Quality and Diversity in Health and Social Care
Introduction
This report summarises the position of equality and diversity, especially the issues of discrimination and equal opportunities in the current health and social care regime. It reviews the current regime considering the six factors: age, disability, gender, ethnicity, sexuality, and class. For those seeking a deeper understanding or assistance, healthcare dissertation help can provide valuable insights and guidance on these critical issues.
The term, ‘equality’ carries a broad meaning. The introductory text of the Equality Act 2010 infers that the term has a social-economic consideration that does not provide any space for discrimination or harassment (as seen in its Section 4), associated with personal characteristics, such as age, disability, gender reassignment, marriage and civil partnership, pregnancy and maternity, race, religion or belief, sex, or sexual orientation.
The element of diversity impacts the consideration of the equality provisions in law or in social-economic policy. Diversity supports equality by promoting inclusion of people with personal characteristics. Section 4 of the Act of 2010 is the appropriate example. Diversity is another word for an inclusive approach towards achieving equality. This report will present the elements of equality and diversity as a way of delivering health and social care objectives.

Diversity and Equality in the health and social care system
The UK health and social care system considers the issues of equality and diversity in its policy and legislative measures. Each situation must be considered in its own right and thus a general principle cannot be applied. For instance, direct discrimination based on age is prohibited by Section 13 of the Act of 2010 except when the act is proportionate to achieve a legitimate means. Thus, it will not be discriminatory when the Department of Health invites women aged between 25 and 49 for a cervical screening every three years while inviting women aged between 50 and 64 every five years. This reason is the former group is more susceptible to the disease than the latter group. However, certain studies have highlighted the ongoing issue of age-based discrimination regarding tests and treatments, which for example limited coronary care facility to people above 65 years if age with suspected myocardial infarction. Such practices are in violation of the relevant legislations, such as the Health and Social Care Act 2012, which provides for equality in the social and health care system.
Continue your journey with our comprehensive guide to Primate Sexuality: A Comparative Study.
The Secretary of State has the duty to reduce inequalities in health services. This is particularly relevant as the situation of disabled people is not acknowledged in the policy practices. The 2021 report by the Disability Unit found that 78% of disabled people accessing health services experienced some difficulties while accessing public buildings. Even 83% of carers experienced the same difficulties. These two findings suggest indifference to people with disability in terms of accessing health care. It amounts to discrimination, as provided under Section 15 of the Act of 2010.
Disabled people require better access to care and healthcare services including funding and medical professionals with more knowledge about the needs of disabled people.

Human rights – equality and diversity
There are many courts’ judgments that enforce the rights of people with disability. For reference, in R (JF) v Merton LBC, the court held Merton LBC violated its duties regarding a needs assessment related to the claimant’s residential provision under the Care Act 2014. Disabled people are diverse group with different needs. Thus, there must be reasonable adjustments while taking policy decisions.
In regard to social and health care, access is linked with equal care and as such issues related to access become barriers to equitable care.

Gender recognition and protection
The equitable access must not vary in quality because of personal characteristics, including gender. For example, requiring Gender Reassignment Certificate for gender reassignment is unlawful discrimination, which is prohibited under Section 22 of the Gender Recognition Act 2004. Thus, the attitudes of general practitioners’ attitudes towards trans-patients will weaken the protection provided in the Gender Identity Services and will be in violation of the Act of 2010.

Indifference to different gender needs
The LGBT communities experienced inequalities with regard to health services and sexual health services. There is a lack of relevant quantitative data due to front-line services not collecting the information. This causes the neglect or lack of assessment of the needs of individuals as LGBT people, and inability to plan for their needs.
Continue your exploration of Challenges in Health and Social Care Management with our related content.
The issue of equitable access is also found with ethnic minority population despite the apparent strong commitment, including policy directives such as the NHS Ethnic Health Unit, 1996; dedicated teams and senior posts such as the Ethnic Health Advisor, 1989 or National Lead for Equality, 2013); and initiatives such the Equality Delivery System 2011 and 2013 with legislative reinforcement in the form of the Race Relations Act 1965 or the Equality Act 2010. Data collected related to ethnic monitoring in healthcare settings are limitedly used. This issues is similar to the issues concerning LGBT people where special attention is not given. Hence, the existing measures cannot address the low levels of trust in statutory services, low health literacy among minority ethnic people, and issues of access to primary healthcare. The following represents a health indicator:

The equality law provides protection against discriminatory or unequal treatment based on factors including one’s sexuality. There must be a legitimate reason for discrimination. For example, it is lawful when a sexual health service provider holds clinics at different times for women and men, it is justified as a combined service is not effective. Sexuality refers to a gender identity, body image or sexual desires and experiences. A person can, thus, have different needs relating to his sexuality irrespective of the age, personal history or mental capacity. Hence, a care provider must assess the needs to enable them to manage their sexuality. For example, best interest decisions cannot be made regarding their ability to consent to sex, as provided under the Mental Capacity Act 2005, S2. The aim is to promote an inclusive care based on equality, diversity and human rights. One such initiative is the Sexual Orientation Monitoring Information Standard to record sexual orientation of patients to deliver proper adult social care.
The access to better income and to be a part of a better social class also impact the equitable access to social and health care. The link between social class and health was identified almost 40 years ago. For instance, there is an inequality in life expectancy between men in social class 1 (example: managers and professionals) and those in social class 5 (example: unskilled workers). Low pay, unsafe jobs, low status and lack of power expose a low-class person to more health risks. Social class is, thus, linked to other protected characteristics identified by the Act of 2010 regarding access to health and care.
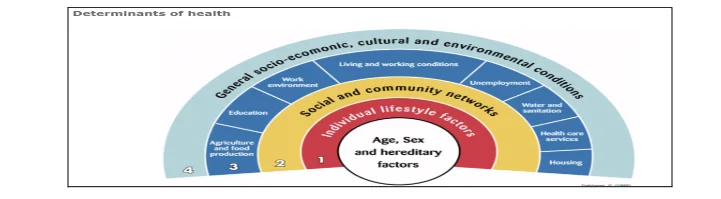
Health Determinants.
Health outcomes are generally worsened when there is greater socioeconomic disadvantage. For example, in 2013 it was found that males living in the most deprived region had a shorter life expectancy (8.2 years) than those living in the least deprived region.
The health and care regime seems to have a central focus on equitable access. However, inequity between socio-economic groups still exists. The lack of political will seems to still cause inequalities in the social and health care access system.
Conclusion
The impact of interpreting equality with a social-economic consideration impacts the area of employment, opportunity, family relationships, victimisation, and public and private function in relation discrimination and other prohibited conduct.
The current regime must consider the different protected characteristics and other social conditions while providing an adequate social and health care access.
Task 2
The Health and Social Care Act 2012 introduced the first legal duties governing health inequalities. The health bodies such as the Department of Health, Clinical Commissioning Groups, Public Health England, and the NHS England have specific duties with the aim to reduce health inequalities between the people. It also brought new functions of the local authorities.
This Act reinforces equality principles regarding physical and mental health. Irrespective of this Act, mental health issues have remained marginalised and stigmatised in the social services and in the society. In the sphere of social work practice, there are insufficient resources provided mental health services as those provided to other areas of health and care. Thus, people with serious mental health needs are more likely to live in poorer housing or in poorer physical health and may be unemployed or socially isolated.
The Act of 2012 has, however, brought changes to the Health and Social Care Act 2008. It ensures the practitioners protect and promote equality and diversity. One such duty is to provide integrated care services, as found under Section 195. Provisions such as Section 26 governing duties of Clinical commissioning groups provide for reducing inequalities regarding access, outcomes; promoting patients’ involvement in care decisions; and enabling patients to make choices.
The Act of 2012 has provided a consolidated patient-oriented approach, especially concerning patients with mental health conditions. duty under the HSCA 2012 explicitly recognises the need to consider treatment and care outcomes and the patient experience. CCGs are also required to endorse a patient-centred approach. It has also introduced competition principles (Chapter 2) concerning procurement, patient choices and competition and to safeguard patients’ interests in the form of free choices. This will ensure efficiency in health care services and adequate protection of patients.
The effectiveness of a legislation is also dependent on the policy measures. For example, the Act of 2012 imposes duties on the relevant authorities to reduce inequalities in access to health services. However, its effectiveness is subject to the concerned authority to implement an effective policy. Thus, this policy will lay down the course of action with the aim to achieve the goals of the legislation.
The Equality and Diversity Policy of the Windsor Forest Colleges Group is one such policy that aims to promote equality and diversity as envisaged in the Equality Act 2010. The students from over 100 nations, with different age groups is an evidence to its commitment to observing equality. It runs a Single Equality Scheme with the aim to commit. To an environment without discrimination, which is not merely legal compliance but a compliance to a social cause.
The Policy not only recognises the protected characteristics of the Act of 2010 but does far more by placing socio-economic background on equal footing. The Public Sector Equality Duty of reporting is a good example to this objective. The Policy also ensures the institution practices equality in the administration of the institute. For example, it conducts a Gender Pay Gap Reporting under the Equality Act 2010 (Gender Pay Gap Information) Regulations 2017.

The environment in the Windsor Forest College Group is one of diversity and equality found in the diverse workforce, equal employment opportunities, fair access to recruitment and selection procedures, equal access to jobs and posting ads, protection of employees from harassment, equal training opportunities, and freedom of choices in regard to the dress, culture and religious needs. It has designated authority, such as the Governors or the Chief Executive and Group Principal and Senior Leadership Team to enforce these provisions. It has monitoring standards to that effect.
Take a deeper dive into Qualitative Descriptive Study with our additional resources.
Bibliography
Books
Allen R, S Carr, K Linde, and H Sewell, Social work for better mental health A strategic statement (Department of Health 2016).
Thompson N, Anti-Discriminatory Practice: Equality, Diversity and Social Justice (Macmillan Education UK 2012)
Journals
Elder ET, ‘Which Benchmarks for Age Discrimination in Acute Coronary Syndromes?’ (2005) 34 AGE & AGEING 4.
Glover-Thomas N, ‘The Health and Social Care Act 2012: The emergence of equal treatment for mental health care or another false dawn?’ (2013) 13(4) Med Law Int. 279–297.
Salway S, et al, ‘Obstacles to “race equality” in the English National Health Service: Insights from the healthcare commissioning arena’(2016) 152 Soc Sci Med 102–110.
Shaw AB, ‘In Defense of Ageism’ (1994) 20 J. MED. ETHICS 188, 188-89; Phoebe Weaver Williams, ‘Age Discrimination in the Delivery of Health Care Services to Our Elders’ (2009) 11(1) Marquette Elder's Advisor 3.
Szczepura A, ‘Access to health care for ethnic minority populations’ (200%) 81(953) Postgraduate Medical Journal 141-147; Alan Nelson, ‘Unequal treatment: confronting racial and ethnic disparities in health care’ (2002) 94(8) Journal Of The National Medical Association 666.
Reports
Care Quality Commission, ‘Relationships and sexuality in adult social care services: Guidance for CQC inspection staff and registered adult social care providers’ (2019) accessed 11 November 2021
Accessed 11 November 2021
House of Commons: Women and Equalities Committee, ‘Transgender Equality: First Report of Session 2015–16’ (2016) accessed 11 November 2021
House of Commons: Women and Equalities Committee, ‘Health and Social Care and LGBT Communities’ (2019) accessed 11 November 2021
Public Health England, ‘Local action on health inequalities Understanding and reducing ethnic inequalities in health’ (2018) accessed 11 November 2021
Websites
Equality and Human Rights Commission, ‘Your rights to equality from healthcare and social care services: Equality Act 2010: Guidance for service users’ (2018) accessed 11 November 2021
service providers and customers’ (2012) accessed 11 November 2021
NHS Greater Glasgow and Clyde ‘Equality, Diversity and Human Rights’ (2021) accessed 11 November 2021
NHS Greater Glasgow and Clyde, ‘Why social class matters to health’ accessed 11 November 2021 https://www.nhsggc.org.uk/your-health/equalities-in-health/meeting-the-requirements-of-equality-legislation/legislation-policy/social-class/why-social-class-matters-to-health/>
NHS Greater Glasgow and Clyde, ‘Social Class and other protected characteristics’ accessed 11 November 2021
NHS, ‘Key legislation’ accessed 11 November 2021
Psoinos M, Eleni Hatzidimitriadou, Christina Butler and Ravinder Barn, ‘Ethnic Monitoring in Healthcare Services in the UK as a mechanism to address Health Disparities: A Narrative Review’ (2011) accessed 11 November 2021



- 24/7 Customer Support
- 100% Customer Satisfaction
- No Privacy Violation
- Quick Services
- Subject Experts