Market Equilibrium: Supply and Demand
Question 1
1. Briefly describe the conditions which must be met for a market to be in equilibrium.
In a liberal market, which is characterised by a perfect competition, the laws of demand and supply of goods and services determine the equilibrium point, or rather the equilibrium price of goods and services. In markets, equilibrium is attained at the price where the volume of demand and the quantities of supply are equivalent. In most cases the equilibrium point is epitomised in charts that show a point where the price and quantity where the supply and demand curves intersect (True et al. 1999). For instance, in a case example where a pizza maker is willing to sell his commodity at two large pieces at a price of $10 for all the pieces. If consumers are willing to buy the two large pieces at $10 then the equilibrium price in the market for two large pizzas would $10. Which implies that 2 pizzas are equivalent to $10.
Any imbalance in the market will create disequilibrium in prices, and at the end there would either be surplus supplies or shortages in the market. Surplus in the market exists when the price is above the point of equilibrium, which would encourage suppliers to lower their prices to reduce the surplus. At the same time, a shortage takes place when the price is below the equilibrium, which will drive the suppliers to increase the prices of their goods. These shifts from the point of equilibrium is determined by the changes in the demand and supply, which would lead to a new equilibrium price and quantity.
Looking for further insights on Private Housing Markets? Click here.
In cases, where there is a shift in the supply or demand, the pre-existing prices will not form the equilibrium. Instead, a shortage or a surplus will exist and these prices will subsequently adjust themselves to point of new equilibrium. For instance, with the inversion of the COVID-19 more people are willing to buy face mask and hand sanitisers at all possible prices, which has caused the demand of these commodities to increase. If these commodities are to be sold at the original price, then there will be a shortage of hand sanitisers and face mask, which is a signal that the seller ought to increase the price of the units until the quantity being supplied and the magnitude of demand are again equal.
Dig deeper into Demand and Supply with our selection of articles.
2. In a market for health that does not meet the conditions for equilibrium it leads to a market for health insurance. Describe adverse selection in the context of a health insurance market
In the health sector equilibrium leads to some sort of certainty in terms of the services that people expect and the money that they are supposed to pay for these services. An imbalance in the existing equilibrium leads to various instabilities in the healthcare industry, which posses market threats, most health care insurers take a defensive side in cases of a disequilibrium in the health market when it comes to insuring people. Health care industry professionals match their projections on market trends to their goals and the strategy of the business. Changing these rules of engagement within the healthcare industry also leads to disequilibrium that is likely to harm the care industry consumer. As an outcome of taking a defensive line in the provision of healthcare insurance services, insurance companies are likely to raise their premiums for consumers across the market, fail to cover risks that are perceived to be high risk and reduce the rates of reimbursement to various providers.
Factors such as increased government regulations lead to the current changing nature in the healthcare market equilibrium. In the short term, disequilibrium in the health market leads to increase in the cost of guaranteed care in cases where preventive care is not effectively followed by the consumer market. In the long-run, guaranteed care will lead to the stabilization of market costs since healthcare will spread across the range of whole life care as opposed to the periods of illness. Consumers of healthcare services are therefore forced to accept the prompt changes and threats in the industry that are characterised by increased cost of health services and limited supply of these services. Conservative slants to healthcare like making sure that there is adequate preventive care, can help in cutting costs drastically and protect the consumers from the sudden changes in the cost of health services.

3. What are the advantages of the Beveridge model of health care?
According to Beveridge, very citizen is entitled to the healthcare, and perceives healthcare as aright and not a privilege. Countries such as Japan, Cuba and China among others have embraced this model and some of the benefits enjoyed by these companies include universal access to healthcare, because every citizen has an equal access to healthcare. Secondly these governments have the responsibility of providing healthcare to their citizens. The fact that the government is responsible for the quality of healthcare acts as an incentive for the healthcare industry to provide its services at a cheap or subsidized rate.
In short, people in these countries enjoy low healthcare costs. Unlike in other countries where citizens are exposed to cost-sharing by their governments when accessing healthcare, the systems in countries that have embraced the Beveridge model are not liable for any co-payments or medical bills. Lastly, the Beveridge model ensures that health services are controlled to point where at no point the health sector faces imbalances unless in unavoidable circumstances such as during an outbreak of an epidemic or when the government changes its health policies. The certainty created by the Beveridge model creates a sustainable environment for everyone in the country, especially those with chronic or re-occurring conditions that would need continuous services.
4. What is one advantage and one disadvantage of the “Fee For Service” system to pay doctors
The Fee for Service system is mainly flexible in its operations. A patient can visit any medical provider at any preferred medical institute without seeking government or authority approval to do so. Patients are likely to receive highly valued services and at the same time the provider is capable giving suitable recommendations where they feel it is necessary to do so. At the same time doctors can charge a justifiable amount for a plan and can always be ready to offer specialized attention and services to their respective patients. One major problem with the Fee for Services System is that the patient is likely to incur more costs, than those in medical plans. The case is even worse when the customer has a recurrent or chronic condition, where they will need to visit the doctor regularly. In such a case, most people are likely to run out of money to carter for their medical fees and thus end up dying because they lacked the necessary resources.
Question 2
1. Choose a perspective for this economic evaluation and briefly justify your answer
Societal perspective; this perspective offers decision makers and economists with a wide possibility of understanding the costs and effects of alternative services or products as well as the related outcomes. Using such a wide range of thoughts would permit policy makers to examine the effect of a healthcare intervention on improving productivity on the welfare of family members. It is through this way that policy makers can gain consistency between the necessary decisions that ought to be achieved in healthcare interventions, which will result in investing in an appropriate project.
2. What figures are missing from the table (indicated by A-F)
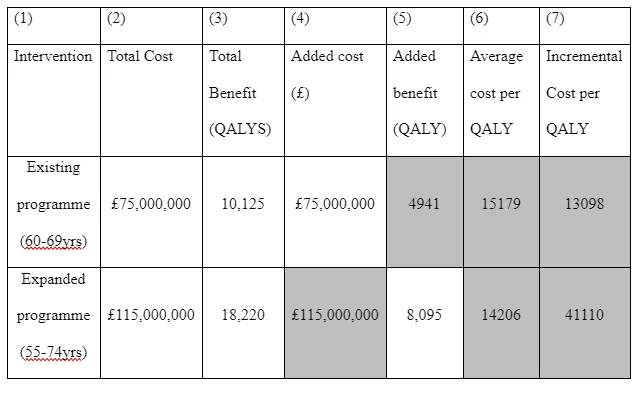
A= £115,000,000, If the total cost for the existing program was £75,000,000, same to its added cost, then the added cost of the expanded programme is also the same. B= Total Cost of the expanded programme-Total Cost of the Existing Programme/Total Benefit of the expanded Programme-Total benefit of the existing Programme
115,000,000-75,000,000/ 18220-10126
=40,000,000/8095
=4941
C= 75,000,000/4941
= 15179
D= 115,000,000/8095
=14206
E= 115,000,000-75,000,000/8095-4941
=40,000,000/3154
= 13098
F= 115,000,000-75,000,000/15179-14206
= 40,000,000/973
=41,110
4. Based on what information from the Table would you make a recommendation to NICE about the screening programmes? Explain your reasoning behind your answer.
The screening program has a positive recommendation due to the fact that the benefits offered by the healthcare services tend to outweigh the cost of receiving the services. It is an indicator that the screening process is efficient in ensuring that the needs of its consumers are met, at a price that most consumers are willing to pay. At the same time, the low costs of services is an indicator of efficient services in the healthcare process, hence lower production costs and subsequently lower services fees (Ordover, Saloner, and Salop 1990). At the same time, the society stands to benefit more from the programme and hence reinforcing the societal outlook that is needed for a project to reach out to a huge number of consumers as compared to projects with economical perspectives.
5. In economic evaluation, costs and benefits are discounted. What are the reasons for discounting and what are the implications of discounting on funding decisions?
The process of discounting helps in presenting the value of payment or a stream of payment that is to be attained in the future. In regards to the fact that the value of money is dependent on time, that is a dollar is worth today in comparison to its worth tomorrow. Therefore, the process of discounting helps to determine the value of the dollar today in future. The approach is majorly used to determine pricing streams of the future cash flows. The use of discount rates in cost benefit analysis is crucial due to the fact that high discount rates tend to result to lower values of benefits, which accrue after longer periods, and would result in giving more focus to interests of the future as compared to current interests (Drummond, Sculpher, Claxton, Stoddart, and Torrance 2015). The fact the discounting evaluation system majorly extrapolates its outcomes from the current generations outlook, the evaluators ought to focus on the inter-temporal issues on equity, which involve the fairness of the current decisions to those people who would be existing in the future. The benefit-cost analyses do not majorly focus on inflation due to the fact the projection of future prices would lead to unnecessary uncertainty into such analysis. Thus, discount rates are majorly based on the rates of interests for government borrowing, which has reduced risk in regards to doing away with the inflation and interest rates.
Question 3
1. A health state has a utility value of 0.6. Life expectancy is 15 years at this health state. Calculate the number of expected QALYs
QALYs helps to quantify the value of health results. The approach uses the assumption that health is a result of length and quality of life, and integrates these values into a simple index number. For one to determine QALYs, they would have the multiply the utility value with the appropriate state of health lived in the same state. One year of perfect health is worth 1 QALY. A year that one lives in a less perfect health shape is quantified to be less than 1 QALY. Therefore, in this case the utility value is 0.6 (less than 1 QALY, which implies that the patient is not living a whole year perfectly). To get the number of expected QALYs, it would be 0.6*15= 9 QALYs.
2. What are the benefits of using the QALY concept in an economic evaluation?
The QALY model gives consistency and helps to reduce budgetary waste. The QALY system is based on utilitarianism, which is founded on the principles of the greatest good for the greatest number of people. It implies that the QALY model majorly focuses on benefiting everyone within the society, and therefore its evaluation is focused more social empowerment or what can be referred to as distributive justice. It helps to give a direct contrast of interventions in a common currency and platform despite the clinical discipline. It majorly due to the fact that the cost per QALY does not confer the price of treatment but the price of resultant outcomes in terms of the quality lost or gained (Furlong, Feeny, Torrance, Barr, and Horsman 1992). Through the QALY evaluation an expensive treatment could have a low cost per QALY in cases where it leads to significant benefits to its patients. At the same time a relatively cheap treatment could have a high cost per QALY if the magnitude of benefits is relatively low. It implies that QALY is more efficient when setting up health priorities in a state.
3. Explain how we use the cost-effectiveness plane to present results of a cost-utility analysis
Cost-effectiveness plane present the results of cost-utility analysis graphically as a combination of the costs and the impacts of a health intervention in comparison to an alternative, which could be a different intervention (McClellan and Staiger 2000). The costs incurrent are majorly placed on the north-south (top-bottom) axis, while the impacts of the intervention are placed on the east-west axis. In both cases, such impacts can be negative, positive or have no effect (zero) as shown in the diagram below
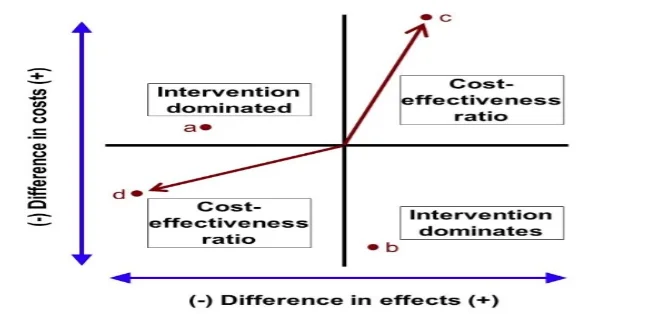
A treatment plan could be located on the diagram as per its incremental costs and the necessary benefits. If the treatment plan lies in the top left section like in point A, then it means that the cost of treatment is more expensive than its substitutes, which renders its benefits very low to the people, or in other words it is worse as compared to its interventions, thus it ought to be rejected. At the same time, if a treatment is placed at point B, then it implies that the costs of treatment is lower while its benefits are higher as compared to its alternatives. Thus, the intervention is more efficient and ought to be accepted.
4. What are the strengths and limitations of the standard gamble and time-trade off methods for eliciting utility values of health states?
Strengths of the Standard Gamble
The standard gamble approach helps health economists to asses various health utilities of various states and acts as a platform for comparison across various populations and various clinical settings. These health utility metrics are crucial as measures of outcome for the quality of life and contribute to the depth of knowledge in health economics
Limitations of Standard Gamble
The model does not consider baseline health status and could encourage the various health inequalities among various groups. The standard gamble approach assumes that there is no other objective to health care than death or health maximization. The options presented by the standard gamble approach are crude leading to the questions on what is quality care means to humans (Leal, Luengo-Fernández, Gray, Petersen, and Rayner 2006). The model majorly favours those people who have treatable condition and those with greater potential for life in regards to longevity as compared to those who do not have the same qualities.
Time trade off method
The approach helps economists to evaluate various decisions that people would make on their health after a prolonged period. The approach leads individuals to imagine living in a certain health state for a longer period like 10 or 20 years, and then derive the shorter amount of time that they would spend in full health (Banks and Sobel 1987). The approach is very efficient in valuing health status. However, when individuals are prompted to consider living in poor health states that are characterized by pain or immobility, they might not like such conditions that they could opt to trade of all their time to full health. In short, some people would prefer to be dead that to undergo such experiences.
Question 4
What are the strengths and limitations of using a cost-effectiveness analysis approach to evaluate public health interventions?
Advantages of Cost benefit Analysis
The main strength of the cost-benefit analysis is that one is assigning numerical values on all costs and benefits that are related with a medical plan, even the non-physical ones. Through using numerical values, one can calculate whether the project is justifiable by assessing whether its benefits are more than the cost. Secondly it can help in making transparent decisions that other projects can also use the same results to assess their respective outcomes (Cutler, 2003). Majorly the cost-benefit analysis is applicable to various healthcare products in regards to helping them in weighing various investment opportunities, examining the change initiatives and making future decisions.
Limitations of Cost-Benefit Analysis
The most prevalent limitation of the Cost-benefit analysis is the fact the accuracy of the data collected can be guaranteed. The inaccurate data could be analysed and the results could be manipulated to confirm various biasness of the researcher. What challenges might economic evaluations of public health programmes or projects experience? In the public health sector, it can be difficult task to conduct a full economic evaluation of programs, projects and services that are used in the sector. In most cases, the information on resources and their associated costs is very difficult to collect, at the same time most staff that the under economic valuations do not have the relevant skills or enough time and the appropriate resources to support the type of work they do. The long run frame over which the impacts of public health systems are likely to have an effect also ensures the measurement of benefits challenging, and potentially necessitates the use of discounting to mirror the fact that individuals place greater importance on the benefits they derive from healthcare systems in the short run as compared to the long run benefits (Cookson, Griffin, and Nord 2014.). It is for these reasons that there is limited high quality economic evidence in various areas of public health that would inform the process of decision making. Other challenges include the difficulty in assessing various costs particularly when interfacing with other sections like social services and education and various possible perspectives on the cost spend and various savings that were made (Sorenson, Tarricone, Siebert, and Drummond 2011). The expenditure of resources in one area could lead to more savings in one area as compared to the other, for example providing pre-walkers for the elderly in their houses could reduce the rates of falls and as an outcome, it could lead to fewer hospital admission rather these savings could be superficial care as opposed to public health, and in the long run there could be benefits accrued from the system.
Willingness to pay is phrase used to imply to the highest cost a consumer would be willing incur for one unit of goods or services. Willingness to pay (WTP), is a crucial element of consumer demand and is a crucial knowledge for a business in the process of product pricing. In this framework, the demand of the product or service is used a key indicator for determining the best price of a commodity or service, which helps to satisfy both the suppliers and consumers when the good or services goes to market. WTP is crucial for finding the best price that one would use to sell both a product or service. Establishing a happy point between the two entities ought to be reached between the two entities to make a sale. WTP is relative based on various factors, although it is among the best ways of conceptualizing the overall demand at any given time. Because of this variability, WTP is normally articulated as a collective number with a conforming range of lower and upper limits.
II. How do you estimate WTP?
There are various techniques that could be used to estimate the customers’ willingness to pay for a product and even asses the characteristic of the product. One of the simplest ways to determine the customer’s willingness to pay is by simply asking the client how much they would be willing to pay for the product. However, more accurate and sophisticated approaches like the revealed preferences that is majorly used for products that already in the market can help in revealing the customers willingness to pay. Other approaches such as the discrete choice which is more valuable for new products. Besides, the two approaches, companies need to have a good grasp of their potential market size. Such knowledge will help the company to determine its customers WTP and their future expectations. As per the sources available in a market a firm can use the historic data size. Therefore, the past historical data can help in estimating the future trends in terms of WTP. Price elasticity is another approach that can be used to estimate WTP. Every customer has their specific WTP for a particular product (McClellan and Staiger 2000). Naturally, one would use surveys from customers to establish and construct the client’s graph on WTP and volume. When this is not possible an aggregate of customer segments could be a better section approach. The objective in this case is to construct a demand and curve graph that would depict how many clients would be willing to buy a certain product and at what price.
Question 5
1. Describe marginal cost and marginal benefit
Marginal cost implies to the increase or reduction in the cost of producing an extra unit of goods or offering services to an extra client. In some cases, it is referred to as incremental cost. Marginal costs are normally based on the expenses incurred during the production process such as labour, purchase of materials and equipment. Other types of fixed costs involve administrative and overhead and marketing and promotional activities that remain the same despite the number of units produced or clients served. On the other hand, marginal benefit is the maximum number of clients who are willing to pay for an additional service or good. It also revolves around the extra satisfaction or benefit that clients receive when they purchase additional good or service. The marginal benefits of consumers tend to reduce as the rate of consumption of a good or service increase.
2. How would you reallocate resources between Programme A and B and when would you stop the re-allocation process? (200 Words)
In this case the project B would need more resources, this is because more resources on program B would help the project to achieve various economies of scale, which will make the project to produce more services. In projects with higher marginal costs, workers would learn on how to move from one task to the other, which means that more goods or services will be produced. As more goods and services are made in the same period, the costs associated with the process service delivery and goods production reduces. The costs of service production and materials could go down as more clients access the services. Therefore, in the long run, the cost of services will be low to a point where it can be afforded by most people. When the price of the services is low to point that the cost of product or service production is more than its market price, then the re-allocation process ought to be ended. If not, the industry would lose its profitability and the necessary incentives to attract service providers, which is a recipe for the collapse of the industry. Therefore, to avoid such negative outcomes it is important to stop re-allocation as soon as service provision is at point where it is can be afforded by most people in a population and at the same time the industry is still profitable to its service providers.
3. Why would you reallocate resources in this way?
The other option presents a case of marginal benefit, which usually declines as consumers consume more of the service. For instance, if a consumer needs a product for $50 and finds a perfect product for the same price (Cutler 2003). When the same consumer spots the same product for $50, they would not need it because they have one of the same values. However, they might be convinced to buy another for a lesser price of maybe $30. Thus, her marginal cost reduces from $50 to $30. Another perspective is on satisfaction it means one product or service would make a client satisfied, however second one would make them happy, but not as happy as the first one. The reduction in appeal is referred to as diminishing utility. Therefore, investing in project A would lead to diminishing utility in the long run, while investing in project B would lead to increased service accessibility and availability.

4. State the assumption that lies behind your thinking?
The cost-benefit framework has a ceiling methodology, that is any event that causes the consumers to buy services or goods in bulk leads to a reduction in the price, which is good for healthcare provision. At the same time, production of goods and services can go up prior to fact that machines and the service providers are exhausted. It the implies than new projects ought to be established or new workers ought to be hired. However, establishing a new project would only be justifiable if the demands of consumers continue to rise. In healthcare, lower medical expenses are likely to attract more people, and according to the utilitarian theory (the greatest good for the greatest number of people), lower medical fees would be beneficial to the community. Therefore, the assumption is that more resources would lead to the industry enjoying economies of scale, which will lower the production cost and the prices of the service. The lowered prices will attract a larger consumer base who will be able to afford to services and products. Since the industry experiences economies of scale and bulk buying the end result would be more decreased service prices.
5. Describe the purpose of the programme budget developed within a PBMA exercise
Program Budgeting and Marginal Analysis (PBMA) is a system that helps decision makers in the United Kingdom to maximize the effects of healthcare resources on the needs of local population or meet other goals like the consideration of equity. At the same time program budgeting is an assessment of the previous allocation in specific programs with an objective of tracking forthcoming resources in same packages. On the other side, marginal analysis is an assessment framework that focuses of the additional costs of proposed investments. The process of PBMA needs information on expenditure by a project such as the yearly budget, the number of employees and the targeted population. The PBMA exercise helps to estimate various health services such as maternity services, surgical services, and chronic patient care.
Dig deeper into The Debate on Democracys Impact on Economic Development with our selection of articles.
References
- Banks, J.S. and Sobel, J., 1987. Equilibrium selection in signaling games. Econometrica: Journal of the Econometric Society, pp.647-661.
- Cutler, D.M., 2003, January. Employee costs and the decline in health insurance coverage. In Forum for Health Economics & Policy (Vol. 6, No. 1). De Gruyter.
- Drummond, M.F., Sculpher, M.J., Claxton, K., Stoddart, G.L. and Torrance, G.W., 2015. Methods for the economic evaluation of health care programmes. Oxford university press.
- Furlong, W., Feeny, D., Torrance, G., Barr, R. and Horsman, J., 1992. Guide to design and development of health-state utility instrumentation (No. 1990-09). Centre for Health Economics and Policy Analysis (CHEPA), McMaster University, Hamilton, Canada.
- Leal, J., Luengo-Fernández, R., Gray, A., Petersen, S. and Rayner, M., 2006. Economic burden of cardiovascular diseases in the enlarged European Union. European heart journal, 27(13), pp.1610-1619.
- McClellan, M. and Staiger, D., 2000, January. Comparing the quality of health care providers. In Forum for Health Economics & Policy (Vol. 3, No. 1). De Gruyter.
- Sorenson, C., Tarricone, R., Siebert, M. and Drummond, M., 2011. Applying health economics for policy decision making: do devices differ from drugs?. Europace, 13(suppl_2), pp.ii54-ii58.
- True, J.L., Jones, B.D. and Baumgartner, F.R., 1999. Punctuated equilibrium theory. Theories of the policy process, pp.175-202.



- 24/7 Customer Support
- 100% Customer Satisfaction
- No Privacy Violation
- Quick Services
- Subject Experts