Coronary Heart Disease among Adults
In the current state of health care systems, the prevalence of diseases and other related conditions has been associated with risk factors such as the people’s nature of lifestyles and socio-cultural forces or barriers to access. This paper presents an urban healthy profile of the coronary heart diseases, with a specific focus on the adult population in Leytonstone Ward, London Borough of Waltham Forest. According to Townsend et al. (2012), the coronary heart disease (CHD) refers to a condition in which plaque, a waxy substance, builds up in the patient’s coronary arteries. Some of the risk factors associated with this condition include ageing, gender (in which men exhibit a greater risk), obesity, diabetes, high levels of blood cholesterol, smoking and family history.
On the other hand, signs and symptoms include chest pain (angina) and pressure in the back, jaw, neck, arms, and shoulders (British Heart Foundation 2014). In the UK, CHD has been reported to account for over 73,000 deaths annually. In addition, angina has been documented to affect about two million people while about 2.3 million people live with CHD (in the context of the UK) (Lim et al. 2013). It is also worth noting that about one in ten women and one in six men died from CHD. With this trend, it becomes imperative to examine the urban health profile on CHD among adults in Leytonstone Ward Borough of Waltham Forest. In so doing, it is projected that valid conclusions and reliable recommendations will be made to inform the neighborhood’s health care systems about potential interventions that could reverse the situation; as the Department of Health, UK Food Standards Agency (2014) observed that there is a direct relationship between healthy populations and improved economic performance.
Seeking healthcare dissertation help may also be beneficial in exploring the complexities of such public health issues. The paper is organised in such a way that the neighbourhood’s profile is provided, followed by the rationale explaining the importance of the selected urban health issue, the observations made, an analysis of these observations, and a conclusion and recommendations regarding some of the strategies that could be adopted to reverse the adversities resulting from CHD among adults in Leytonstone Ward.

Neighbourhood Profile
Recent statistics indicate that the population in Leytonstone Ward lies at 11,284 (Department of Health 2012). In addition, the ward’s demographic profile is similar to the rest of Waltham Forest in which the ethnic minority origin and Blacks constitute 55 percent of the residents. Specifically, the largest ethnic minorities in Leytonstone Ward include Indians at 8.6 percent, other white backgrounds at 8.7 percent, and Pakistani at 9.2 percent (HSCIC 2013). Similar to Waltham Forest’s mean age of 34.4, Leytonstone Ward is documented to have its population’s mean age lies at 34.2. However, the percentage of young populations is the lower and is reported to be 26.4 percent while a comparative deprivation is evident in the ward; ranked 150 out of London’s 627 wards (Townsend et al. 2012). In terms of healthy, major issues that have been reported at the ward level include drug and alcohol use, smoking prevalence, well-being, and the issue of weight. Some of the provisions and facilities in existence include Henry Reynolds Gardens with a basketball court near the high road, and indoor sports courts. Lastly, health support and advice is offered at the Ashiana Network, a charity-based firm that offers counseling and information to those who are at risk and disadvantaged (British Heart Foundation 2014).
Continue your exploration of Heart Failure Mechanisms with our related content.
Rationale
An understanding of CHD in Leytonstone Ward is important for various reasons. For example, an examination of trends in CHD will aid in informing about some of the policies or strategies that could be developed, adopted, and implemented in terms of early interventions and prevent some of the adversities associated with the condition. In addition, an understanding of some of the barriers to access among populations in the ward will inform about some of the steps that the public and private sectors or organisations could adopt and facilitate programs such as community sensitisation, seminars, and conferences, upon which the people’s lifestyles that puts them at risk might be adjusted towards better health outcomes. It is also worth noting that this paper is important because it will give an insight into some of the secondary contributors that complement mortalities and comorbidities arising from CHD, upon which corrective mechanisms will be recommended and allow relevant authorities at the local, regional, and national levels to engage in the implementation process and save lives of thousands of patient groups while restoring high qualities of life among the affected populations (such as the patients’ families). Lastly, an understanding of the state of CHD in the selected neighbourhood is important because, as mentioned earlier, a healthy population is associated with better economic performance. Therefore, the paper forms a foundation from which solutions to CHD in the ward might be adopted and implemented to not only realise a healthy population but also translate the effort of this population to a viable state of economic productivity and, improve Leytonstone Ward’s overall economy.
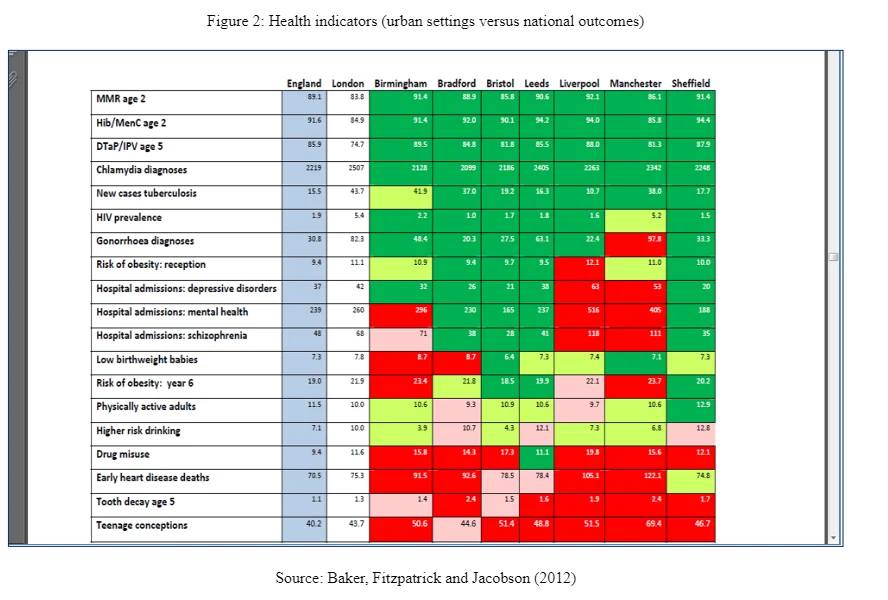
The importance of this examination is also informed by insights gained from the sick city hypothesis. According to the hypothesis, urban population health is poorer when compared to the rest of the national population (Townsend et al. 2012). With this trend, it becomes imperative to examine some of the major risk factors associated with conditions such as CHD in contexts such as Leytonstone Ward. The hypothesis states further that big cities tend to be environmentally less friendly, pedestrian less friendly, motor-vehicle dependent, and spatially vast or disconnected. On the other hand, small cities are documented to be more pedestrian-friendly, connected, compact, and less pollutant. According to the Department of Health (2012), these characterised posed by the sick city hypothesis reflect on the health statuses and outcomes of residents living in big and small cities. The following figure indicates a comparison of indicators in which urban-based settings tend to perform poorly when compared to the national average.
 Insights from the urban health penalty form an additional focal point from which this paper gains significance. As documented by the British Heart Foundation (2014), the urban health penalty states that residents in inner cities are likely to suffer chronic conditions to a similar extent as the experiences faced by people everywhere or in other parts of the country. However, situations facing these residents in the inner city tend to be worsened by adversities such as unemployment, poor housing conditions, poverty, and other socio-economic problems. As such, an understanding of the selected issue (which seeks to highlight the urban health profile of CHD among adults in Leytonstone Ward) is important because it will not only focus on trends in the selected health condition but also seek to understand the risk factors and related causes of CHD in this neighbourhood. The eventuality is that valid and reliable recommendations will be made for adoption and implementation to improve the overall state of health outcomes among residents. The following figure illustrates the assumptions held by the urban health penalty hypothesis.
Insights from the urban health penalty form an additional focal point from which this paper gains significance. As documented by the British Heart Foundation (2014), the urban health penalty states that residents in inner cities are likely to suffer chronic conditions to a similar extent as the experiences faced by people everywhere or in other parts of the country. However, situations facing these residents in the inner city tend to be worsened by adversities such as unemployment, poor housing conditions, poverty, and other socio-economic problems. As such, an understanding of the selected issue (which seeks to highlight the urban health profile of CHD among adults in Leytonstone Ward) is important because it will not only focus on trends in the selected health condition but also seek to understand the risk factors and related causes of CHD in this neighbourhood. The eventuality is that valid and reliable recommendations will be made for adoption and implementation to improve the overall state of health outcomes among residents. The following figure illustrates the assumptions held by the urban health penalty hypothesis.
Observation
CHD has been found to account for a significant rate of mortalities for individuals aged 75 and below. Compared to more affluent areas, poorer wards have been documented to experience significantly higher rates; including Leytonstone Ward. Recent statistics suggest that the death rates resulting from CHD in the ward lie at 0.5 percent in every 1,000 persons. Out of these people, males account for 0.6 percent of CHD-related deaths reported while the rate for women lies at 0.3 percent (Lim et al. 2013). Compared to the Waltham Forest average of 35.2 percent, individuals aged 20-39 are in a higher proportion in Leytonstone Ward. It is further notable that lower life expectancies for males and higher mortality rates for coronary and heart and circulatory diseases suggest that Leytonstone rates worse than the borough average (British Heart Foundation 2014).
A survey of this ward indicates that individuals exhibiting a high likelihood of visiting health care facilities include women aged 55 and above, individuals suffering from long-term conditions, and older people. On the other hand, groups such as younger adults, men, and persons in employment are less likely to visit health care facilities frequently (Department of Health, UK Food Standards Agency 2014). Notably, the gap between women and men has narrowed (in terms of life expectancy) while some of the factors contributing to CHD in the ward include diabetes, obesity, and high rates of smoking. A silent but significant challenge has also been observed in managing CHD and involves non-adherence to prescribed medicines. Similarly, about one third to a half of the prescriptions has not been taken as per the physicians’ recommendations (Department of Health 2012). In the wake of alcohol dependence, harmful drinking, and hazardous drinking, CHD remains the biggest killer in the ward and accounts for about 27 percent of premature deaths among adult populations. Similarly, the condition forms the major contributor to health inequalities between Leytonstone Ward and the rest of Waltham Forest, with about 29 percent and 34 percent life expectancy gaps reported for women and men respectively. Unhealthy eating and physical inactivity have also been found to contribute to the condition in Leytonstone Ward (British Heart Foundation 2014)
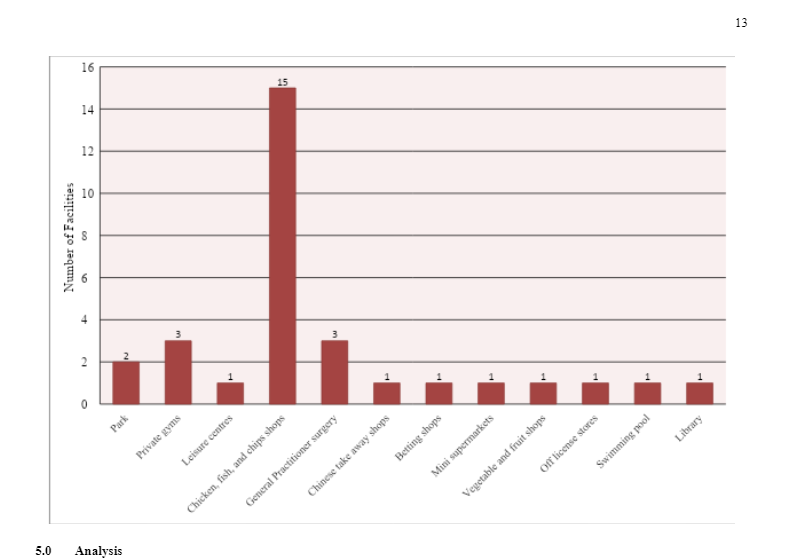
Primary data was collected through a five-hour direct observation. Indeed, the study extended to other neighbourhoods or surroundings to compare facility and service availability. Instruments for collecting data included note taking and the taking of photographs. The outcomes are summarised as follows:
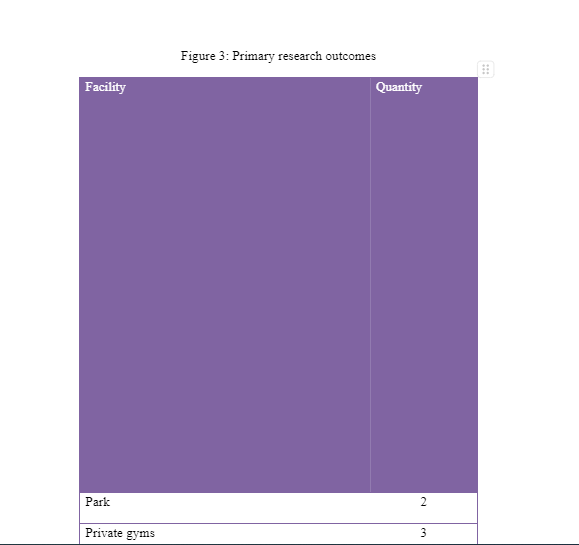
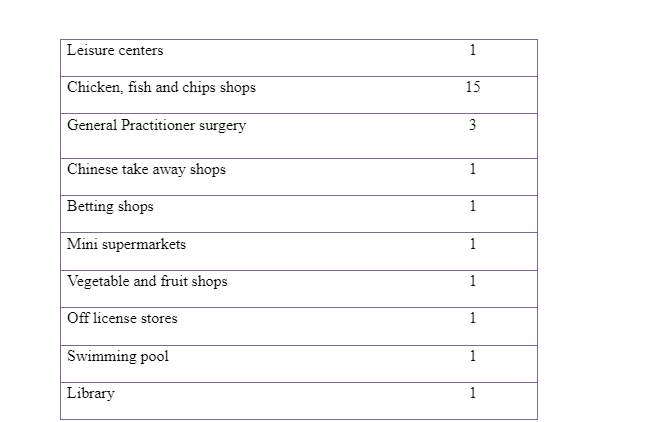
From the outcomes, there is a heavy presence of chicken, fish, and chips shops; foodstuffs that are perceived to be high in calories – complemented by a Chinese take away shop. Indeed, this trend is seen as a predictor of high risk for CHD. In addition, evidence of a sedentary lifestyle is seen due to the presence of fewer fitness facilities such as one swimming pool and only three private gyms. In addition, high risk for CHD is evidenced by the presence of only one vegetable and fruit shop; a trend that points to a potential challenge in healthy eating lifestyles – coupled with the presence of only one leisure centre. These outcomes are summarised in the figure below.
From the observations, prevalence of CHD in Leytonstone Ward can be attributed to lower rates of detection. In addition, the outcomes indicate that men remain at a higher risk, with similar outcomes reported in terms of death rates and related comorbidities. It is further notable that the causes of CHD in Leytonstone Ward seem to operate almost uniformly, and that no single cause stands out as the major contributor − such as a case in which obesity would outshine diabetes or physical inactivity as a major contributor of CHD. It is also worth highlighting that community sensitisation programmes are yet to receive an in-depth analysis, adoption, and application. Besides, physical exercising facilities remain underutilised and this trend translates into inactivity among most of the adult groups; including the groups diagnosed with CHD.
Conclusion and Recommendations

In summary, this paper has focused on CHD among adults in Leytonstone Ward. Findings indicate that men remain at risk more than women. Major risk factors in the region include smoking, alcohol consumption, diabetes, obesity, and physical inactivity. Similarly, lower rates of detection have been found to be major contributors not only to the escalation of the disease but also additional adversities such as emotional scars and trauma that the affected family members, friends, and relatives experience. From these outcomes, it is recommended that the public sector embraces community sensitisation programs in which adult groups would be sensitized about the inverse relationship between physical activity and risks for CHD. Similarly, physical exercising facilities should be developed further to foster access among members while health care organisations’ representatives should hold seminars and conferences. The aim of these seminars and conferences should be to highlight some of the health benefits that members of the public might experience, should they engage in healthy eating, screening for early detection and intervention, and regulate or cease smoking and drinking alcohol. Overall, a collaborative approach between the health sector and the public is projected to yield desirable outcomes and, in turn, make the improved health outcomes translate into better economic performance – due to the resultant presence of a healthy population in Leytonstone Ward.
Continue your exploration of COPD: A Worldwide Menace to Health with our related content.
List of References
- Baker L, Fitzpatrick J & Jacobson B, 2012, Capital Concerns: Comparing London’s health challenges with England’s largest cities. London Health Observatory
- British Heart Foundation 2014, Cardiovascular Disease Statistics 2014: British Heart Foundation Centre on Population Approaches for Non-Communicable Disease Prevention. Nuffield Department of Population Health, University of Oxford
- Department of Health, 2012, National Diet and Nutrition Survey – Assessment of dietary sodium levels in adults (aged 19 to 64 years) in England, 2011. London
- Department of Health, UK Food Standards Agency, 2014, National Diet and Nutrition Survey: headline results from Years 1, 2 and 3 combined (2008/9-2011/12). London
- HSCIC, 2013, Health Survey for England 2012, Trend tables. Health and Social Care Information Centre: London
- Lim SS et al., 2013, A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study. The Lancet, 380, 2224-2260
- Rodwin VG, 2001, Urban Health: Is the City Infected? In Medicine and Humanity. London: King's Fund. [Online] Available at: http://www.nyu.edu/projects/rodwin/main.html
- Townsend N et al., 2012, Coronary Heart Disease Statistics 2012 edition. British Heart Foundation Health Promotion Research Group and Department of Public Health, University of Oxford



- 24/7 Customer Support
- 100% Customer Satisfaction
- No Privacy Violation
- Quick Services
- Subject Experts