional Education & Collaborative Practice. A Curriculum Framework. The University of Western Australia.
The national and international competency framework in interprofessional education and collaborative practice fields mentioned above recognizes that there are several health systems across the world that have been subject to fragmentation and struggles in managing the unmet needs related to health. The future and the present workforce have been given the task to provide health services in the context of the rising complexities in the health issues. The evidences have indicated that as there is movement of these health workers through the system, for them the opportunities in gaining the interprofessional experience provide helping hand in learning the needed skills in becoming involved in the collaborative practice-ready health workforce.
These have affected the IPE/IPCP implementations around the world. Current research findings have been fit well in to the Canadian National interprofessional competency Framework (CHIC 2010) with in this six model of core capabilities framework.The researcher has suggested that Canadian interprofessional health collaborative framework could help to develop an interprofessional education curriculum for SLTs for pre-registration and post-registration level.The CIHC National Interprofessional Competency Framework have a set of competencies that included the attitudes, behaviours, values, and judgments which have necessary for collaborative practice (CIHC, 2010). The six CIHC competency domains are:
Role clarification
Team functioning
Interprofessional communication
Patient/client/family/community-centered care
Interprofessional conflict resolution
Collaborative leadership
“Collaboration is a developmental process, and therefore, interprofessional learning is cumulative over one's professional practice, reflecting a continuum of learning” (CIHC, 2010 p 12).According to curriculum design, the framework has clear definitions of the parameters of interprofessional practice and education with some principles. The competency domains of the CIHC framework have been integrated into the current research findings. One of the main findings of the current research was knowing each other's roles, and responsibilities have been an important element of interprofessional working. According to SLTs Interprofessional education activities give SLTs opportunities to understand other professional’sroles, responsibilities, knowledge and skills.Interprofessional education and collaborative practice experience of SLTs clearly show that knowing others roles and responsibilities could help team working and promote their job. Promoting their job will be discussed under a different domain. Findings related to team roles were mentioned at CHIC frameworks with team roles domain which stated that “Learners/ practitioners understand their role and the roles of those in other professions, and use this knowledge appropriately to establish and achieve patient/client/ family and community goals". (Chic, 2010, p12). The statement of the CHIC clearly showed that current research findings of team roles fit in that domain. The elements of this domain could be used at pre and post-registration level. On pre-registration level placement based IPE/IPCP activities could help SLTs to understand other professional's roles and responsibilities. Also, it gives them an opportunity to express their jobs.
Other main findings from current research were a patient/client centred approach which was mentioned several times by SLTs, such as, SLTs mentioned that families and clients involve into the practice was a positive effect on the outcomes of the practice. Also, they have indicated that client's interest would be the in the heart of their practice. Furthermore, SLTs suggested thatPatient involvement in IPE activities was a positive and effective model for them to understand IPE/IPCP. Also, SLT mentioned that IPE and IPCP give them a holistic view and patient centred perspectives. According to CHIC framework “Learners/ practitioners seek out, integrate and value, as a partner, the input and the engagement of the patient/client/family/community in designing and implementing care/services”. (CHIC 2010 P13). The experience of SLTs on IPE and IPCP showed that SLTs worked for patient best interest with a patient centred approach. For SLTs education and practice patient/client/service user or student centred approach would always be a hot topic. Pre and post-registration IPE and IPCP activities should give SLTs patient centred perspectives.
One of the other main findings mentioned by SLTs was team functioning, which SLTs mentioned that working with other professionals was vital however not an easy mission. They have stated that working with a cross-sectoral and different team made their interprofessional teamwork more complex. SLTs think that working with different personalities and characters made interprofessional working more challenging. Also, personalities has been a challenge in mono professional practice as well. The work nature of the SLTs work forced them to work in the different sector, teams and settings which could affect their relationships and team workings. CHIC 2010 frameworkhave mentioned issues with Team Functioning domains. According to team function domain of CHIC 2010"Learners/practitioners understand the principles of teamwork. Dynamics and group/team processes to enable effective interprofessional collaboration”. (CHIC, 2010 P14). The importance of team working has always been an important topic for all health and social care professionals. IPE and IPCP gave SLTs opportunities to deal with that complex team working issues.
IPE workshops especially placement based IPE and IPCP activities could help SLTs to improve their team working skills learning team dynamics and functioning.
Current research findings pointed out leadership, hierarchy and decision making several time. SLTs think that leadership, hierarchy and decision making depended on the team setting they have worked. In some setting, they feel more hierarchy than the other setting. Sometimes they feel more equal in some settings than the other. SLTs explain that with different work setting have different leadership mechanism, and this could affect hierarchy and decision-making process. One of the domain in CHIC framework mentioned that “Learners/practitioners understand and can apply leadership principles that support a collaborative practice model”.(CHIC, 2010 p15). For the SLTs to understand leadership and management issues at the pre-post registration level in IPE/IPCP workshops and learning activities needs to include leadership and management subjects. There may be some interagency work needed to train SLTs and other health care students together with business and management students. For the both sidesstudents could learn from with about each other in IPE/IPCP activities on Pre-post registration and placement level.
The original documents on that domain there were not mention on business and management IPE/IPCP. The research was put that as a suggestion for SLTs training and practice institution to develop some IPE/IPCP activities with business and management faculties to improve their leadership knowledge.
The interprofessional collaboration and communication are considered by the nursing profession along with baccalaureate education’s nine other necessary elements for the practice of professional nursing. In addition, there are a few professional organizations emphasizing the IPCP and IPE benefits after the ending of the formal education and commencement of the clinical practice. The WHO and the IOM have published recommendations highlighting the multidisciplinary practice of interprofessional communication and improvement in the patient care.
Leadership and management skills were teaching and training at business and management faculties. For health and social care students having business and management IPE workshop might be help to improve their leadership and management skills. Also having IPE workshops could help business and management students to improve their skills on health and social care managements. According to current research findings SLTs think that leadership and management has been an important topics in their practice which shape their relationship with the teams.
Furthermore, they have discussed decision making and the role of leadership in decision making process has been vital.
Modern social and health care recognizes the patient-centred care’s importance. With respect to this, the most important aspect is for the right of an individual to have full involvement in the decisions related to the healthcare. This right receives protection in most Western countries by legislation. For instance, the NHS Constitution in England with 5 domain resources states the shared decision-making, person-centred care, and self-management as the key deliverables because of the contribution of these to well being and health. A person having the “mental capacity” is subject to assumption that he has the ability of making his own decisions in relation to his healthcare and social needs. The decision making, however, is a complex process and having involvement of multiple linguistic and cognitive abilities, manipulation of the information in a deliberative process, appreciation of whether a decision is made or not made and the consequence of it, the communication of the choice.
Interprofessional communication was one of the main findings at current research. SLTs have very specific knowledge and perspective on communication.
That may be because of their professional backgrounds and perspectives on communication. They mentioned that interprofessional communication skills and communication types were significant effects on to the team working. The CHIC framework has a domain on Interprofessional Communication which stated that“Learners/ practitioners from different professions communicate with each other in a collaborative, responsive and responsible manner”.(CHIC, 2010 p16). According to CHIC framework communication would be responsive, responsible and collaborative manner, which could help to interprofessional communication of professionals. For the SLTs educational and practice institutions training of interprofessional communication at Pre and post-registration level has been an important issue.
Everyone has a role in inclusive communication. However, unique skills and knowledge is possessed by the SLTs in developing understanding, knowledge, and awareness in all areas in minimizing inclusive communication. The unique core theoretical knowledge possessed by the SLTs related to the communication, language and speech. They bring about clinical skills of specialist nature having focus on the optimization of the improvement of the life quality and capacity of communication of an individual. The social models are applied by the SLTs to intervene the disability of communication. They are equipped well in enabling the understanding that is best possible between people having disabilities in communication and their families, staff, carers, and wider community. SLTs, as such as, are the most important players to lead and develop the inclusive communication practice for populations, communities, organizations, services, environments, and individuals. However, commissioning, demand, and capacity will have influencing effect with regards to the time spent by the SLTs to fulfill their roles at these levels.
The IPE activities at pre-registration level especially within the placement are vital for SLTs to learn interprofessional communication. Also, at the post-registration level IPCP activities need to cover interprofessional communication activities. This could train SLTs to communicate with other professionals with a "responsive and responsible manner.
The patients with autism and/or learning disabilities in the settings of a hospital have been at risk due to poor communication. This is not limited only at an individual level, but also at the organization and services level. The breakdown of communication has been an environmental risk factor clearly as there has been no interaction by the staff in general with the people supported by them with respect to enabling individuals achieving higher level on integration, participation, and independence. This shows the need of developing an environment of communication around the RCSLT (2013) related to the standards of good communication around reasonable adjustments in minimizing involvement, engagement, and inclusion at service and individual level. The researchers have suggested that Pre and Post registration IPE/IPCP activities should also have more elements of the interprofessional communication skills and workshops.
Interprofessional conflict resolution was mentioned by SLTs several times under the main theme of communication. According to SLTs managing disagreement in different settings and teams needs and skills and knowledge. Some of the SLTs mentioned that diplomatic skills and using appropriate communication methods and skills helped to avoid conflict in interprofessional teams. The CHIC framework suggests that subjects with the domain of Interprofessional Conflict Resolution which stated that “Learners/practitioners actively engage self and others, including the client/patient/family, in positively and constructively addressing disagreements as they arise”.(CHIC, 2010 p17).
Also, Current research findings show that SLTs have great diplomatic communication skills to communicate with other professionals. They have tended to use that conflict resolution tactics to resolve possible conflicts in their teams. There were not enough evidence to show that this skills learnt from IPE workshops. Interprofessional Conflict resolutions domain would be help SLTs to understand potential conflicts and solation of them. The researcher suggested that at pre and post-registration level of SLTs IPE/IPCP activities should need to cover conflict resolution tactics and tracing workshops.
To sum up, some of the current research findings perfectly fitted into the CHIC, 2010 Framework of capability. This clearly showed that CHIC framework for capability should be used for a base for IPE/IPCP activity design for SLTs. However, unfortunately there is no example of the institutions which used that framework or IPE curriculum with SLTs in the UK accept De Montfort University. Moreover Leicester IPE curriculum was design before CHIC 2010 Frameworks. This means that Leicester model of IPE and SLTs experience on that fits clearly into the CHIC 2010. Next section will discuss the meeting objectives and addressing research questions.
SLTs experience of mono professional practice
In today’s world where communication holds the key to every possible problem, SLTs have emerged as a distinct class of health professionals who can boost the way individuals communicate. In this manner, we are able to gain insights into the job type and life of the SLTs. According to interview data participants tend to explain their current mono professional practice. They have mentioned putting clients into centre of their practice, their typical work days and how they work with clients. This part was not a research aim of objectives however it was mentioned by participants several times. To fulfil this criterion, they play an important role and engage in various activities through direct interaction or supporting acts. In the current scenario, constructing assessments, checking and updating assessment procedures, talking to clients as well as executing the act of therapy forms the primary activity of an SLT. In addition, prescribing proper care plans and providing credible support to the fellow caregivers are also expected from the SLTs. The main interpretation that comes up from SLTs perspectives is the understanding of the team. They generally tend to reinforce their mono professional team. For instance, if the researcher asked a question related to team, they started to talk about their SLTs team in the region. This clearly showed that understanding of team mostly their mono professional teams. We have discussed SLTs perspectives on mono professional practice. The next section will focus on answering of the main research questions, which would be the experiences of SLTs in IPCP and IPE.
The experience of SLTs in interprofessional team working
One of the main research question was about the SLTs experience on interprofessional working. Answer of that research question will discuss in depth in this section with details. According to current research findings, there are several main areas from which the themes emerged. These include interprofessional education, Interprofessional collaborative practice, interprofessional communication and professional identity issues of SLTs, complexity of their work and personalities. This section will focus on the interprofessional collaborative practice experience of the SLTs discussion of these findings with relevant literature. The section will commence with the experience of SLTs in interprofessional team working and continues with complexity, professional identity and personality.Interprofessional collaborative practice (IPCP) has become a necessity in the healthcare sector where the objectives include health improvements, patient care, and affordability of healthcare for patients.SLTs understating of interprofessional working depended on their different work settings.The current research has highlighted new findings through the participants’ responses to the research questions focusing on interprofessional team working; most SLTs have positive perspectives on interprofessional team work.Some of the theories which explain that withUnique IPCP practices can play a significant role by improving healthcare service delivery through proper intervention (Zierler, Blakeney and Brien 2017). Researches have observed improvements in the functioning of teams with IPCP meetings in hospice providers. An interview conducted on 24 service providers revealed the capacity of meetings to improve service quality and assist in holistic patient development. However, there were concerns of meeting inefficiencies resulting from constraints on content and lack of participation. To that end, some modifications and standardizations can help increase meeting efficiencies (Washington et al. 2016).
Finding the best services for patient ad sharing patient information’s with professionals gives SLTs a holistic view of how things work, help them better understand child and adult needs and other professionals’ perspectives.This might be explained by Marris (1986) used psychodynamic theory to describe loss and change. Meanwhile Holman and Jackson (2001) used the Marris’ theory in their study involving seven interprofessional workshops for staff caring for older adults. They found that interprofessional communication had a powerful effect on social care. Ineffective communication can lead to confusions in roles which emphasize the role of professionals, thereby affecting their performance negatively. On the other side, an effective interpersonal communication can give positive outcomes through an increase in motivation and enthusiasm in healthcare workers such that they can provide high quality service to patients. With saying that there have been some positive outcomes of interprofessional team working mention by SLTs.They used terms like“everyone gives their input it is very important” “Participants saw interprofessional collaboration as “positive” for their patients”. This might be explain byElspeth (2012) statedthat cross-sectorial SLT has positive outcomes on educational and therapy professionals. Professionals in education and health/social care sector need to communicate with each other and share their knowledge. Overall under the Nancarrow 2013 (P1-2), ten characteristics underpinning effective interdisciplinary team work were identified: positive leadership and management attributes; communication strategies and structures; personal rewards, training and development; appropriate resources and procedures; appropriate skill mix; supportive team climate; individual characteristics that support interdisciplinary team work; clarity of vision; quality and outcomes of care; and respecting and understanding role”. According to the participants, positive leaderships and personalities have a positive impact on interprofessional teamwork. At this part, we have discussed the positive outcomes of interprofessional team working for SLTs.
There are also some barriers of interprofessional team working which mention by SLTs.According to SLTs, organizing people from multidisciplinary backgrounds was problematic. Sometimes, there was a lack of space; rooms, equipment, time and using language could cause some barriers for SLTs. As a result, it became really stressful to arrange everything in a proper manner. The fact that various kinds of people came together in the same place made a lot of things dependent on luck. The nature of the SLTs’ practice and organizational/systems approach could affect this collaboration. This would shape the notions of students and others in such a way that a sustainable collaborative system can be formed which can then help develop a permanent place for the collaborative learning practice”. Also, Healthcare professionals need to be trained on different disciplines in order to gain real collaborative lessons and to become competent healthcare. Provision of healthcare needs a strong coordination between practitioners which can be made possible with this learning. However, in practice, the students are not so widely trained primarily due to cultural barriers (Pecukonis, Doyle and Bliss 2008).According to theories and research findings to avoiding barriers of interprofessional team working we need to use interprofessional education and train professional together. Interprofessional education train and prepare professionals for interprofessional collaborative practice. We have discussed the experience of SLTs into the interprofessional team working. Next section will focus on to the complexity of SLTs work pattern, settings ininterprofessional collaborativepractice.
Complexity
Empolyment opportunities and how that has change...working cross-sectoral work….
As the nature of SLT practice determines, SLTs are simultaneously required to work with several different teams, professionals and sector at the same time.Some of them work in the education services and health services at the same timeand the others work in social care and criminal justice system. Which caused several complexity.This section will discuss start to focus on time and place and how that’s caused complexity, language, culture and communication types, different settings and different leadership issues which have caused complexity. Thereare some participants think thatthey did not feel a sense of belongings in the team because they sometimes worked at three different places and as a result, did not get their own space to connect with other professionals at their workplace. Gum at al. (2012) explained some of the main barriers for interprofessional communication are poor design, lack of space and privacy. A well-designed place and space would encourage all members of healthcare team to communicate with each other to promote interprofessional collaboration. The first challenge identified was that professionals who needed to work closely with SLTs were located in different places. This made it difficult for them to integrate. They also used phrases like “in a situation where we are not placed”, “you're much more isolated from the MDT” and “we're quite often mobile.” IPE needs a great amount of investment in online resources and classroom learning structures.This might be explain by (Brewer, Flavell and Jordon 2016) The outcome of IPE is expected to be an increased rate of return on this investment for which, the IPE practice needs to be sound and have ability to change the perceptions of students on collaborative practices. The culture of hospital is entirely medical in nature and when the SLTs are trying to collaborate with the doctors or medical professionals, it can be extremely difficult for the SLTs if the medical professionals are constantly interacting among themselves using terms that the SLTs do not understand.
Hall (2005) stated that different health care professionals have different identities, cultures, values, beliefs, attitudes, customs and behaviours.
This difference affects both professional relationships and communications. Educational experiences and socialising process during the training of health professionals shapes their professional cultures. Marshall at al. (2011) point out that “language can impact significantly on the ways in which health care professionals relate and provide clinical services, as well as the way in which patients conceptualize their role in the healthcare encounter”(P4).This suggests that using difficult jargons can sometimes cause problems for communication and interprofessional interaction.IPE practice can help decrease learning cost, enhance patient care, and improve the quality of healthcare. However, it remains to be seen as to how intervention can be done to create a supportive specific setting. An understanding of social practices and processes is required to fully understand how care is to be provided (DiazGranados et al. 2018).
Some SLTs were also of the opinion that communication should be the focal point rather than the workplace. This means that great emphasis should be on the way people communicate or interact with each other. SLTs think that if they can collaborate, it would certainly be for the best interest of the service user. Some SLTs are also of the opinion that their mobility makes them more accessible, which then adds to their edge. It does not take a lot of effort for the service user to find them and that even if they missed a session, they could quickly make up for it. The research revealed that the fact that some medical centres were spread over large areas makes it difficult for the SLTs to sometimes not receive information at a proper time, which affected the way in which the service users received the therapy.
SLTs felt that the fact that they were not all from the same place and they did not get enough time to communicate with others did not help the cause.This is consistent with the findings of Baxter (2004) stated that working in different setting with different clients has great impact on SLTs communication and interprofessional works. On the other hand, Gum (2012) opined that communication and interaction barriers were related to poor design, lack of space, frequent interruptions and a lack of privacy for health care professionals. The SLTs are of the opinion that it is the duty of the people mediating between the patients and the SLTs who can apply the gathered knowledge effectively. Sometimes, the SLT would do as much as they could to ensure that whatever is required by a particular class is included in the knowledge stream of the reader. According to SLTs, different work settings have a different leadership and hieratical system. They used terms like “are perhaps some members who are quite hierarchical”, “I think see us as equals and really value our opinion” and” It depends on my particular role for the client” to illustrate hierarchy at their interprofessional teams. This might be explain by (Kent 2018) an exploratory research study was conducted on IPE initiatives taken by a metropolitan health network involving clinicians who were part of the process of designing the activities. The inputs were taken using an interview process which revealed three key themes for the development of IPE activities, which included IPE considerations, organizational and clinical factors. There can also be considerations of sustainability such as investment in the education, establishment of education roles and an expansion of the IPE activities (Kent 2018).Health and social care are integrated in many countries through the provision of primary care, community programs, hospitals and social care. However, the process changes do not really guarantee benefits in the case of delivery. The improvement of the health care quality and the challenges it poses continued to be identified with a health care collaborative team having essentiality to improve the outcomes of health. The IPE studies have shown that health professionals have collaborated in teams in managing complex practice situations requiring the informed and systematic collaboration between the professional specialities and different professions in recent years. Moreover, the collaborative practice is also shown by the research that can be improving the coordination and access of the outcomes, resources, and services for people with chronic diseases while reducing the conflicts, tension, and the complications with the caregivers, staff turnover, clinical error rates, and hospital readmission. The current health workforce has been a critical element to strengthen the systems of health care and to expand the universal health coverage. The initiation of IPE by WHO is to improve the ability of the health care workers to provide the high quality care.
Facilitation can help in building collaborative relationships such that a transformational change can be achieved. However, this would not independently enhance the quality of care, and may need the support from learning and development. Some key elements that are used in an integrated approach to facilitation include work based learning, improvement, development, innovation, social care, and knowledge transfer (Martin and Manley 2018). We discussed the timing and workplace effects on complexity. There are also some SLTs mentioned about the lack of equality in some settings, especially in medical settings, which caused complexity as well.Theyhave added that working, as a team with different professionals was a positive experience. They mentioned about education settings, which is quite positive and easy to work with. In medical settings, the consultants made the ultimate decision and took responsibility of those decisions.This might be explain by Lingard (2012) discussed the ways in which interprofessional teams tried to achieve common goals; evidence indicated that the actual enactment of collaborative leadership was indeed a challenge. Doctors think that their teams functioned in a non-hierarchical manner; however, reports from non-medical professionals suggest that there was some hierarchy in their teams.
According to Lingard (2012), theobservation data revealed that those hierarchical behaviors persisted, even from those who most vehemently denied the presence of hierarchies in their teams. During the course of this current research, SLTs sometimes felt the impact of hierarchy within different settings. For example, they felt it more at NHS than at the schools. Band levels are a one of the main hieratical parameters within the context of mono professional teams and interprofessional teams. All this elements around language, jargon, time, different culture, different work settings and sector could cause complexity, which was clearly mention by SLTs. Next section will focus on the negation and relationship to resolve that complex issues around interprofessional team working.
NEGOTIATION AND RELATIONSHIP
The SLTs interact and work with professionals from various fields this caused some complications and complexity, which we discussed at previous section.This section mainly focusing on SLTs negotiation and relationship elements to minimize that complexity with their perspective. Those who primarily participated in the interview reported mostly about the following fields within which they collaborated. It generally included pharmacist, doctors, psychologists, teachers, psychotherapists, paediatricians, and others. These fields required a lot of active SLTs who could come to the aid and help the ones in need of therapy. Schools and rehabs were also among the top collaborators. This is consistent with the Reeves and Lewin (2004) activity theory to explore the nature of teamwork in relation to temporal-spatial pressures. This means that building relationships between professionals related to formal and informal communications. Interprofessional collaboration is suggested widely in the social and health care policies. However, the researches existing have the provision of relatively poor understanding with regards to the way the collaborations are done between the professionals or the attached meaning to their collaborative work. In addition, various studies (Barnes and Turner, 2001; Kennedy and Steward, 2012) have examined the collaborative relationship between teachers and occupational therapists. Teacher participants reported frustrations on not having formal collaborative meetings with occupational therapists (Barnes and Turner 2001). Nevertheless, teacher participants understood that the occupational therapists’ high caseload made it difficult to schedule regular meetings (Barnes and Turner 2001). The SLTs perceive that one can perform different roles in their interprofessional collaborative practice. To that end, it is imperative to have good communication channels with all professionals.
The staffs employed in a plethora of formal and informal strategies of communication have been for overcoming these constraints. Also, collaboration’s contrasting accounts are given by the professionals: the view of the doctors with collaboration is mainly as an activity that involves work along with their medical colleagues, where the views of other professionals has been as an interprofessional activity. The contrasting notions and temporospatial constraints of collaboration are the key factors to shape the interprofessional collaboration’s nature. The policies in promoting this activity fail assuming that there is existence of collaboration’s shared understanding. There is also need of being mindful of the practical constraints affecting the hospital ward’s collaboration.
Analogously, Allport (1954) developed the social psychology theories which described the tension between group members. Groups require equality, common goals, and cooperation. Common goal or shared goal between professionals is to give patients a good quality of care. Allport 1954 theory of group dynamics helps us to understand different dynamics between interprofessional team members. Meanwhile Jains (1982) and Tuckerman and Jensen (1977) developed the group thinking theory. Similarly, social exchange theory (Challis et al. 1988), cooperation theory (Axelrod 1984), relational awareness theory (Drinka et al. 1996), and team reflexivity theory (West 1996) are important in the field of inter-professional collaboration. All this related theories helped researcher to understand interprofessional relationships between team members are important to deliver quality care.
This research anticipated the impact of mutual perception on commitment, cohesion, and trust. This study investigated the group dynamics that affects the interpersonal trust, commitment to group members, and cohesion. The results are suggestive that larger group members have less commitment and group having a size of more than six members have negative association with the trust level that the group members reports.
According to these responses, the SLTs think that some professionals are easier to work with as compared to others; for instance, they opine that working with professionals such as, OT, PT, Psychologist and Dietician is easier than working with consultant and medical professionals. Some SLTs explained these situations with different personalities and in different settings. Interprofessional approaches to health and social care are linked to improved clinical service and enhanced problem solving (Mitchell et al. 2010). Generally, through the collaborative efforts of diverse medical professionals, SLTs think that overall the collaboration is a good idea. We have discussed about formal and informal communication between professionals and theories behind that. Now we will focus on to the knowing each other’s roles and responsibilities and how this does effects the negotiation and interprofessional relationship.
For a Good negotiation and relationship, SLTs think that knowing each other roles and responsibilities has been crucial. Some SLTs have had a very positive experience within the education services, whereas others had some negative experience in the health sector. The workplaces can include schools, nursing homes, rehab centres, working with special children and so on. In the school team, the lead would be the SENCO or the head teacher, which will be discussed under the heading of leadership and hierarchy. They would speak to the SLTs as coordinators to coordinate or have a basic overview of the process, understand how it was working with the different teaching assistants, and get referrals from children. Mostly SLTs have had some opportunities for interprofessional communication within interprofessional team meetings and case meetings. Most common issues mentioned by SLTs included knowing each other’s roles and responsibilities. This was evident in the following statement: According to Benne and Skeats (1948 as cited in Payne 2000), three important factors affect team roles: (a) the behaviour of the team members, (b) the skills of the members, and (c) their helpful or unhelpful roles. The behaviours of team members are important for quality communication between each other. Individually, the professionals’ perception of their role, whether helpful or unhelpful, impacts their satisfaction and performance. Some participants mentioned that knowing other professional’s roles and their own boundaries could help them communicate better. Similarly, Engestrom et al. (1999) developed the activity theory, which affects interprofessional and inter-agency relations at micro and macro levels. Engstrom et al. (1991) developed Vygotsky’s model of mediation into a triangle of individual relationships between the subject, the object, and the mediating artefact. In this research, this process has implications in terms of the quality of communication. When the SLTs provide recommendations and similar things, if a staff member does not understand one of them, or needs to be reinstructed for the same, they can easily approach the SLT because they know what days they would be available and where to find them.
This might be explain by Hartas 2004 mentioned, “Collaboration is a key aspect in developing effective educational provision for pupils with special educational needs.” Teachers and SLTs view collaboration as a formal and distinct activity that can only occur within a pre specified time and space allocated to it, which encourage individuals to engage in prescribed activities whilst remaining within their own professional boundaries. Implications for policy and practice are discussed and issues for future research are raised.
The key aspect to develop the provision of education for pupil having the needs of special education is the collaboration. The collaboration, in this study, has the conceptualization as the educational effort’s dynamic system endorsing co-equal, interdependent and collegial styles of interaction between SLTs and teachers. Seventeen SLTs and twenty-five teachers were asked completing a questionnaire and participating in group discussions for provision of information regarding collaboration’s perception at a school with their colleagues catering for children with communication and language difficulties. Across the quantitative and qualitative analyses, the consistent suggestive results that SLTs and most teachers considers time commitment=constraints and the structures of the organization that are rigid hinders factors in their collaborative workings with others. The willingness and making professional changes and learning from one another, share beliefs and values and individual contribution, on the other hand, have been considered as supportive factors. The collaboration of the SLTs and the teachers has been as a formal and distinct activity occurring only within a pre-specified space and time allocated to it, which encourages the individuals in engaging in prescribed activities while remaining within the professional boundaries of their own. The implication for the practice and policy has had their discussions and future research issues have been raised.
SLTs have very strong feelings on importance of the communication, which was stressed by SLTs in many different ways. This statement of SLTs could support by Southill et al. (1995) which pointed out that communication between professionals and between professionals and clients positively affects the quality of care and the utilisation of resources. Interprofessional collaboration can make patient care more effective and safe for patients through discussions on clinical problems. A study involving three focus group discussions to understand what is considered as an ideal interprofessional found that the spatial and social structures can influence collaboration (Verhaegh et al. 2017). A better underdoing of communication failures can be achieved by exploring case studies involving interviews and physical artefacts (Leijen-Zeelenberg et al. 2015). It was found that the communication routines were embedded into practices and some repetitive patterns which had caused failures needed improvement (Bardach, Real and Bardach 2015).
The scholars of health communication are increasingly attending as to how the communication is shaped by hospital built environment as been found in the results. The results are also indicative that there is significantly more walking by the nurses in the new environment of the hospital. The qualitative analysis has shown the development of three insights in relationship to the outcomes, processes, and system structure. Firstly, the system interdependency has been changed by the decentralized nurse stations by the reduction of the team work and nurse to nurse interactions while heightening the teamwork and interdependencies with other occupants of healthcare. Secondly, several processes that are nurse related remained centralized while decentralizing takes place of nurse stations that created for the nursing some system based problems. Thirdly, the practices related to the nursing communities were affected adversely by the new design. This study’s implications are suggestive that patient outcomes, patient care processes, and communication are shaped by the nurse station design. Moreover, it is key to understand how the environment is built, which in communication research is usually treated as invisible, is critical in understanding the communication with the complexities of health care systems.
For a better communication SLTs mention some skills which have an import role on interprofessional relationships.The key communication skills mentioned by SLTs requires understanding others, good listening skills, flexibility, friendliness, adaptability, willingness to share information, pushing to cater for the interests of patients, and an empathetic attitude. Flexibility and adapting to others’ ways of working were also important in a team. A study was conducted at three Australian States on 68 pharmacy, nursing and medical graduates on interprofessional teamwork and communication. Students were able to comprehend the importance of team work, communications skills, and other professionals(Thomson, Outram, Gilligan and Levett-Jones 2015). Another study involving four reference lists explored to understand the role of visual and performing arts in developing professional skills found that the students could enhance their teamwork and communication skills using various art forms (Acai, McQueen, McKinnon and Sonnadara 2017).Organisation plays a key role in this process since SLTs are always in and out of schools.
They observed that when a problem arose, it was often easy to forget about it straight away, so they needed to be organised enough to write it down and remember to go and email the therapist once they were back at their base. They observed this work really well when one examines the work of SLTs as roles in schools, it can be said that their role is to manage the SLET within the school, which means they should provide support, training, observation assessments, and prepare teaching assistants to carry out the interventions. The personalities of these professionals tend to affect their interprofessional communication and thus, in general, the SLTs must be assertive enough to put their views across in the team because they are constantly subjected to doubts about their opinions on certain subjects. Which might be explain by Curren et al. (2010) stated that different professionals have different attitudes, which can affect their professional practice.
Some participants have experienced difficulties working with different professionals like doctors and pharmacists. This maybe shows that different professional culture and attitudes have some impact on interprofessional working. The interprofessional teamwork also depends on the particular role of SLTs for those particular clients. The respondents stated that some clients were lead professionals, in which case, their role was around care coordination. In others, since they were a part of the team, they did the professional bit but did not engage much in care coordination. For others, it was just another part of their rotational job role. Thus, they rotated between teams in the hospital. They worked there for six months before getting promoted. It was an organisational mind-set that they all adopted to develop as speech therapists. They felt that it was good for patientoutcomes because everybody can work together and becomes aware of their needs as individuals.Which could be explain by Martin (2008), school and SLT staff learn together when they work together; this may also affect the outcome of SLT in school settings. The respondents stated it most of the times it gets a bit challenging because they try and offer CPD opportunities to educate the staff about the role of the SLTs. Due to some types of hospitals in which the patients were generally found, it was quite challenging to get the staff to commit to Speech and Language tasks. Thus, it can be surmised that some areas definitely needed improvement. In general, the outcomes that are agreed upon are realistic.
The only point for consideration regarding this particular area was that the therapy and the time of rehabilitation could take years. Often when patients left the facility, they might have to go to another rehab center.Generally, the SLTs thought that the outcomes agreed for patients are realistic. Thus, the study reveals the importance of communication, which as per the Joint Commission (2010), has also been identified as the leading contributing factor of medical errors. Furthermore, according to Leape and Berwick (2005), Interprofessional Communication is extremely relevant in multidisciplinary teams for the organization of care delivery. We have discussed the importance of communication and communication skills in negotiation and interprofessional relationship. We have discussed the communication skills which mention by SLTs. Now, next part will discuss the communication types, which could made negotiation and relationship easy.
There were several ways in which team members communicated with each other such as, face to face, email, phone and meetings, which are mentioned by participants. Twenty-three out of twenty-five pointed out that face-to-face communication was the most preferred way of communicating due to the difficulties associated with emails, phones or texts in explaining a point. In working environments, communication is the golden key, with a fundamental understanding of the professionals’ roles to conduct flawless communication. The SLTs need both organizational skills, patience, and analytical skills during assessments. All these entail communicative competency, e.g. the ability to share views through reports on emails. In addition, interprofessional working is imperative in SLTs working, which shows a majority of skills required to work with children. Also, since they mostly work in schools, organisation plays a major part in this process. With specific reference to doctors, the personalities of the professionals tend to affect Interprofessional Communication and communication itself. This requires an attitudinal change in doctors and pharmacists to ensure that equal importance is accorded to the SLTs and address the universal incongruence between the SLTs and the doctors. Correspondingly in communication, SLTs need to be assertive to counter being constantly subjected to doubts, as against taking their opinions seriously.
Sargeant et al. (2011) stated that the communication skills of health care professionals could improve with formal communication skills training. Communication is also important due to the work of multi-disciplinary teams on case-to-case basis, as they are fundamental to intersecting relationships. For some SLTs with rotational professional roles, communication is essential as the roles requires the ability to explain things in layman's terms, understanding other people’s perspectives and understanding the parents, or understanding or talking to teachers about how a child could get through the classroom.We have discussed communication types and skill for interprofessional relationship and negotiation, which have mention by participants. Next part will focus on the decision-making. How negotiation and relationship skills help for a decision-making.
According to SLTs, decision-making does affect interprofessional teams and their relationships. This partwill begin with decision-making and its impact on interprofessional relations, best interest decision making for patients, the fact that interprofessional decision making is not easy, decisions made without considering the input of SLTs, parent’s values and perspectives about the decision as well as the differences in interprofessional decision-making. Shared decision making can assist in the creation of knowledge and bringing synergies that can influence patient care positively. However, an understanding of the use of shared decision-making in a critical care unit is rare. An exploratory study conducted on 22 team members of interprofessional groups explored the practice of shared decision making in Canada’s intensive care unit. Four key roles which participated in the shared decision-making were identified, including parents, clinical experts, leaders, and synthesizer. Shared decision making is achieved through collaboration, sharing and weighing of alternatives (Dunn et al. 2018). Different students can have different values related to their work and thus, during the initial working years, this can influence their decision making, as was found in a study conducted on 311 students (Nagao et al. 2017).
At decision-making process SLTs think, that confidence play an important role.This might be explain by Morison at al. (2011) mentioned that lack of knowledge on your professional angles, team roles and responsibilities would have a negative effect on professional practice and confidents. Morison at al. (2011) observed that when someone was newly qualified, confidence played a big part because sometimes they would have a lot to say but did not feel confident enough to say it, especially when there were expert peoplewho would have been working in the job for many years. They felt that when an SLT has confidence in what they are doing, their ability to voice their opinions on what could be right or wrong would be enhanced. The SLTs can look at how their skills come together to help the patient accomplish that ultimate goal. Thus, it is a nice place for them to realise that the team works together and that they are working on the common goal of patient satisfaction and patient quality of life. A research was conducted on 53 research professionals to identify their core competencies for shared decision making along with 16 older people. It explored their experiences to identify the key elements within a teaching framework.
The key elements identified included practical training, collaboration, facilitation, knowledge creation, and patient engagement. The framework was found to be very useful for clinicians and educators promoting SDM for older patients (Icon et al. 2017). According to the participants, SLTs did not have a say in the final decision making because they generally gave their perspectives about the clients’ head teachers, consultants or psychiatrists who took the final call. Some SLTs also highlighted their apprehension regarding the majority decisions because they felt that, in the end, everyone disagreed. Several approaches were used to arrive at a decision, which involved working in different settings, working with different needs clients, and working with diversity of professionals. They used terms like “you make that decision jointly together” and “make a decision from there jointly” to show interprofessional decision-making. Shared Decision-making (SDM) allows the influence of professionals and patients to rub off on each other while making health choices.
Thus, it gives individuals more control over the care they want to receive. SDM practice is embedded in several healthcare approaches. In addition, SDM is a dynamic process by which the health care and the patient influence each other in making health-related choices or decisions. It is also advocated as an ideal model since it provides individuals with more control towards the health care they choose to receive, and has also been shown to improve patient outcomes. However, there are rarely any studies that can prove the impact of SDM on the outcomes of patient care (Tousignant-Laflamme et al. 2017).This brings to the forefront, the significance of interprofessional working, which has been perceived as a balancing act specifically between traditional power holders and the other clinicians. Thirty six rehabilitation practitioners from Australia providing spinal cord injury repairs participated in a research experiment involving different control groups pre and post training (three and six months).
Ethical decision making was found to improve after the training within the control group, while no change was observed in the experimental group. In a more traditional structure decision-making, change could be devastating. Mono professional practice model was considered for a traditional system for SLTs by making or suggesting some changes for a newly qualified SLT. However, this process of monitoring was presented as unofficial, negotiated and context-specific. It should be understood that in addition to a clear need for more standardisation in various aspects of advanced practice, there needs to be an augmented value for the unique practices that were profession or role specific like the SLTs. The research found that whenever there was a meeting, especially regarding making a decision in situations of disagreement and conflict, the final arbiter would be the doctor since they are the ones that make the referrals.
Another barrier of interprofessional decision making was when clinicians made the decision without considering the input of SLTs. For instance, in a hospital, the doctor made environment based decisions. Participants mentioned that by using terms like “definitely an air of the medics have the final decision.” UK government encourages the healthcare staff in bringing collaboration in practice through appropriate policies. However, the impacts of these changes on staff and patient care are not fully understood. Studies have found some level of influence of professional knowledge and skills on interprofessional working in the healthcare unit (Brumfitt and Baxster 2008).
In a few examples, the SLTs mentioned that parent values and perspectives about the decision is important using terms like “if they're able to, and their families at least twice during their admission to discuss everything and set some goals.” In this context, social values theory was used to examine how parents make decisions for their adolescent children. Social values theory posits that decision making for others is premised on the social value of an action, which leads to a norm on how to decide for others, whereas self-decisions are influenced by a number of extraneous factors. Consistent with a risk-aversion norm, in hypothetical health and safety scenarios, parents made more risk-averse decisions for their adolescent children than they did for themselves. Further, the level of risk and inconvenience affected self-decisions more than the decisions made for one's child.
In diverse settings, SLT professionals work along with an array of other professionals. However, in community settings, there has been little research on SLT teams and also very little research is done on wider array of professions such as allied health. Specifically, the research has been insufficient on the interprofessional practices and SLT in supporting the children having disabilities with communication. In this context, IPCP can contribute to audiology departments, language and speech therapy.
Another study showed that the norm was stronger for decisions relating to one's child than for oneself and more related to the parents’ decisions for their child than for themselves. In sum, the parents’ decisions for their children seem to be largely determined by a norm stating how they are supposed to decide, at least within the domain of health and safety. Implications for both the judgment and decision-making and parenting literatures have been discussed(Dore, Stone and Buchanan 2014). The participants mentioned that sometimes their opinion about clients was not considered professional and sometimes, they did not know SLTs role with those clients. Some SLTs mentioned the fact that differences have a great impact on interprofessional decision-making; here, different perspectives and values could present great opportunities for joint decision-making. Shared decision-making plays a significant role in providing customer centric care in an interprofessional working. A study conducted on 31 healthcare service providers through semi-structured interviews identified specific barriers to shared decision making, such as mental health of patient and treatment given to them during the patient care service (Chong, Aslani and Chen 2013).We have discussed decision making process and types and their influence on to the relationships and negotiations. According to Some SLTs On the process of decision making and interprofessional team working there were some disagreements and conflicts which could have affected the negotiation and interprofessional relation. Next part will focus on to the conflicts resolution and theories behind that.
Most participants mentioned having a good working relationship with team members. Working in a team usually tends to have differences of opinion which need to be identified and resolved in several ways. Laschinger and Smith (2010) mentioned that authentic leadership and structural empowerment might affect interprofessional collaborative practice on nursing which means that new leadership will still need to be more group based and share power with other team members. According to SLTs, discussion with patients and professionals openly would yield mutually beneficial outcomes. Moreover, the difference of opinion could be resolved through voting. This is what was supported by most team members. Usually, this involved brainstorming the different ways in which targets could be met. The research data showed did not reveal glaring differences. The SLTs and the doctors had conversations where they determined whether something was good for the patient or not. The different people the SLTs work with are also influential in this parlance.
The majority of SLTs highlighted inhibitive outlook of doctors on collaborating, with lack of knowledge on the effect of speech therapy. The limiting factors to collaborative practice include multidisciplinary backgrounds of professionals, a lack of space, rooms, equipment and mismatch in the work schedules of all the professional i.e. cultural, diversity, and language, time and workplace-based. Time, place and professional culture has a great impact on interprofessional working which shall be discussed under the barrier of interprofessional team works later.
Hind et al. (2003) used three social psychology theories: the realistic conflict theory (Brown et al. 1986), social identity theory (Ellemers et al. 1999) and self-categorization theory (Turner 1999), in an inter-professional study involving five different professional groups. According to Reeves et al. (2007), discourse theory describes culture and language, whereas Foucault’s (1972; 1979) theories of social power, discourse, and surveillance have been used in inter-professional literature. This shows the implications of bureaucratic organizational structures and power within interprofessional communication. The organizational structure of NHS and Education services mentioned by SLTs also deserve attention. Power relations and leadership style had both positive and negative effects on interprofessional working.At this part we have discussed the disagreements, conflicts and arguments in interprofessional teams with the relevant theories. Next section will be discussed the power relationship between team members, leadership and hierarchy. Mostly, the SLTs think that they have worked at quite the same level, but they all assume different roles in the team. Being newly qualified professionals, working in medical setting sometimes causes hierarchical problems and conflicts. This section will be focus on the current research findings on leadership and hierarchy and discuss these findings within the relevant literature.Most SLTs observed that they all work at quite the same level with other professionals. They used terms like ““I think it comes naturally” and “I feel it is quite equal”, but they all have different roles in different teams which shape up their hieratical position and leadership issues. They used terms like “she was a central person that knew all these other people” to show that their respective roles shape up the hierarchical and leadership issues. In education settings, SENCO would be a leader in healthcare settings and in social care settings, more general physiatrist and even adult nurses could be a team leader in some cases. To improve the quality of healthcare service and make it affordable for patients, provisions have been made in the policies and practices, such as the emphasis on team based healthcare practice, mental health parity and service integration. Schools in the social sector have since joined other education organizations to explore shared learning practices. In social work, collaborative practice has been supported but in education, students rarely get opportunities to interact with other experts. Interprofessional collaboration has been considered as an increasingly important factor in the social workers’ works. With Canadian social work practitioners, educators and students, a focus group was conducted in identifying facilitators and barriers for collaborating from the social work perspective. There have been six themes identified by the participants acting as facilitators and barriers to collaborate: power dynamics, communication, decision making, role clarification, self-identity, and culture. These findings are the key implications in health practice interprofessional collaboration with social workers.
Social leaders have to address the needs of intersectionality between social factors as well as collaborative competencies. These competencies can then create opportunities for social educators as they pave the way for innovative IPE. An integration of this IPE in the school curriculum can bring in institutional benefits to an organization through the creation of a social work culture (Rubin 2018). A scoping study on the subject of leadership critically reviews 114 articles on interprofessional leadership in the domain of healthcare. Most of these articles covered in the research failed to provide clear definitions or theorisation of leadership capabilities in healthcare settings. The articles mostly explored leadership qualities in students, but did not explore actual leadership practice at higher levels in the hierarchies. Thus, the understanding on the use of interprofessional leadership in healthcare practice still needs deep exploration (Brewer et al. 2016).
Some SLTs are in a school every single week which becomes quite an uncomfortable environment, given that they have a huge caseload. This also eases the paths to be able to assess more children at one go. However, some other SLTs opined that some hierarchies were present in some settings. Distributed leadership models are often used in the healthcare sector and have been explored in several studies. However, the views of clinicians and other professionals have been rarely explored. Their beliefs about leadership can be associated with the team and their professional strengths. A survey conducted by Forsyth and Mason 2017 on 229 professionals in England on leadership beliefs found a positive association between the shared leadership and professional identification, especially in cases where participants had a strong professional identification. Thus, it can be said that strong team identification reinforces the spirit of shared leadership in people, but needs further examination of leadership practice (Forsyth and Mason 2017).
There has been another factor which caused power issues is banding system.In a banding system, the management is at the highest level and provides leadership and supervision in mono professional environments. The use of shared leadership models imparts specific benefits in healthcare, but only a few studies have explored the leadership benefits in the field. However, an online survey conducted on 229 healthcare professionals working in East England identified a positive relationship between leadership and professional identification in a single person. Thus, it can be said that strategies can promote personal identification and also help in shaping shared leadership. However, a research may still be needed to ascertain leadership practise in healthcare professionals to see this link in action. Personal identification and shared leadership still make two important concepts in the study of IPE (Forsyth and Mason 2017).As suggested by the participants, people at higher levels of management can provide guidance to those who are at lower levels of the hierarchy. Thus, it is important that their contribution in shaping a new person joining the sector be duly considered.To sum up at this section we have discussed communication skills and types, decision making and types with power relation, leadership, hierarchy, conflict resolution and theories behind them to help negotiation and relationship. Next section will discuss another important key findings which was mentioned by SLTs is professional identity and perspectives of SLTs about their professionals.
Professional Identity
According to current research, as a small group of professionals, SLTs feel more responsible about explaining their roles and responsibilities. This section will focus on to the explain about their roles, how they feel about their job,being not understood and what it is like to be an SLTs with theories behind their thoughts.According to SLTs, explaining their role to the other professional in an interprofessional environment is sometimes like “banging your head against a brick wall”.
The SLTs are very small and relatively lesser known professional groups. This caused some problems while working in different settings. Additionally, this adversely affects their professional identity and attitudes while working in different teams. There was a feeling of being forgotten or a lack of acknowledgement by other professionals regarding them. As stated before, this has been a recurring concern where the SLTs seem to have been acknowledged randomly without a uniform and standard attitude bestowed upon them, as would happen to someone like a nurse, a teacher or a doctor. They used phrases like “constantly been forgot about”, constantly been forgot about”and “newly qualified professionals, they don't understand our role” Other professionals showed a lack of knowledge or acknowledgment as medical professionals. The one category of professionals who acknowledged their clinical input was psychologists who consulted them for patient needs of understanding, communication, hearing, and swallowing. However, there was also evident lack of recognition with the SLTs not being called to attend meetings and such. It was observed that when working in a multi-functional team, some are very keen for speech therapy input and there are some that don't value the input of the SLT at all and do not consider it as an important part of someone's management, which makes it more difficult. For a team-based health care approach to be efficient, all team members must understand one another’s roles to maximise team collaboration and efficiency (D’Amour et al. 2005). There is also a global demand for quality healthcare which can be made possible only with a patient-centred approach. Thus, a culture of values and sound principles must be practiced in a healthcare unit by an entire team that serves the patient; collaborative practices can make that possible.
According to the SLTs, other professionals’ perspectives about their work have been an important factor for effective communication and interprofessional working.It was noted that some people do appreciate SLTs and some who do not. Interprofessional Education and Collaborative Practice approach improve team- based communication culture and foster an understanding of each other’s roles and responsibilities. In the current research, SLTs mentioned that knowing each other’s roles and boundaries had a great impact on their communication with other professionals.Thus, amongst the respondents, a majority of the health professional students who answered open-ended qualitative questions clearly showed a need towards the desire for respect for their individual points of view. Correspondingly, the findings of Lumague et al. (2006) suggest that IPE encourages and cultivates respect, thereby resulting inan enhancement in the knowledge of the diverse roles played by a multi-disciplinary healthcare team. Similarly, Suter et al. (2009) concur that respect and trust are enhanced and compounded amongst the team members with the development of a mutual understanding of each other’s roles and responsibilities. It was also evidenced amongst the research participants in IPE in the Senette et al. (2012), who employed simulation to extend support to handoff communication as well as teamwork initiatives. IPE was known to influence their responses to be an affirmation for positive collaboration, and intention-to-act with regards to the handoff communication.
This, in turn, translated to greater patient satisfaction. Thus, based on this finding, the researcher opined that IPE oriented activities can and should constitute an essential part of nursing and allied health professional educational curriculums, as corroborated by a previous relevant study (Titzer, Swenty, and Hoehn 2012). This viewpoint is agreement with the results of Baker et al. (2008); Dillon, Noble, and Kaplan (2009); and IOM (2010). These researchers acknowledged the use of simulation and IPE as an effective teaching strategy, especially with reference to early co-education of students from diverse healthcare field professions. In order to fulfil the demands of the curriculum, instructors are increasingly embedding IPE in the activities used for running their academic programs.
This integration is done at a small scale was one in class online activity is introduced to students, which in turn augments their perception about knowledge grasp (Wallace and Benson 2018). In social work, this integration is also seen in service provisions given that collaborative treatments are used for serving the patient care needs of children with delayed development. However, the literature still lacks information on the quality and quantity of such collaborative practices. A need for collaborative multidisciplinary services is clear (Edwards, Newell, Rich and Hitchcock 2015).In summation, as small health professionals, SLTs have to explain their work to other professionals and sometimes feel less powerful in team meetings.
Personalities
SLTs mentioned that different personalities comes with different atmosphere sometimes this influence their work positively sometimes it affected negatively. Some participants mentioned about the skills, team atmosphere, personalities and knowing each other’s roles and responsibilities which was congruous to the ten principles outlined by Nancarrow (2013). According to current research, SLTs mentioned the effects of different personalities on interprofessional relationships. According to SLTs, the types of ambiences were based on the types of people they were dealing with. The SLTs are exposed to challenging environments due to the multi-disciplinary nature work demands with diverse backgrounds individuals, requiring the qualities of an open-minded person, a very good listener and a patient person. These ranged from professional knowledge, experience and authority and power to discharging or retaining people in wards. Also, there was mention of cuts in funding to the services and how this impacted inter-professional relations as well as operations. Hence for an effective communication, it is imperative for the SLTs to understand the other person’s background.
These shared experiences can further lead to mutual understanding (Clark 1993). There have been some quotations on personalities of different professionals and how does this affects interprofessional team working. Rogers (1959) postulated the theory of therapy, personality, and interpersonal relationships, as developed in a client-centred framework, which was primarily concerned with personalities, behaviours, relationships and person centred care. According to the theory, there is a correlation between personalities and behaviours. Environments affect personalities and personalities affect behaviours, which then shapes attitudes. Different personalities within the team have some positive and negative effects on interprofessional team working. The SLTs think some of them are easier to work with than others. There tend to be individuals that the SLTs can feel they can get along with easily and with whom they have shared a good relationship with and they find those people easier to work with than those who do not prefer to include them in their personal lives as well; this in turn can make it a bit difficult to mentally get along with the whole situation.
There are some personalities who have a negative effect on to interprofessional working. This was evident in the tone of the emails, and a sense of passive aggression prevailed in the paralinguistic mannerisms shown by some co-workers. The participants used phrases like “tricky personality issues”, “those kinds of people” and “those are individual personalities.”According to Hall 2009 healthcare professionals have different values, culture, customs and behaviours that have effects their interprofessional relationships. Such as Professional culture comes with historical factors, social class and gender issues. Educational and training factors of each professional gave him or her a Professional identity and values which sometimes could be a barrier for interprofessional works. A study by Scott Reeves explores the role of ethics in collaborative practices. Some ways ethical issues can be addressed in these practices include creation of cultures that is inclusive of considerations of ethical reflexivity, use of self-surveillance in practitioners for achieving professionalism, and involvement of users for promoting collaboration. Overall, For the SLTs personalities have some positive and negative effects on to the interprofessional working. Personalities has been the final section of the experience of SLTs in interprofessional collaborative practice. At that section we have discussed SLTs experience in IPCP such as, complexity of their work and its effect on IPCP, negotiation and their interpriofessional relationship experience with identity and personalities. This section was answered the research question one. The answer of research question two will be discussed at next section which is the experience of SLTs in interprofessional education.
The experience of speech and language therapists in interprofessional education
The aim of this research question is to obtain an in-depth understanding of IPE as well as its impact on Interprofessional Collaborative Practice. There are several benefits of IPCP, as observed by McGrath (1991). According to the research, these SLTs were able to develop a basic overview of the process and there was an evident diversity in their individual perceptions concerning IPE. They developed an understanding of the input and significance of the roles of other professionals or collaborators, with a focus on teamwork. IPCP researchers have frequently focused on teams in acute care or medical and healthcare teams, for example, surgical teams (Kitto et al. 2013) as opposed to groups like SLTs. This section will focus on understanding IPE before discussing its benefits, the learning assimilated and finally focusing on the attitudes towards IPE.
Understanding of IPE
During the study, a majority of the participants spoke about their understanding of IPE. These subthemes will focus on the various perceptions as regards what IPE meant to participants, such as understanding of other professionals, explaining their roles to others, holistic perspectives, and seeing different views and perspectives. Quotation was deleted. This section will focus on the current research findings on understanding IPE within the context of the current literature. A research was conducted on the students of Nuffield Foundation, which explored the knowledge and skill levels of SLT professionals serving children during their early years of practice. Working together and taking training helped them gain extensive knowledge and improve upon their capabilities as found in the research (Hall 2005). Understanding the roles of other perspectives provides SLT students with a holistic perspectiveAlso, some SLTs were of the view that IPE workshops at universities worked at that time but not now, because real life is different from a workshop
Good for promoting SLTs role
The SLTs also felt that IPE was aimed at reducing team conflict when it came to working with groups. In addition, they opined that interprofessional environments give them opportunities to promote their job. Quotation was deleted. A lack of understanding into the roles of SLTs among patients is one issue, but when this information is also found lacking in other practitioners who may be serving the same patients, the problems tend to accentuate. It becomes a struggle for new practitioners to cope in such conditions and as a result, an awareness of their roles through IPE is the need of the time.
Good for understanding patient values
In addition, some participants mentioned that IPE gives them good opportunities to understand patient values. Quotations were deleted. Healthcare organisations with patient-centric teamwork practices have flattened organisational structures. Such organisations have healthcare settings that can facilitate the IPE practice of learning and serving. These organisations always seek team-based collaboration when providing healthcare, and positive impacts of IPE in teams is quite evident (Anderson, Gray and Price 2017). Through these responses, the SLTs presented a basic overview as regards the various perceptions of IPE’s interpretation of them. (i) IPE made them more knowledgeable to make others understand what their job description or roles entail, thus clarifying the functionality of SLTs as well as their contribution to the field; (ii) IPE process is fun while understanding is what IPE meant; (iii) IPE provided them with a clearer idea of teamwork as IPE was aimed at reducing the team conflict when it came to working with groups; (iv) IPE enabled them to have professional dialogues by getting them to learn necessary skills to adapt to and blend in with the others; and (v) some SLTs had negative views about IPE and did not find it very useful in light of the existing barriers with other professionals.
Thus, one unifying theme to emerge from the data was that current and future SLTs roles had a crucial part to play as regards IPE comprehension towards improved patient care. SLTs often drew attention to the lack of clarity with IPE and subsequent understanding of IPE’s significance. This confusion can be exacerbated with the emergence of SLTs along with their subsequent dialogues in the clinical settings with personals from different clinical professions, including physiotherapy, paramedics, dietetics, and radiography. The perception of the majority of SLTs was that focusing only on skills could limit the potential of SLT roles and lead to more entrenched professional groups. Analogously, the need for skills reflected the ‘reality’ of the ever-evolving demands of practising at an advanced level; some opined that the current role provision struggled to keep pace with such demands.
This necessitates the development of preregistration education as an important step for inter-professional collaborative practice. Lumague et al. (2006) conducted a study where the results showed that the collaboration affected the students’ skills, behaviours, and attitudes. In addition, Zwarenstein and Reeves (2000) completed a Cochrane review to determine “the efficacy of IPE interventions as compared to education in which the same professions were learning separately from one another.” The researchers proposed that mixed-method studies could provide some clarity for IPE, which in turn affects both practice and patient care. Meanwhile, Zwarenstein and Reeves (2000) advocated the view that studies in IPE generally focus on the different group's works and multi-disciplinary teams. In totality, according to current research findings and theories of IPE, it is apparent that IPE helps improve team collaboration and communication skills, knowing each other’s roles provides great opportunities for SLTs to explain their jobs to other professionals as small and unknowing professionals.
Benefits of IPE
According to the data collected from the research, the SLTs positively benefited from IPE through learning how to work with different professionals towards the improved success of SLTs. The results also revealed that the main area to focus for the SLTs is working together with other professionals. They also learned the art of team building and the ability to explain their functionality. According to this research, IPE created a bridge between diverse professionals and facilitated an understanding of different approaches and perspectives. McCartney (1999) suggests that between such radically different systems, it is surprising that effective collaboration occurs as often as it does, stressing upon the need for IPE. Most importantly, the SLTs learned a lot about how others think and what they do. The majority of respondents viewed medical problems through psychological and physical prism. Paragraph was deleted
The respondents also felt that IPE prepared them to work with a team where professionals came from different backgrounds. The most positive effect of IPE is that it clarifies communicating power to a great level whilst fostering team spirit. According to the data, IPE helps SLTs understand how to promote their own field and enables a cross-professional promotion through other fields.
Thus, they felt (she have put here how many), they were very lucky in that they could communicate with each other very easily. The data also shows that the most important thing is to understand their professional role and input, especially what their focus is when dealing with patients or service users. The idea is to develop and gain inclusion in key strategic multi-agency planning groups, requisite high-level negotiation skills, develop an in-depth knowledge of the functioning of different agencies, and build necessary skills to actively influence senior decision makers at a strategic level across agencies. Thus, the findings were positive as regards, the recommendations to sustain and incorporate IPE in the curriculum. It is imperative for the future studies to continue exploring the IPE and their subsequent linkage in the improvement of the patient safety outcomes. As per the findings, IPE evidences an increase in the attitudes and value towards other professionals’ roles. In addition, it increases the knowledge of healthcare teams to impact a positive change in terms of patient safety and patient outcomes. IPE can, in fact, contribute towards the creation of a safer health care system and a systematic way to integrate safety into the process of care (Donaldson, 2008).
Limitation of IPE
According to the research findings, (i) the lack of communication and information in relation to professional communications emerged as one of the major IPE deficits, with a total 18 participants out of the 25, mentioning this problem. It was felt that those who were aiming for a common good motive lacked proper communication and that their motives somehow became overlapped. This aspect was underpinned as the SLT group showed minimal involvement within case discussions. In addition, the IPE events did not have a lot of information according to SLTs, resulting in limited awareness of the SLTs. (ii) Also, medical and pharmacy students received more focus. Correspondingly, the SLTs felt that speech therapists were denied due recognition. SLTs in their minority status faced challenging situations when the pharmacists or medical students would not be too keen on working with the SLTs. Despite a good experience of IPE, several SLTs reported their acknowledgment by other professionals and painted a very practical picture for them. (iii) The SLTs felt that IPE did not really provide practical skills.
Also, it was revealed through the results that during interaction with the medical students and the pharmacists, they felt uncomfortable owing to their personality and how they communicated as a group.Thus, based on their responses and the findings, it is evident that the interventional planning for children and adults with speech, language, communication or eating/drinking needs should constitute a partnership with other agencies. Correspondingly, excellent communication and negotiation skills should be developed by all SLTs as part of their portfolio of leadership competence. Similarly, service delivery through integrated systems and processes has been conceptualised within Every Child Matters framework, as shown in the figure below. SLTs work not only with children, but also their families and other education professionals for the development of personalized strategies in supporting the individual needs of a child.

Figure 8.2 depicts the importance of integrating thinking at every level to provide an integrated package as an outcome to the child. Thus, the contribution of the SLTs as a part of the wider team working together to meet a child’s must be acknowledged in the professional space. Generally, service delivery potential streamlining for the child and their family is evident through the concepts of interdisciplinary and trans-disciplinary working.

Furthermore, At Figure 8.3 D’Eon (2005) opined that IPE and PBL learning situations promote effective teamwork through real-life contexts. D’Eon also noted that progressively augmenting the complexity of practice cases enhances the students’ ability to transfer learning into real-life circumstances. Such an approach necessitates an extended implementation of IPE as opposed to a “one-off” session or an optional extra. Analogously, as regards IPE, Barr et al. (2013) recommend that inter-professional initiatives should be tested “against…other theories, which may confirm or conflict” (p.7). Manwihile Hean et al. (2013) and Hammick et al. (2007) stressed on the importance of theory and pedagogy to the evidence base of IPE. Irrespective of the approach to skill mix and sharing of competence, the key role for SLTs as trainers and educators must not be ignored. In addition, Lindsay and Dockrell (2011) noted that collaboration requires shared responsibility and understanding along with limited authoritativeness. However, the term ‘collaborative model’ fails to deliver the key principles of transferring skills and competencies to others, particularly within a multidisciplinary team in order to support children more effectively. Byrne and Pettigrew (2010) highlight that the biggest barrier to collaboration in healthcare is a lack of knowledge about each other’s roles. Also, resource saving strategies is a typical outlook, towards service models, involving the delegation of tasks and programmes to others; fortunately, there are examples of positive models where others within the workforce around the child contribute towards the achievement of speech, language and communication goals. The positive models that work with children must identify the communication, language, speech, or drinking/eating needs of a child with reference to, or part of the appropriate multidisciplinary team.
What I learnt from IPE?
The most important skills learnt by SLTs from IPE are skills for working with different professionals in interprofessional team. With IPE, the SLTs also gained an understanding of how to work with professionals who were not qualified to understand various aspects of SLT duties to reduce the team conflict. This could be helpful in circumstances where their contribution is not recognised in the way that they should have been. This education also helped them provide others with a chance to understand their job description or roles, their functionality and contribution. Correspondingly, Craddock et al. (2013) stated that IPE needs to be mandatory in the pre-qualification phase of the curriculum. The response to this research question views the understanding of IPE and how IPE prepares them for Interprofessional Collaborative Practice. Mostly, SLTs opine that IPE has quite important outcomes for their practice. However, in their pre-registration phase,IPE was not a fascinating thing for them. Many of them do realise the importance of IPE at the point of registration into their practice.
The aim of IPE is improving the outcomes of the patient and the care quality. The interprofessional competencies and the interprofessional learning outcomes have had their inclusions in a number of countries’ social and health care professions' accreditation standards. While IPE can be taking place at any time in health professions curricula, the tendency of it is focusing on the clinical topics and professionalism rather than basic activities of science.
IPE involves learning about other people’s roles in the healthcare setting and an understanding of the broad framework that persists in the organization.
During the course of learning processes, it is not just the involvement of other practitioners, but also that of the patients and their families. In the initial days of learning, the SLT only gets to realise that the role of others is neither properly understood nor valued by them before undertaking IPE training, which opened up their mind set for accepting the collaborative environment in a manner that enabled them to become open to learning about others and understanding their connections with patient care service.While they are at the university, IPE workshops do not seem to be relevant for their course; it seems like fun time for them. However, when they started to work, they realised that the lessons were important and needed to be learnt. The research shows that SLTs had a basic overview of the process and that they had various perceptions regarding what IPE meant to them. The key takeaway included: (i) IPE made them more knowledgeable and they were also able to learn how to work in multi-functional teams involving psychiatrists, psychotherapists or even dieticians, thus introducing them to a broader framework. (ii) They also had fun while understanding the concept of IPE and showed great enthusiasm after their initial inhibition about the fact that they had a chance to clearly explain what their job demanded and how important the role of an SLT was with regards to the current scenario.Correspondingly, various studies have investigated the effects of IPE along with the use of simulation in health education, particularly as regards SLTs role, e.g., Scherer et al. (2013). The beneficial impact of these teaching strategies progressively evidences a continued utilisation to enhance imperative parameters like critical thinking, psychomotor skills, and communication. A paragraph was delated. Hence, their closed circle becomes broadened to a great extent and they needed an in-depth preparation before the interaction so that they could market their own field of expertise. They were more or less happy about the fact that they had a chance to clearly illustrate what their job demanded and how important the role of an SLT was in terms of the existing scenario. The qualitative findings revealed in this study clearly indicate that post the IPE experience, learning professional roles were better understood by the SLTs, which is corroborated by Gallagher et al. (2010). They conducted a study wherein in an interdisciplinary project, volunteer students were employed from Physician Assistants, Nursing, and Pharmacy programs; the researchers studied the impact of augmented understanding of strengths as well as skills of other members of the healthcare team.The SLTs learned a lot about how others think and what they do. That was probably one of the most useful things about all of it. It was about getting an understanding of where they were coming from. They mentioned that they remembered being in a group with social workers at university and that they quite enjoyed it, but did not really understand what the others did until they were involved in case studies. The research shows that they had to all look at the case studies from their own perspectives; hence, the speech therapists and social workers did the same since they all had very different perspectives. The findings clearly indicate the development of IPE and simulation as regards the importance of collaborative practice, with an aim to lower practice errors and bring about an improvement in the quality of care and patient outcomes. IPE extends a great leverage in the inter-professional teams being progressively involved in simulation, which remains a growing trend in healthcare education (Willhaus 2012).
In order to impact patient care, these programs combined efforts between medical team dynamics, including Pharmacy, Nutrition, Physical Therapy, and Social Work. Thus, it can be safely inferred that IPE offers a viable avenue for the evolving attitudes amongst healthcare professionals, aimed at the enhancement of patient centred care (Rodehorst, Wilhelm and Jensen 2005; Rose et al. 2009). Correspondingly, there is a growing acceptance of the utilisation of IPE and simulation within an academic setting amongst healthcare educators. Similarly, in early co-education of students, this use of simulation within IPE remains an effective teaching strategy particularly, in healthcare (Baker et al. 2008; Dillon, Noble, and Kaplan 2009). Similar to the findings of the current study, Giardino and Sigler (1994) posited that inter-professional education helps medical students work collaboratively with other professionals in inter-agency collaborative practice. Furthermore, they studied IPEs’ impact in gaining experience whilst working with other disciplines. Gallagher et al. (2010) opined that work results are concurrent with the findings of Rodehorst et al. (2005).
The current studyconfirmed that the interdisciplinary learning leads towards the clarification of professional roles and also in enhanced learning. It was found that concurrent to the study of Lumague et al. (2006), the SLTs in this study pointed out that all participants acknowledged the significance of interprofessional teamwork oriented towards patient care whilst congruently stressing upon the need for further education on the functional roles of other medical professionals. The SLTs also said that IPE suggested how they could team up with other professionals who were not qualified to understand the various aspects of SLT duties. The SLTS also felt that IPE was aimed at reducing team conflicts in groups. At times, some professionals would feel that their contribution was more important than others, but that they were not recognised in the way that they should have been.
The SLTs felt that this provided them with a chance to make the others understand what their job description or roles were. The practice started from there, what to and how to explain the way in which they operated and understanding what their contribution was in the field. IPE was also the reason why the SLTs learnt the art of adapting and blending with the others. Initially, some SLTs were apprehensive about the whole thing and doubted the potential benefits of IPE, but they began to enjoy their roles when the activities started to get engaging. Thus, the theory of IPE and Interprofessional Learning (IPL), along with the model of IPE, is imperative. Similarly, Petri (2010) observes that “an interpersonal process characterized by healthcare professionals from multiple disciplines with shared objectives, decision-making, responsibility, and power work together to solve patient care problems; the process is best attained through an inter-professional education that promotes an atmosphere of mutual trust and respect, effective and open communication, and awareness and acceptance of the roles, skills, and responsibilities of the participating disciplines” (p.80). The theory behind the IPCP is too complicated since it encompasses different professional fields and inter-professional backgrounds.
IPE as preparation for practice
The key expectations from IPE for the SLTs focus on the (i) specialist medical professions and their purpose with (ii) aiding them in bridging the gap within their knowledge levels with other medical students. This accorded SLTs with (iii) knowledge to collaborate with professionals in future and aligned with learning to communicate. In addition, (iv) the IPE events granted knowledge of detailed insights for individual aims of other professionals as regards affecting improved teamwork. Inter-professional education and training must first take place to ensure that all team members understand each other’s responsibilities, roles, and domains. (Connolly, et al. 2010) (vi) Given the importance of case studies, SLTs understood the diverse case management of each professional, thus providing SLTs with plenty of scope to have a better understanding of what they were expected to face in the future. However, (v) few SLTS differed in opinion during the research on any benefits from the IPE (vi) IPE also exposed them to audio-visual classes and they had the chance to interact with service users who shared their stories. The activities were more about understanding the exact role of the speech therapists and not restricted to what is generally taught in class.

The sessions also strongly emphasises on case studies and how every professional led with the cases in a different pattern as in the mode of approach of the different professionals. Practitioners were absolutely different from each other and this provided a lot of scope for the SLTs to have a better understanding of what they were to face in the future. The SLTs added that their interaction was also dependent on whether other professionals were interested in communicating with them and understanding their contributions in the field. A number of SLTs are also of the opinion that the activities did not help a lot because it was previously about collaborating with different professionals. However, in today’s context, they also had audio-visual classes and the chance to interact with service users who shared their stories. This nervous opinion changed to confidence after the IPE. This finding is concurred by Sinclair and Ferguson (2009).
In their study, amongst nurses, concerns were expressed about over-anxiety as regards the clinical practice application of their learning. Although there was a reported improvement in self-efficacy with particular reference to skill performance post-simulation experience, it was revealed through the findings that universally, there is ambiguity, lack of understanding and availability of variable role scope and definition as regards the SLT. In addition, the fact that this bridge can be addressed with the IPE is the common understanding reached between the respondents. The findings reveal an increased confidence among the SLTs with IPE, which are concurrent with van Schaik et al.’s (2011) survey oriented towards a simulation-based inter-professional team-training program that entailed interviewing health professionals with open-ended questions. The resultant themes from the study revealed an increase in professional roles’ understanding, debriefing value, and hands-on experience. At the same time, the study (Schaik et al. 2011) outcomes revealed an increase in self-confidence, positive attitude and a positive impact on self-efficacy.
Services user involvement in IPE
SLTs stated thatthe service users are also noted to have a positive involvement in the context of IPE. The SLTs stated that the service users mostly share friendly relations with them and provide a lot of useful insights to help the teachers interact freely with any children who need help, or with any patients who need to be taken care of. The SLTs have a fair amount of interaction with the service users. Some SLTs also have direct interaction with the parents of school children, which directed them towards their case studies. Thus, based on these findings, it is important that the SLTs be provided with a framework to support local service development and delivery. However, the current paper is not focussed to serve as a service-planning document. The aim of the paper is to capture and eventually disseminate the key principles that must underpin service commissioning and provision. Thus, it is believed that optimal utilisation of IPE with respect to service users will best meet the needs of children and adults alike with speech, language and communication needs. It has been observed that in order to provide effective support for children with speech and language impairments, interventions need to consider, according to Bloom and Lahey (1978), various approaches that address the entire communication context:
Children’s opportunities to communicate
Reactions children receive
Topics of currently available conversations
The language models (grammar, vocabulary, sounds) they hear
The modality used (adapted from Bloom and Lahey 1978)
Correspondingly, the concept of managing a child’s speech, language, communication or eating and drinking goals as part of their daily routine, and therefore undertaken by the people who are part of that routine, should be seen as a positive option. This is exactly where IPE comes into play. Notably, this is not a dilution of a specialist resource (Fey 1986), but the effective implementation of an IPE approach whereby individual child requirements are optimally addressed. Analogously, Freeth and Nicol (1998) used Kolb’s (1984) theory of experiential learning to enhance the clinical skills of final-year students as well as newly qualified nurses. Furthermore, Barr (2002) stated that the challenge of an IPE is a targeted outcome which also affects the outcomes for the service users of healthcare systems.
In addition, Owen et al. (2014) identified some limitations in existing IPE knowledge and published a list of collaborative care best practice models (CCBPMs) to address them. The process of developing CCBPMs includes various steps; however, learning theory drives this approach. As yet, no researchers have used such a model to develop an IPE program. Overall, we have discussed the experience of SLTs in interprofessional education with their understanding of IPE, barriers and benefits of IPE for them. How IPE prepared them for IPCP and how IPE activities helped them.
Next section will focus on to the using current research findings to develop an interprofessional education and practice model for SLTs.
How can we use this new findings to improve education and practice of SLTs?
Developing an interprofessional education and practice frame work discussed in interprofessional filed for years.There have been five different international framework used in interprofessional field to develop IPE/IPCP which will discussed later on recommendation chapter. According to current research findings the researcher will focus on the model which could show both side of the angel (education and practice). With that explanation the researcher prefer to use Canadian model for IPE/IPCP for developmening a framework for SLTs for education and practice. The reason researcher used that models because it has been more suitable for IPE and IPCP activities at the same time. As the researcher mention early chapters the current research give us an opportunities to see both side of the angel (education and practice). The section below will discuss the adaptation of Canadian model into education and practice of SLTs. Which has called Interprofessional Education for Collaborative Patient-centered Practice (IECPCP) model based on the research work done for Health Canada.
Adaptation a new model for interprofessional education and collaborative practice in speech and language therapy(was this part of the projects? What she write
This section will focus on the interprofessional education and collaborative practice models for SLTs according to the findings of the current research and relevant literature. There are some models which explain the process of IPE and IPCP. In this section, I will use Interprofessional Education for Collaborative Patient-centred Practice (IECPCP) model based on the research work done for Health Canada. I will re-organise this model in accordance to the SLTs’ education and practice. “This frame of reference can be seen as a first milestone in the development of this emerging area of inquiry linking interprofessional education with interprofessional practice.” (Oandasan, D’Amour and Zwarenstein et al. 2004 p.4); it is a framework which shows the education and practice system of interprofessional working. “This IECPCP framework should help to identify the determinants and processes that influence educational programs to teach about Interprofessional practice as well as the determinants and processes that influence the adoption of interprofessional practice within the health system.” (Oandasan, D’Amour and Zwarenstein et al. 2004 p. 5)IECPCP framework can be used for identifying the processes and factors that can create an influence on the educational program as well as adoption of IPE in the field of healthcare. It can also help in exploring the link between the two and understand the cross-fertilization process that goes between them.
This framework is defined using two circles, including one for IPE and the other for collaborative practice. IPE deals with the capability of learner gain competency through the combination of micro teaching, meso institutional, and macro systematic factors. The second circle also explores these factors but for processes and patient care outcomes. The processes defined during the second circle of the framework are complex since they involve an interaction between the views of different professionals. Patients are at the core of the collaborative practice that should be able to address the needs of patients through proper collaboration. The framework suggests that the practitioners working within a collaborative environment need to be exposed to IPE learning.
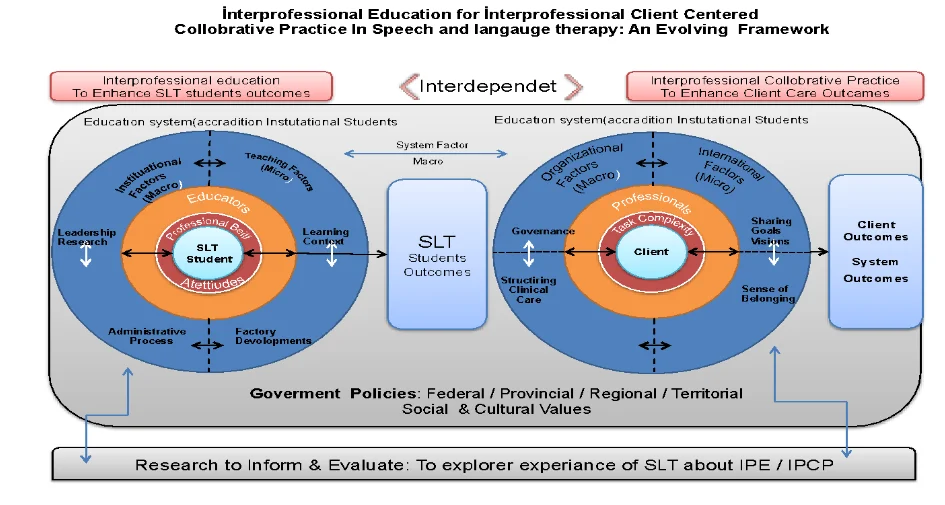
Interprofessional education model for SLT(how this related to your findings)
Pre-registration education is an important step for interprofessional collaborative practice. In this current research, SLTs demonstrated positive perspectives about IPE. The figure below shows the links between IPE and IPCP with different dimensions.

In figure 8.4 comprises of four circles; the first circle in the centre for SLT students, Second circle is about other students and professional identity of SLTs students in the interprofessional students group. The third and fourth circle is include current research findings themes and subthemes which related to the D’amaour and Quandesen 2004 models.It highlights micro (teaching level) meso (institutional level and macro (system level) factors. The learner is the centre of the education circle; the first circle is affected by all other circles and influences the ability of healthcare professionals. Oandasan et al. (2014) assert, “Interprofessional education to enhance learner outcomes highlights the learners as central to interprofessional educational processes” The interface between the learner and the educator is an essential aspect of interprofessional education. Within our framework, we situate socialisation issues as a key component that needs to be addressed in the development of interprofessional education. Socialisation here means that the professional and cultural beliefs/attitudes that develop among health professionals can affect their willingness to collaborate with other health professionals (Perkins and Tryssenaar, 1994; Zungalo 1994). Learners enter health professional programs with already formed stereotypes of their own professional identity as well as the stereotypes of others (Tunstall-Pedoe, Rink and Hilton 2003).Several studies have documented interprofessional education in health and medical courses. In this section, we will focus on the first circle which relates to IPE in the context of SLT. The middle of the circle is placed for SLT pre-registration students or learners.
The second circle around SLTs according to current research findings is other student’s attitudes and Professional identities of SLT students in their team. As well as in the original model which was done by D’amaour and Quandesen 2004 the second circle was about the Professional belif and attiteueds which was clearly match with the current research findings.Lumague et al. (2006) sought the students’ perspective of interprofessional experience, benefits, and challenges.The result showed that the collaboration affected the students’ skills, behaviours, and attitudes. With the IPE workshops, SLTs have learnt to collaborative work with other professionals as well. Current research suggests that there will be some IPE models for SLT courses; this section will illustrate a few model examples with the support of some findings in that research. Interprofessional Learning can be achieved using a variety of ways, each offering their own learning and practical benefits.
At the original model the third circle mentioned educators how every in this current research there was no mentioned on educators. Which clearly shows that educator’s roles in Leicester model of IPE was more facilitator level. It is more students centred IPE model. Which reflected at this current research. Also researcher put the related funding’s under the related maso level headings such as in the third circle under the institutional factors the research puts barriers of SLTs according to current research findings. Under the teaching factors benefits of IPE, under the faculty development preparation for the practice, under the administrative process understanding of IPE put by the researcher. The fourth circle on new model more policy level and more general cover in the original figure fourth circle and this circle was together however in this current adaptation researcher put general point in the fourth circle. Which was included the institutional factors, teaching factors, faculty development, structured clinical care, and organisational factors and all finding related to that (maso) level was put the third circle. The final elements in the original framework which was related to the current research as well is education outcomes for the learner or students. In this adapted model out comes of IPE for SLTs was mentioned there with themes in current findings. The major outcomes which we can put to the new model is IPE prepare SLTs to the interprofessional collaborative practice. Outcomes of IPE was discussed at previous chapter the researcher used original models out comes as a main base for his themes Such as, Knowledge, skills behaviours and attitudes. For the knowledge, skills and behaviours we can clearly see that SLTs have very positive change and learning outcomes from IPE. Also, their attitudes has positively changed by IPE and final and main outcomes id IPE prepared SLTs for IPCP. Next section will discuss the adaptation of the IECPCP framework models practice part with the reflection of the current research findings.
Interprofessional collaborative practice model for SLT
Frequently, SLTs work with different professionals with different sectorial backgrounds. Sometimes, SLTs visit a school two days a week and work in community health services for the next two or three days. Generally, SLTs have not got a permanent place to work. This will affect their team working and socialisation with other professionals. This section will discuss the collaborative working models for SLTs which is adapted from Oandasan, et al. (2004).
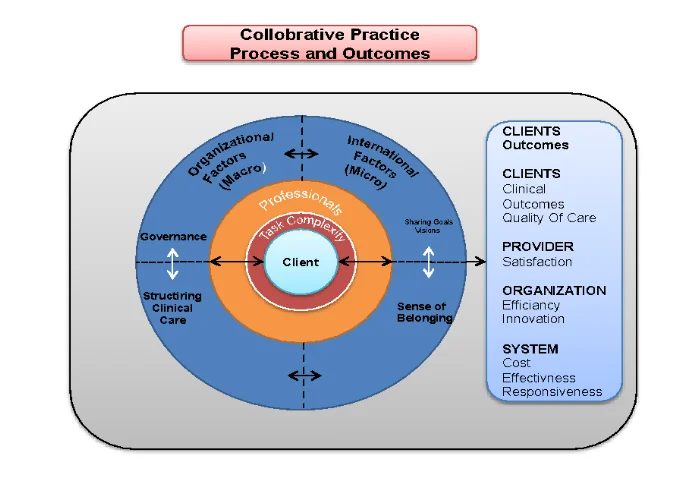
Here again, the micro (interactional), meso (organisational) and macro (systemic) factors are highlighted. At the centre of collaborative practice circle, patient or services users can be seen, which means that children with speech, communication and language needs would be in the middle of the circle. The second circle would comprise of professionals who involve the care of SLCN children, which in turn impacts the outcomes of SLCN care. In this circle, the process of interprofessional working seems to be working clearly. Patient or services users are located right at the centre. These circles are quite complicated because human interactions between professionals from different world-views take place within acomplex changing environment. Patients are at the centre, which means that his or her care outcomes are affected by professionals.For an effective patient centred model, the patient’s needs and wishes need to be addressed.
Oandasan et al. (2004) state, “Research, including evaluation, informs both interprofessional education and collaborativepatient-centred practice. It provides feedback that encompasses micro, meso and macrolevels and helps stakeholders bring improvements to both the educational and practiceenvironments. “For the current adaptation the researcher have patient, client, services user or students on the centre. This narratives clearly shows that SLTs used different terms for different clients because of their work settings. Second circle is professional identity. Which was clearly seen at the findings. SLTs mentioned their professional identity issues with the themes like how do you feel as a SLTs? How other professional seen you as an SLT. Complexity of the work was one of the other circle which was really shape the practice of SLTs. The final circle was about the more maso level such as under the organizational factors we can see the barriers of IPCP. Under the interactional factors we see the leadership, decision making, and hierarchy themes. Also we can see decision making under the structuring of the clinical care as well. Sens of belonging was one of the main themes mention by SLTs many times with themes like noting being understood and feeling as SLT. Finally the outcomes which mention in the original figure can be directly adapted here with the outcomes of SLT sessions to the clients, provider organisation and system.For an effective SLCN care, professionals needs to take accommodate the opinions of patients and parents along with their perspectives on SLCN care.In SLCN practice, decision making is influenced by the perspectives of children as well as their parents; this requires a practitioner to understand their specific roles in decision making. It depends upon the level of knowledge they have. This can be discovered through an active interaction between the practitioner and children or parents such that the information received from the interaction can be assessed to understand their preferences as well as awareness about the collaborative practice. The level of involvement on the part of children and their patients in this decision making needs to be decided before their views are considered in the decision making process. This involvement can require a practitioner to take short term steps and understand the nuanced targets for healthcare in collaboration with them. Further, the children and their parents must be informed about the level of involvement they would have during the decision making process, which can help bring about improvements in practices.
Summary of the chapter
The discussion clearly highlights how effectively collaborative practice contributes towards the achievement for good practice and team working by SLTs. The diverse barriers in addition to the facilitators of collaborative practice have been identified within this section, with an in-depth analysis of the findings sourced from the respondents to the interview. This study apparently bridges the evident gap with the emerging research focusing typically on medical professions with an emphasis on the significance of collaborative practice for allied health professionals. Through the use of semi-structured interviews, relevant data was collected through responses, which were then analysed qualitatively using thematic analysis.This discussion indicates that the participants in this study regard collaborative practice as being significant for effective practice, particularly for delivering the required intervention. Typically, the participants described their role as a provider and receiver of information about a case, albeit as a provider of skills. This in turn evidenced a lack of inclusion of the SLTs collaboratively; this lack of reciprocity may be an additional barrier to effective working relationships. Participants emphasised the need for better links between theory and practice in teaching collaborative practice, and were disappointed by the variability of opportunities to experience such collaboration. It was also felt that enhancing the value of collaborative practice could be addressed by examining it in congruence with the clinical skills. Additionally, engaging with other professionals through case-based clinical interventions could make sure that all SLTs have equitable opportunities to experience as well as develop skills in collaborative practice. A sentences deleted It also serves as a preliminary study to enrich the understanding of the beliefs of newly qualified SLTs with regard to the current teaching of collaborative practice and demonstrate how learning opportunities can be enhance.



- 24/7 Customer Support
- 100% Customer Satisfaction
- No Privacy Violation
- Quick Services
- Subject Experts