Understanding Cardiopulmonary Diseases
Introduction
The cardiopulmonary diseases are referred to the range of disease which affects the lungs and heart of the individuals. During the diagnosis of the cardiopulmonary disease, effective knowledge regarding the structure and function of the cardiac and pulmonary region is required to understand the way the heart and lungs work normally. In this assignment, the different structural and functional aspects of the heart and lungs are to be discussed to understand the way different parts of the cardiac and pulmonary region work. Additionally, seeking healthcare dissertation help can provide valuable insights into these complex topics. Lastly, a cardiopulmonary disease is to be explained to inform the way it is affecting the lungs or heart of the individuals as well as the way it can be treated.
Task 1:
1.1 Labelled Diagram of a mammalian heart

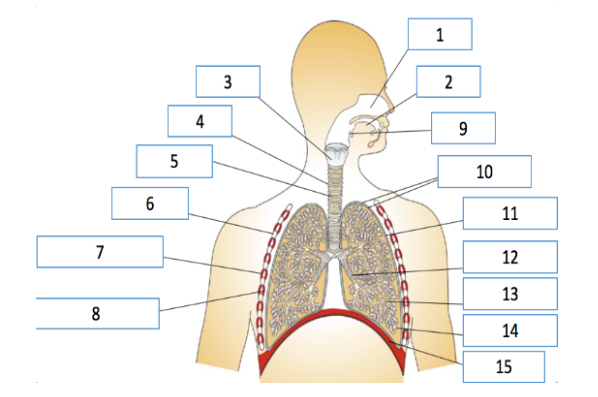
Labelled structure of the human heart

1 Pulmonary trunk
2 Superior vena cava
3 Pulmonary valve
4 Right atrium
5 Inferior vena cava
6 Tricuspid valve
7 Chordae tendineae
8 Right ventricle
9 Aorta
10 Left Atrium
11 Pulmonary vein
12 Bicuspid valve
13 Left ventricle
14 Myocardium
15 Septum
1.2 Question 2: A)
Stage (a)
Atrial systole
The stage is called atrial systole. The atrial systole mainly happens late after ventricular diastole in which the contraction of the right and left atria occurs as a result of decline in the ventricular pressure. The pressure is created through ventricular diastole in which the tricuspid and bicuspid valves open and lets the contents in the atria to flow into the empty ventricles. During the opening of tricuspid and bicuspid valve, the pulmonary and the aortic valves remain closed so that the pressure gradient present between the ventricle and the atrium is preserved during the late stage of ventricular diastole (Henein et al. 2018). At this stage, the arterial blood pressure is seen to reach 80-100mm Hg and the atrial systoles are indicated by P in the electrocardiogram (ECG) (Des Jardins, 2012).
Stage (b)
The stage is called ventricular systole. In ventricular systole, self-contraction is induced in such a way that pressure in left and the right ventricles increases to certain level which is more than the atrial chambers leading the tricuspid and bicuspid valves to be closed. The closing the valves are caused by inverted chordate tendinase along with the papillary muscles. This leads to build-up of pressure in the ventricle to rise to isovolumetric level which is maintained until the contraction phase is reached where the pressure is maximum. The pressure causes the aortic as well as pulmonary valves to be opened to let blood flow from the right and left ventricle. The phase is known as the ejection phase in which the blood flows from the high-pressure area in the ventricle to the low-pressure area in the aortic and pulmonary valve. The pulmonary trunk distributes blood to be left and right lungs whereas the aorta transport the blood to different parts of the body (Stokke et al. 2017).

Stage (c)
The stage is known as Ventricular filling. The ventricular filling occurs when the intraventricular pressure falls below the arterial pressure. In this condition, the blood from the left and right atrium flows through the opening of the atrioventricular valves (tricuspid and bicuspid valve). In this stage, despite the flow of blood into the atrium the intraventricular pressures are seen to develop continuously and fall briefly as the ventricles are filling with blood and are relaxing. Once the ventricles reach complete relaxation, the pressure is seen to slowly rise as they are filled with blood drawn from the atria. The ventricular filling is seen to be normally silent with third heart sound heard during rapid ventricular filling (Andersen et al. 2017).
Question 2b:
The heart works through the coordinated working of the ventricles and atria where they alternately contract and relax to pump blood through the heart. The electrical system of the heart us triggered through electrical impulses which travel from the sinoatrial node to the His-Purkinje network. The sinoatrial node is referred to the natural pacemaker of the heart where the electrical impulse is initiated within a small bundle of specialised cell known as the sinoatrial mode present in the right part of the atrium. The electrical impulse then flows through the walls of the atria which lead them to contract and this force the blood into the ventricles. The sinoatrial nodes set the rhythm of the heart (Moghtadaei et al. 2016).
The atrioventricular mode is referred to cluster of cells present in the middle of the heart between the ventricle and atria. This acts as the gate which lowers the flow of electrical impulse before it reaches the ventricles. This brief amount of delay in time allows the atria to contract and the ventricles to be relaxed. After this, the impulses are seen to the muscular walls of the ventricle through the His-Purkinje network causing the ventricles to contract. This contraction leads blood from the ventricle to be released into the body and lungs. The sinoatrial modes initiate another impulse and the cycle continues (van Setten et al. 2018; Vigmond and Stuyvers, 2016).
At microscopic level, the wave of depolarization in the heart is seen to propagate to the adjacent cells through gap junctions present on the intercalated disc. The heart is regarded as functional syncytium, where electrical impulses travel freely from one cell to another in free direction so that the proper function of the myocardium is ensured. However, the process though being advantageous under normal condition but it is detrimental in abnormal condition as it leads to incorrect propagation of electric signals in the heart (Kennedy et al. 2016).
1.3 Question 3:

1.4 Question 4:
The red blood cells are also known as erythrocytes and they are specialised cells which are circulated in the body to deliver oxygen to the tissues and organs. The red blood cells of the mammals are biconcave in structure as they lack mitochondria or nucleus. The size of the cells is 7-8µm. The red colour of the cell orients from the iron-containing protein known as haemoglobin. The key task of the protein is to carry oxygen to the body but it also helps to transport carbon dioxide (van Beers and van Wijk, 2019). The haemoglobin present in the red blood cells binds to four molecules of oxygen so that each of the cells is able to carry nearly 1 million molecules of oxygen. In humans, there are nearly 25 trillion red blood vessels present in the blood which is estimated to carry 25x1012 molecules of oxygen (van Beers and van Wijk, 2019). The red blood cells do not carry nucleus as a structural adaption to have space to contain more amount of haemoglobin so that carry increased amount of oxygen into the body. The lack of mitochondria is also effective for the red blood cells to avoid cellular respiration resulting the entire oxygen to be transported to other parts of the body rather than using them for own (Pivkin et al. 2016). In some mammals, there is the presence of nucleated red blood cells where they metabolise anaerobically by using metabolic pathway to form ATP and improve efficiency for transporting oxygen (Cluitmans et al. 2016).

Task 2:
Question 1:

Question 2:
a)
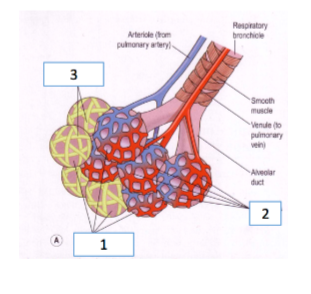
1. Alveoli
2. Capillary network around alveolus
3. Elastic fibres
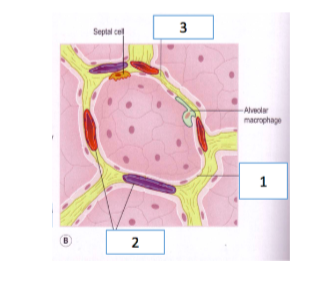
1. Squamous epithelial cell
2. Type II alveolar cells
3. Type I alveolar cells
b)
The alveoli are composed of two types of cells that type I and type II. The type I alveolar cells is seen to cover most of the surface and they function to act as an air-blood barrier. The air-blood barrier is required so that air bubbles do not enter the blood and then inside the alveoli. The barrier is preamble to allow oxygen, carbon dioxide, carbon monoxide and other gases to be transported (Vadász and Sznajder, 2017). This related to the function of the alveolus where they allow proper transport of gases from the body into and outside the lungs. The type II alveoli cells allow producing surfactant to coat the inside of the alveolus for reducing surface tension (Place et al. 2017). The Squamous epithelial cell in the alveoli ensures proper absorption and transport of gas is maintained by creating a barrier between internal body fluids and outside air (Tipping and Nicoll, 2018). This relates to the function of the alveolus where they allow gaseous exchange without coming in contact with the body fluids. According to Fick's law, pressure difference occurs between diffusion barriers and solubility of the gas is required for proper gaseous exchange (Pisano, 2017). The type I alveolar cells along with squamous epithelial cells are found to create proper condition to allow exchange of gases by avoiding formation of air bubbles and the type II cells are seen to create proper surface condition for diffusion of oxygen and carbon dioxide in the blood (Nardiello et al. 2017).
Question 3:
The ventilation occurs through inspiration and expiration. During rest and in normal condition, the contraction of the diaphragm occurs which makes it get flatted out and move downward nearly 10 cm with the ribs getting contracted and pulled upward. This enlarges the chest cavity and it is elongated allowing the air in the lungs to get expanded and filled to about 5mmHg below atmospheric pressure (Kovacs et al. 2017). At rest, the expiration occurs by making the air move out of the lungs and in this process the lung tissues are stretched along with sternum and the ribs come down and the diaphragm moves back to the original position in the thoracic cavity (Smith et al. 2017).
During exercise, the amount of oxygen transported to the blood becomes much lower than the amount of carbon dioxide expelled from the blood. Moreover, while executing the heavy exercise, the expiration becomes a major process compared to inspiration and more carbon dioxide is to be exhaled outside the body (Kovacs et al. 2017). In this condition, the intercostals muscles and abdominal muscles are seen to act more powerfully compared to ventilation during rest creating increased depth of exhalation. During exercise, the performance of the lungs is increased as breathing increased from 15 times a minute to 40-60 times in a minute (Aliverti, 2016). The tidal volume that is quantity of air inhaled and exhaled each breath is also increased as more amount of air is taken and released out due to the increase in the chest cavity caused by increased contraction and relaxation of the diaphragm and other abdominal muscles (Agostoni et al. 2017).
Question 4:
A)
The statement provided from 2-5 are true and thus the right option to be selected is d.
The cerebral cortex region provides assistance in voluntary breathing because within the region the motor cortex is present which is responsible to control voluntary breathing (Tan et al. 2016).
Respiration is mainly regulated through homeostatic and metabolic purposes in the brain. However, breathing rate is affected by emotions as change in emotions alters the homeostatic and metabolic functioning of the brain and body resulting the brain to increase or decrease respiration so as to regain homeostasis (Ma et al. 2017).
The chemical stimuli are able to alter rates of breathing because when there is increased carbon dioxide in the blood the individuals are to made more deeply as well as frequently so that the oxygen deficiency created is resolved and the increased carbon dioxide is released from the body to allow proper cellular respiration (Hopkins et al. 2017).
During exercise, abrupt increase exercise is followed by more gradual increase in breathing as with progress in exercise the body builds up more carbon dioxide which is to be realised thus leading the rate of respiration to be increased to draw in more oxygen and expel increased carbon dioxide to maintain homeostasis (Aliverti, 2016).
B)
The medulla oblongata is the primary centre of the brain which controls respiration. They have the key function to signal the muscles in the body to control respiration for allowing normal breathing. The ventral respiratory group in the brain control expiratory movements whereas the dorsal respiratory group in the medulla controls inspiration movements (Sheikhbahaei and Smith, 2017). During rest, the medulla oblongata sends signals to the muscles to inspire and expire normally so that normal tidal volume which is nearly 50ml per inspiration is maintained (Subhan and Ali, 2018). However, during exercise, the medulla oblongata perceives that there is increased need of oxygen in the body which leads it to direct increasing the tidal volume by increasing the relaxation and contraction of lungs and other abdominal muscles for respiration (Bordoni et al. 2018). The pons in the brain region controls the rate of respiration. The activation of apneustic centre in the pons leads to send signals in the body for taking long and deep breaths. This leads muscles to reach their maximum during inspiration increasing the tidal volume (Sheikhbahaei and Smith, 2017). However, the pnuemotaxic region in pons when activated inhibits the inspiration allowing fine control of respiration (Sheikhbahaei and Smith, 2017). The two centres work against one another for controlling increased and decreased rate of breathing during exercise and at rest to ensure proper homeostasis in the body is maintained by allowing balance in carbon dioxide and oxygen in the body.
Task 3:
Introduction
Pneumonia is referred to infection which inflames air sacs present in the right and left lungs. The organisms which affect individuals to develop pneumonia include virus, fungi, bacteria and others (Jain et al. 2015). In this presentation, an overview regarding the causes, risk factors, complications and symptoms related to cellular as well as physiological changes seen in pneumonia is to be discussed. The current treatment opportunity available for Pneumonia is also to be explained to aware individuals regarding the way to cope with the disease.
Rationale for choosing Pneumonia
Pneumonia is one of the common pulmonary diseases that affects many individuals in the UK as well as the world and is regarded as one of the key reason for deaths among the population (NICE, 2016). In 2012, as per the last published reports, nearly 28,952 deaths occurred in the UK due to pneumonia and it was 5.1% of all the deaths along with 25.3% of the deaths occurred in the country from pulmonary disease in the UK (NICE, 2016). This indicates many people in the UK die as a result of pneumonia and effective awareness regarding the disease is to be created by informing the causes, risk factors and treatment related to the disease so that people can be protected from major health condition and deaths as a result of the disease.
The current statistics revealed in 2016 informs that nearly 0.5-1% of adults in the UK are affected by community-acquired pneumonia. According to reports, 5-12% people who are diagnosed with lower respiratory infection presented before the GPs and 22-42% of them when admitted to the hospital show that they have mortality rate between 5-12% due to pneumonia. In the UK, more than half of the pneumonia-related deaths which occurs are seen among people who are above 84 years (statistics.blf.org.uk, 2019). This indicates that pneumonia is an essential health issue to be discussed so that by understanding the causes, effective intervention and treatment can be applied to lower the death and control better well-being of the individuals.
Causes of Pneumonia
The common cause of pneumonia is bacteria and viruses that are borne through the air and are inhaled by the individuals causing infection in the lungs. The Streptococcus pneumoniae is one of the common bacteria which are responsible for causing pneumonia. The S. pneumoniae may enter the body through cold or flu and is able to infect one part of the lungs leading to the condition known as lobar pneumonia (Silva-Costa et al. 2018). The Streptococcus pneumoniae is seen to release hydrogen peroxide in the lungs which damage DNA and leads to apoptosis in the lungs which leads the alveoli to get damaged. The damaged alveoli are unable to perform proper function to exchange gases in the lungs leading to the development of pus or phlegm making individuals show symptoms of pneumonia (Borges et al. 2017). The Mycoplasm pneumonia is another bacteria-like organism which causes milder symptoms of pneumonia (Izumikawa, 2016).
The fungi related diseases such as coccidioidomycosis is found to be one of the major causes of fungal pneumonia (Hagos and Esayas, 2015). The fungal pneumonia is common among individuals who have chronic health condition as their immune system which is key defence system of the body is weakened. This creates opportunity for the body to get easily affected by spores released in the air by fungi as the defence mechanism to control its impact is not properly maintained (Hagos and Esayas, 2015). The viruses which cause flu and cold are able to cause pneumonia. The viral pneumonia is mostly seen among children below the age of 5 years and though it is mild but in some cases, it may create fatal consequences (Shorr et al. 2017).
The hospital stay is one of the major causes of increased pneumonia among older individuals. This is because in the hospital the older people are contaminated by antibiotic-resistance bacteria and viruses from the droplets released by other patients through coughing and sneezing. This leads older people to become very sick. The people under ventilation in intensive care unit are prone to get affected by hospital-acquired pneumonia (Jun Li et al. 2017).
The health-acquired pneumonia is the bacterial infection which causes the disease among people who are in long-term care facilities and receiving care at the outpatients’ clinics such as kidney dialysis centres and others (Kumar et al. 2017).
Risk factors of Pneumonia
The treatment of the patients in hospital surroundings where proper hygiene is not maintained creates risk for people to develop pneumonia (Lazzerini et al. 2016). The presence of chronic diseases such as chronic obstructive pulmonary disorder or heart diseases creates risks for people to develop pneumonia. This is because in this condition the cells and tissues within the lungs that is responsible in managing the fluids and respiration are damaged leading the infection-causing agents to easily attack the respiratory system to make the patients develop pneumonia (Walters et al. 2017).
The people who smoke are prone to develop pneumonia because the harmful agents in the tobacco smoke damage the cells and tissues within the lungs making them weakened to fight against pathogens. Thus, the lack of proper defence from the body creates favourable environment for the growth of infection-causing bacteria and viruses to cause pneumonia among individuals (Hemilä, 2018).
The people with weakened immune system having HIV/AIDS, individuals who have undergone organ transplant or chemotherapy are at risk of developing pneumonia as their immune system is not working properly to protect their body from infection (Chien et al. 2015).
Symptoms of Pneumonia
The symptoms of pneumonia include:
Increased chest pain during breathing and coughing
Coughing produces pus or phlegm
Feeling of fatigue
Fever, shaking and chills
Low body temperature
Diarrhoea, nausea and vomiting
Shortness of breath (van der Maaden et al. 2016)
Physiological and cellular changes in Pneumonia
There is an intricate balance maintained between organisms which are residing in the lower part of the respiratory tract and at the local as well as at systematic defence mechanism. When this balance is disturbed, the inflammation of the lung parenchyma occurs leading to the development of pneumonia. In normal condition, it is seen that resident macrophages in the body act to protect the lungs from the impact of any foreign pathogen. However, the inflammation in the lungs is triggered by the pathogens leading to the clinical findings seen in pneumonia. During infection, the macrophage which is intended to protect the body engulfs the foreign pneumonia-causing pathogen and this triggers signalling or cytokinesis such as IL-8, TNF-α and IL-1 which recruits the inflammatory cells to the infection site. They are also seen to serve the antigens to the T cells which trigger both humoral and cellular defence mechanism creating activation of complement and form antibodies against the organisms. This leads towards the inflammation of the parenchyma of the lungs making the lining of capillaries leaky creating exudative congestion which underlines the pathogenesis of pneumonia (Dieu et al. 2017).
During pneumonia, the alveoli or the air sacs are inflamed creating spaces that are filled with pus and fluids. This change leads to coughing up of phlegm during pneumonia by the individuals and feeling of pain in the chest along with shortness of breath. This is because the alveoli cannot properly work to transport oxygen to the blood leading individuals to face lack of oxygen for respiration (Quinton and Mizgerd, 2015).
Diagnosis of Pneumonia
Pneumonia is initially suspected in individuals through physical examination executed by the general physicians. The presence of wheezing, cracking, decreased breathing with sounds is indicative the person may be suffering from pneumonia (Cilloniz et al. 2016). The Chest X-rays are done for confirming areas in the lungs being affected by pneumonia. A CT scan of the chest is done to get detailed description of the damage caused to the alveoli in the lungs as a result of pneumonia (Bourcier et al. 2016). The blood cell count is done to measure the number of white blood cells in the body. This is because white blood cells which are mainly involved in ensuring immunity to the body in lower amount indicates that the person is intensely affected by pneumonia and requires immediate action to control the impact of the disease to avoid further worsening of the individual’s health (Williams et al. 2015). A blood culture is done to identify the nature of organisms which has caused pneumonia so that proper antibiotics can be administered to help the patient cope with the disease (Davis et al. 2017). A bronchoscopy is executed for diagnosis of pneumonia and in this process, a thin and flexible tube that is fitted with a light is inserted into the lungs of the person affected by the disease. This is done to direct check the infected parts of the lungs and airways (Tomassetti et al. 2016).
Treatments of Pneumonia
The treatment and recovery of pneumonia include the following ways:
The individuals affected with the disease are provided aspirin to control their fever (lung.org, 2019)
The people with pneumonia are provided acetaminophen or non-steroidal anti-inflammatory drugs to control their chest pain and fever.
The antibiotic such as macrolide drugs is used as preferred treatment for pneumonia among children and adults. However, in recent conditions, it is seen that Mycoplasma pneumoniae have become resistant to the drug creating issues for the physicians to control pneumonia caused by the pathogen (Postma et al. 2015). The medications such as fluoroquinolones are found to widely used in the treatment of pneumonia among patients as it is found to be effective in resolving CAP caused by the H influenzae, H parainfluenzae, Klebsiella pneumoniae, M catarrhalis, C pneumoniae, Legionella pneumophila, S aureus, S pneumoniae and others. The medications are not fit to be provided to the children and to be used for adults only. In order to treat children, instead tetracycline drugs are to be used (Vardakas et al. 2017).

The individuals affected by pneumonia are to maintain proper hygiene so as to avoid spread of the disease. Moreover, the individuals are to take increased amount of water in thinning the sputum to loosen their chest (lung.org, 2019).
Prevention of Pneumonia
The two common vaccines used to prevent and control the risk of developing pneumonia are Prevnar or pneumococcal conjugate vaccine and Pneumovax or pneumococcal polysaccharide vaccine (Bonten et al. 2015). The Prevnar is usually provided as a routine immunisation for the child and it is recommended to be provided to people between 2-65 years and over. The Pneumovax is also recommended for both adults and children. Moreover, it is recommended to be administered to people above 65 years of age, diabetic people, people with lung, heart or kidney disorder, people with spleen disorder and individuals who smoke (Bonten et al. 2015). The vaccines do not offer entire protection to the patient but it reduces the risk of development of pneumonia.
Conclusion
Pneumonia is mainly caused by airborne pathogen and the organisms responsible for the disease include different types of bacteria, fungi and viruses.
The pneumonia symptoms include coughing sputum, tightness of chest, breathlessness and others.
The diagnosis of the disease is done through physical examination, CT scan, bronchoscopy and others.
The treatment available for pneumonia includes vaccination, antibiotics administration, intake of increased amount of water and others.
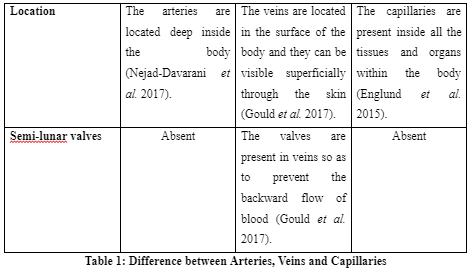
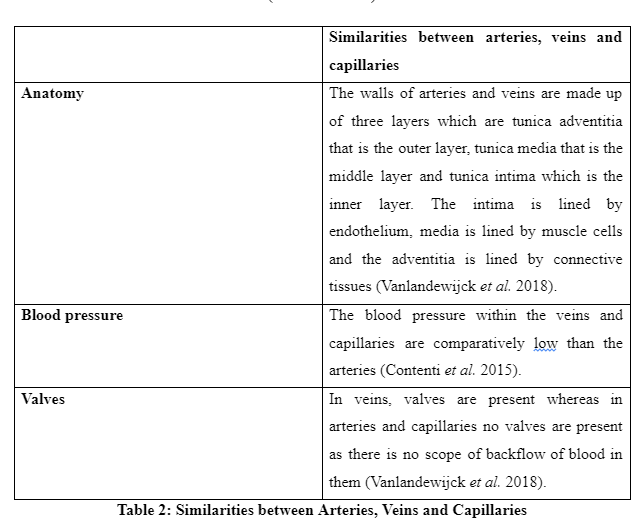
The above discussion informs that heart mainly works through three steps which are atrial systole, ventricular filling and ventricular systole. The heart works through coordinated working of the ventricles and atria where they alternately contract and relax to pump blood through the heart. The arteries are found to be involved in transporting oxygenated blood to the body whereas veins are involved in transporting deoxygenated blood and the capillaries involved in transporting blood to be tissues and cells. The different structures of the pulmonary region are pharynx, nasal passage, lungs, alveoli and others. One of the cardiopulmonary diseases widely affecting many individuals is pneumonia. The use of proper health measures along with antibiotics is able to assist people to control and prevent the disease.
Continue your exploration of Understanding Calcific Tendinopathy: with our related content.
References
Agostoni, P., Corra, U. and Emdin, M., 2017. Periodic breathing during incremental exercise. Annals of the American Thoracic Society, 14(Supplement 1), pp.S116-S122.
Aliverti, A., 2016. The respiratory muscles during exercise. Breathe, 12(2), pp.165-168.
Andersen, O.S., Smiseth, O.A., Dokainish, H., Abudiab, M.M., Schutt, R.C., Kumar, A., Sato, K., Harb, S., Gude, E., Remme, E.W. and Andreassen, A.K., 2017. Estimating left ventricular filling pressure by echocardiography. Journal of the American College of Cardiology, 69(15), pp.1937-1948.
Bonten, M.J., Huijts, S.M., Bolkenbaas, M., Webber, C., Patterson, S., Gault, S., van Werkhoven, C.H., van Deursen, A.M., Sanders, E.A., Verheij, T.J. and Patton, M., 2015. Polysaccharide conjugate vaccine against pneumococcal pneumonia in adults. New England Journal of Medicine, 372(12), pp.1114-1125.
Bordoni, B., Purgol, S., Bizzarri, A., Modica, M. and Morabito, B., 2018. The Influence of Breathing on the Central Nervous System. Cureus, 10(6).
Borges, I.C., Andrade, D.C., Cardoso, M.R.A., Meinke, A., Barral, A., Käyhty, H., Ruuskanen, O. and Nascimento-Carvalho, C.M., 2017. Seasonal patterns and association of meteorological factors with infection caused by Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis in childhood community-acquired pneumonia in a tropical region. Infectious Diseases, 49(2), pp.147-150.
Bourcier, J.E., Braga, S. and Garnier, D., 2016. Lung ultrasound will soon replace chest radiography in the diagnosis of acute community-acquired pneumonia. Current infectious disease reports, 18(12), p.43.
Casha, A.R., Camilleri, L., Manché, A., Gatt, R., Attard, D., Gauci, M., Camilleri‐Podesta, M.T. and Grima, J.N., 2015. External rib structure can be predicted using mathematical models: An anatomical study with application to understanding fractures and intercostal muscle function. Clinical Anatomy, 28(4), pp.512-519.
Chien, Y.F., Chen, C.Y., Hsu, C.L., Chen, K.Y. and Yu, C.J., 2015. Decreased serum level of lipoprotein cholesterol is a poor prognostic factor for patients with severe community-acquired pneumonia that required intensive care unit admission. Journal of critical care, 30(3), pp.506-510.
Cilloniz, C., Martin-Loeches, I., Garcia-Vidal, C., San Jose, A. and Torres, A., 2016. Microbial etiology of pneumonia: epidemiology, diagnosis and resistance patterns. International journal of molecular sciences, 17(12), p.2120.
Cluitmans, J.C., Gevi, F., Siciliano, A., Matte, A., Leal, J.K., De Franceschi, L., Zolla, L., Brock, R., Adjobo-Hermans, M.J. and Bosman, G.J., 2016. Red blood cell homeostasis: pharmacological interventions to explore biochemical, morphological and mechanical properties. Frontiers in molecular biosciences, 3, p.10.
Contenti, J., Corraze, H., Lemoël, F. and Levraut, J., 2015. Effectiveness of arterial, venous, and capillary blood lactate as a sepsis triage tool in ED patients. The American journal of emergency medicine, 33(2), pp.167-172.
Davis, T.R., Evans, H.R., Murtas, J., Weisman, A., Francis, J.L. and Khan, A., 2017. Utility of blood cultures in children admitted to hospital with community‐acquired pneumonia. Journal of paediatrics and child health, 53(3), pp.232-236.
Des Jardins, T., 2012. Cardiopulmonary Anatomy & Physiology: Essentials of Respiratory Care. Nelson Education.
Dieu, T.N.T., Nhat, A.P., Craig, T.J. and Duong-Quy, S., 2017. Clinical characteristics and cytokine changes in children with pneumonia requiring mechanical ventilation. The Journal of International Medical Research, 45(6), p.1805.
Diwakar, A., Adam, R.J., Michalski, A.S., Tamegnon, M.M., Fischer, A.J., Launspach, J.L., Horan, R.A., Kao, S.C., Chaloner, K., Meyerholz, D.K. and Stoltz, D.A., 2015. Sonographic evidence of abnormal tracheal cartilage ring structure in cystic fibrosis. The Laryngoscope, 125(10), pp.2398-2404.
Englund, E.K., Langham, M.C., Ratcliffe, S.J., Fanning, M.J., Wehrli, F.W., Mohler III, E.R. and Floyd, T.F., 2015. Multiparametric assessment of vascular function in peripheral artery disease: dynamic measurement of skeletal muscle perfusion, blood-oxygen-level dependent signal, and venous oxygen saturation. Circulation: Cardiovascular Imaging, 8(4), p.e002673.
Gould, I.G., Tsai, P., Kleinfeld, D. and Linninger, A., 2017. The capillary bed offers the largest hemodynamic resistance to the cortical blood supply. Journal of Cerebral Blood Flow & Metabolism, 37(1), pp.52-68.
Hagos, G. and Esayas, R., 2015. Pulmonary coccidiodomycosis presenting as a mass, an uncommon disease entity in Ethiopia. Ethiop. Med. J, 53(1), pp.35-7.
Hemilä, H., 2018. Effect of β-Carotene Supplementation on the Risk of Pneumonia Is Heterogeneous in Males: Effect Modification by Cigarette Smoking. Journal of nutritional science and vitaminology, 64(5), pp.374-378.
Henein, M.Y., Suhr, O.B., Arvidsson, S., Pilebro, B., Westermark, P., Hörnsten, R. and Lindqvist, P., 2018. Reduced left atrial myocardial deformation irrespective of cavity size: a potential cause for atrial arrhythmia in hereditary transthyretin amyloidosis. Amyloid, 25(1), pp.46-53.
Hopkins, S.R., Elliott, A.R., Prisk, G.K. and Darquenne, C., 2017. Ventilation heterogeneity measured by multiple breath inert gas testing is not affected by inspired oxygen concentration in healthy humans. Journal of Applied Physiology, 122(6), pp.1379-1387.
Izumikawa, K., 2016. Clinical features of severe or fatal Mycoplasma pneumoniae pneumonia. Frontiers in microbiology, 7, p.800.
Jain, S., Self, W.H., Wunderink, R.G., Fakhran, S., Balk, R., Bramley, A.M., Reed, C., Grijalva, C.G., Anderson, E.J., Courtney, D.M. and Chappell, J.D., 2015. Community-acquired pneumonia requiring hospitalization among US adults. New England Journal of Medicine, 373(5), pp.415-427.
jun Li, Y., zhi Pan, C., quan Fang, C., xiang Zhao, Z., ling Chen, H., hao Guo, P. and wen Zhao, Z., 2017. Pneumonia caused by extensive drug-resistant Acinetobacter baumannii among hospitalized patients: genetic relationships, risk factors and mortality. BMC infectious diseases, 17(1), p.371.
Kennedy, A., Finlay, D.D., Guldenring, D., Bond, R., Moran, K. and McLaughlin, J., 2016. The cardiac conduction system: generation and conduction of the cardiac impulse. Critical Care Nursing Clinics, 28(3), pp.269-279.
Kovacs, G., Herve, P., Barbera, J.A., Chaouat, A., Chemla, D., Condliffe, R., Garcia, G., Grünig, E., Howard, L., Humbert, M. and Lau, E., 2017. An official European Respiratory Society statement: pulmonary haemodynamics during exercise. European Respiratory Journal, 50(5), p.1700578.
Kumar, S.T., Yassin, A., Bhowmick, T. and Dixit, D., 2017. Recommendations from the 2016 guidelines for the management of adults with hospital-acquired or ventilator-associated pneumonia. Pharmacy and Therapeutics, 42(12), p.767.
Lazzerini, M., Seward, N., Lufesi, N., Banda, R., Sinyeka, S., Masache, G., Nambiar, B., Makwenda, C., Costello, A., McCollum, E.D. and Colbourn, T., 2016. Mortality and its risk factors in Malawian children admitted to hospital with clinical pneumonia, 2001–12: a retrospective observational study. The Lancet Global health, 4(1), pp.e57-e68.
Leder, S.B. and Neubauer, P.D., 2016. Embryology and anatomy of the oral cavity and pharynx. In The Yale Pharyngeal Residue Severity Rating Scale (pp. 13-32). Springer, Cham.
Light, R.W. and Lee, Y.G., 2016. Pleural embryology and gross structure, circulation, lymphatics, and nerves. In Textbook of Pleural Diseases (pp. 37-50). CRC Press.
Ma, X., Yue, Z.Q., Gong, Z.Q., Zhang, H., Duan, N.Y., Shi, Y.T., Wei, G.X. and Li, Y.F., 2017. The effect of diaphragmatic breathing on attention, negative affect and stress in healthy adults. Frontiers in psychology, 8, p.874.
Meilhac, S.M. and Buckingham, M.E., 2018. The deployment of cell lineages that form the mammalian heart. Nature Reviews Cardiology, 15(11), pp.705-724.
Moghtadaei, M., Jansen, H.J., Mackasey, M., Rafferty, S.A., Bogachev, O., Sapp, J.L., Howlett, S.E. and Rose, R.A., 2016. The impacts of age and frailty on heart rate and sinoatrial node function. The Journal of physiology, 594(23), pp.7105-7126.
Nardiello, C., Mižíková, I. and Morty, R.E., 2017. Looking ahead: where to next for animal models of bronchopulmonary dysplasia?. Cell and tissue research, 367(3), pp.457-468.
Nejad‐Davarani, S.P., Bagher‐Ebadian, H., Ewing, J.R., Noll, D.C., Mikkelsen, T., Chopp, M. and Jiang, Q., 2017. A parametric model of the brain vascular system for estimation of the arterial input function (AIF) at the tissue level. NMR in Biomedicine, 30(5), p.e3695.
Pearson Jr, W.G., Taylor, B.K., Blair, J. and Martin‐Harris, B., 2016. Computational analysis of swallowing mechanics underlying impaired epiglottic inversion. The Laryngoscope, 126(8), pp.1854-1858.
Pisano, A., 2017. Air Bubbles in the Blood Sample: Better or Worse Oxygenation? Dalton’s Law and Fick’s Law. In Physics for Anesthesiologists (pp. 19-26). Springer, Cham.
Pivkin, I.V., Peng, Z., Karniadakis, G.E., Buffet, P.A., Dao, M. and Suresh, S., 2016. Biomechanics of red blood cells in human spleen and consequences for physiology and disease. Proceedings of the National Academy of Sciences, 113(28), pp.7804-7809.
Place, T.L., Domann, F.E. and Case, A.J., 2017. Limitations of oxygen delivery to cells in culture: An underappreciated problem in basic and translational research. Free Radical Biology and Medicine, 113, pp.311-322.
Postma, D.F., Van Werkhoven, C.H., Van Elden, L.J., Thijsen, S.F., Hoepelman, A.I., Kluytmans, J.A., Boersma, W.G., Compaijen, C.J., Van Der Wall, E., Prins, J.M. and Oosterheert, J.J., 2015. Antibiotic treatment strategies for community-acquired pneumonia in adults. New England Journal of Medicine, 372(14), pp.1312-1323.
Quinton, L.J. and Mizgerd, J.P., 2015. Dynamics of lung defense in pneumonia: resistance, resilience, and remodeling. Annual review of physiology, 77, pp.407-430.
Quirk, J.D., Sukstanskii, A.L., Woods, J.C., Lutey, B.A., Conradi, M.S., Gierada, D.S., Yusen, R.D., Castro, M. and Yablonskiy, D.A., 2015. Experimental evidence of age-related adaptive changes in human acinar airways. Journal of Applied Physiology, 120(2), pp.159-165.
Safshekan, F., Tafazzoli-Shadpour, M., Abdouss, M. and Shadmehr, M.B., 2017. Viscoelastic properties of human tracheal tissues. Journal of biomechanical engineering, 139(1), p.011007.
Servais, A.B., Kienzle, A., Ysasi, A.B., Valenzuela, C.D., Wagner, W.L., Tsuda, A., Ackermann, M. and Mentzer, S.J., 2019. Structural heteropolysaccharides as air‐tight sealants of the human pleura. Journal of Biomedical Materials Research Part B: Applied Biomaterials, 107(3), pp.799-806.
Sheikhbahaei, S. and Smith, J.C., 2017. Breathing to inspire and arouse. Science, 355(6332), pp.1370-1371.
Shorr, A.F., Zilberberg, M.D., Micek, S.T. and Kollef, M.H., 2017. Viruses are prevalent in non-ventilated hospital-acquired pneumonia. Respiratory medicine, 122, pp.76-80.
Silva-Costa, C., Brito, M.J., Pinho, M.D., Friães, A., Aguiar, S.I., Ramirez, M., Melo-Cristino, J. and Portuguese Group for the Study of Streptococcal Infections, 2018. Pediatric complicated pneumonia caused by Streptococcus pneumoniae serotype 3 in 13-valent pneumococcal conjugate vaccinees, Portugal, 2010–2015. Emerging infectious diseases, 24(7), p.1307.
Smith, J.R., Hageman, K.S., Harms, C.A., Poole, D.C. and Musch, T.I., 2017. Effect of chronic heart failure in older rats on respiratory muscle and hindlimb blood flow during submaximal exercise. Respiratory physiology & neurobiology, 243, pp.20-26.
Stokke, T.M., Hasselberg, N.E., Smedsrud, M.K., Sarvari, S.I., Haugaa, K.H., Smiseth, O.A., Edvardsen, T. and Remme, E.W., 2017. Geometry as a confounder when assessing ventricular systolic function: comparison between ejection fraction and strain. Journal of the American College of Cardiology, 70(8), pp.942-954.
Subhan, F. and Ali, K., 2018. Control of Breathing. Essential Physiology for Dental Students, p.73.
Tabler, J.M., Rigney, M.M., Berman, G.J., Gopalakrishnan, S., Heude, E., Al-Lami, H.A., Yannakoudakis, B.Z., Fitch, R.D., Carter, C., Vokes, S. and Liu, K.J., 2017. Cilia-mediated Hedgehog signaling controls form and function in the mammalian larynx. Elife, 6, p.e19153.
Tan, C.H., Low, K.A., Schneider-Garces, N., Zimmerman, B., Fletcher, M.A., Maclin, E.L., Chiarelli, A.M., Gratton, G. and Fabiani, M., 2016. Optical measures of changes in cerebral vascular tone during voluntary breath holding and a Sternberg memory task. Biological psychology, 118, pp.184-194.
Tipping, R. and Nicoll, A., 2018. Mechanisms of hypoxaemia and the interpretation of arterial blood gases. Surgery (Oxford), 36(12), pp.675-681.
Tomassetti, S., Wells, A.U., Costabel, U., Cavazza, A., Colby, T.V., Rossi, G., Sverzellati, N., Carloni, A., Carretta, E., Buccioli, M. and Tantalocco, P., 2016. Bronchoscopic lung cryobiopsy increases diagnostic confidence in the multidisciplinary diagnosis of idiopathic pulmonary fibrosis. American journal of respiratory and critical care medicine, 193(7), pp.745-752.
Vadász, I. and Sznajder, J.I., 2017. Gas exchange disturbances regulate alveolar fluid clearance during acute lung injury. Frontiers in immunology, 8, p.757.
van Beers, E.J. and van Wijk, R., 2019. Red Blood Cell Biochemistry and Physiology. In Concise Guide to Hematology (pp. 15-20). Springer, Cham.
van der Maaden, T., de Vet, H.C., Achterberg, W.P., Boersma, F., Schols, J.M., Mehr, D.R., Galindo-Garre, F., Hertogh, C.M., Koopmans, R.T. and van der Steen, J.T., 2016. Improving comfort in people with dementia and pneumonia: a cluster randomized trial. BMC medicine, 14(1), p.116.
van Setten, J., Brody, J.A., Jamshidi, Y., Swenson, B.R., Butler, A.M., Campbell, H., Del Greco, F.M., Evans, D.S., Gibson, Q., Gudbjartsson, D.F. and Kerr, K.F., 2018. PR interval genome-wide association meta-analysis identifies 50 loci associated with atrial and atrioventricular electrical activity. Nature Communications, 9(1), pp.1-11.
Vanlandewijck, M., He, L., Mäe, M.A., Andrae, J., Ando, K., Del Gaudio, F., Nahar, K., Lebouvier, T., Laviña, B., Gouveia, L. and Sun, Y., 2018. A molecular atlas of cell types and zonation in the brain vasculature. Nature, 554(7693), p.475.
Vardakas, K.Z., Trigkidis, K.K. and Falagas, M.E., 2017. Fluoroquinolones or macrolides in combination with β-lactams in adult patients hospitalized with community acquired pneumonia: a systematic review and meta-analysis. Clinical Microbiology and Infection, 23(4), pp.234-241.
Vigmond, E.J. and Stuyvers, B.D., 2016. Modeling our understanding of the His-Purkinje system. Progress in biophysics and molecular biology, 120(1-3), pp.179-188.
Walters, J.A., Tang, J.N.Q., Poole, P. and Wood‐Baker, R., 2017. Pneumococcal vaccines for preventing pneumonia in chronic obstructive pulmonary disease. Cochrane Database of Systematic Reviews, (1). pp.23-45.
Widdicombe, J.H. and Wine, J.J., 2015. Airway gland structure and function. Physiological reviews, 95(4), pp.1241-1319.
Williams, D.J., Hall, M., Auger, K.A., Tieder, J.S., Jerardi, K., Queen, M.A., Statile, A., Myers, A. and Shah, S.S., 2015. Association of white blood cell count and C-reactive protein with outcomes in children hospitalized with community-acquired pneumonia. The Pediatric infectious disease journal, 34(7), p.792.



- 24/7 Customer Support
- 100% Customer Satisfaction
- No Privacy Violation
- Quick Services
- Subject Experts