Ethnicity and Health: Intersecting Factors Shaping Treatment Outcomes
Being White (versus coming from an ethnic minority) was a positive predictor of successful treatment

Out of 23 white ethnic patients, 12 had unsuccessful treatment whereas 11 had successful treatment. On the other hand, out of 9 other minor ethnic group people, 6 had unsuccessful treatment while 3 had successful treatment. As per chi-square test, χ2(1) = 0.552; p = 0.368. As the p–value or significant value is more than the critical alpha value of 0.05, it means there is no statistically significant interaction between ethnic group and treatment result. That is, being white (versus coming from an ethnic minority) was not a positive predictor of successful treatment. For those seeking further analysis and insights, consulting healthcare dissertation help can provide valuable assistance in interpreting such data.


As per Cox & Snell R Square and Nagelkerkr R Square, with 100% variation in the independent variable, that is, ethnic group, 1.7% to 2.3% variation can be expected in the dependent variable, that is successful treatment.


Further, the beta coefficient of independent variable is positively associated with dependent variable. However, p>0.05 for ethnicity shows it is not a statistically significant predictor of successful treatment.
Logistic regression analysis examined Being White predicts the successful treatment positively, defined as a thresh-old of 50%. Using this threshold, 11 white participants had successful treatment less than 50% of offered groups, whereas 3 minority participants had successful treatment, 50% or less of groups offered. This analysis revealed a non-significant prediction model (χ2(1) = 0.552; p = 0.368; Nagelkerke R2=.023) that predicted 81% of cases.
Ethnicity significantly predicts negative outcome

As per Cox & Snell R Square and Nagelkerkr R Square, with 100% variation in the independent variable, that is, ethnic group, 38.6% to 52.5% variation can be expected in the dependent variable, that is unsuccessful treatment.

Further, the beta coefficient of ethnicity is positively associated with dependent variable. However, p>0.05 for ethnicity shows it is not a statistically significant predictor of unsuccessful treatment.
Dig deeper into Evaluating the Treatment Landscape for Depression with our selection of articles.
Logistic regression analysis examined ethnicity significantly predicts the negative outcome, defined as a thresh-old of 50%. Using this threshold, 5 participants had unsuccessful treatment more than 50% of offered groups, whereas 1 participant had unsuccessful treatment, 50% or less of groups offered. This analysis revealed a non-significant prediction model (χ2(13) = 10.234; p = 0.675; Nagelkerke R2=.525) that predicted 81% of cases.
Those who were relatively older are more likely to complete treatment.
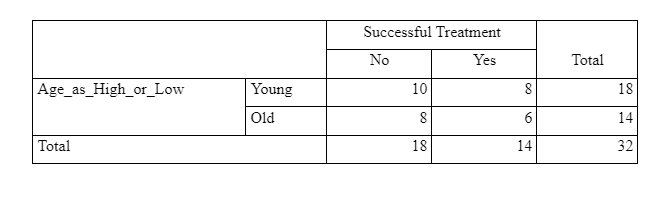
Out of 14 old patients, 8 had unsuccessful treatment, whereas 6 had successful treatment. On the other hand, out of 18 young patients, 10 had unsuccessful treatment whereas 8 had a successful treatment

As per chi-square test, χ2(1) = 0.008; p = 0.607. It means there is no statistically significant interaction between age group and treatment result (p>0.05). That is, those who were relatively older are not more likely to complete treatment.

There will be a significant difference in intelligence between the positive and negative reason for discharge.

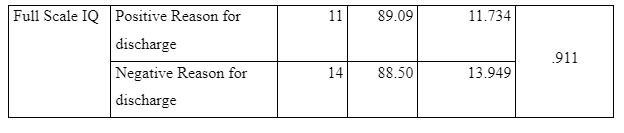
The mean full-scale IQ for the positive reason for discharge patients was 89.09 (SD = 11.734), and that of the negative reason for discharge was 88.50 (SD = 13.949). This shows that mean full-scale IQ was higher for the positive reason for discharge patients. Further, as per independent t-test, t(23) = 0.113; p = .911. Thus, there is no statistically significant difference in mean full-scale IQ between the positive reason for discharge and negative reason for discharge patients (p>0.05). Thus, there will not be a significant difference in intelligence between the positive and negative reason for discharge.
Negative reason for discharged patients will score significantly higher on the HCR-20 sum score (compare the means and SD between negatively discharged patients vs positively discharged patients; also, maybe see the difference between Historical score and Clinical and Risk Factor)
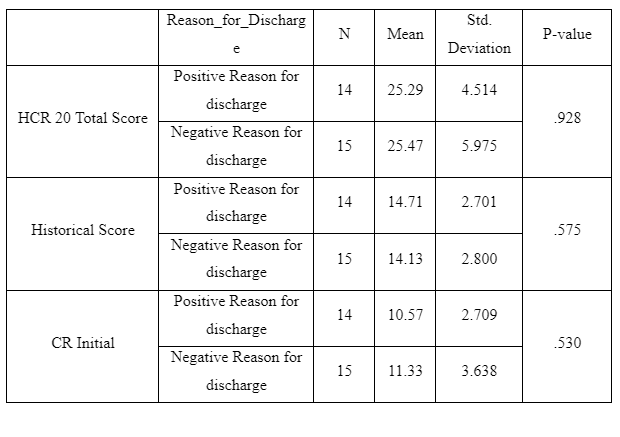
The mean HCR 20 Score, Historical Score and CR Initial for positive reason for discharge patients was 25.29 (SD = 4.51), 14.71 (SD = 2.70) and 10.57 (SD = 2.70) respectively, and that of negative reason for discharge was 25.47 (SD = 5.97), 14.13 (SD = 2.80) and 11.33 (SD = 3.63) respectively. Further, as per independent t-test for HCR 20 Score, t(27) = -0.092; p = .925. Thus, it can be said that there is no statistically significant difference in mean HCR 20 Score between the positive reason for discharge and negative reason for discharge patients (p>0.05).
As per independent t-test for Historical Score, t(27) = 0.568; p = .581. Thus, there is no statistically significant difference in mean Historical Score between the positive reason for discharge and negative reason for discharge patients (p>0.05).
As per independent t-test for CR initial, t(27) = -0.636; p = .530. Thus, there is no statistically significant difference in mean CR Initial between the positive reason for discharge and negative reason for discharge patients (p>0.05).
Thus, overall, it can be said that negative reason for discharged patients will not score significantly higher on the HCR-20 sum score, Historical score and CR initial as compared to positively discharged patients.
Negative reason for discharged patients will score significantly higher on the PCL-R (cut-off of 25).

The mean PCL-R score for negative reason for discharge patients was 21.14 (SD = 6.503).
Further, as per one-sample t-test, t(13) = -2.219, p = 0.045. Thus, mean psychopathy scale score for the negative reason for discharge patients was statistically significantly different from 25 (p<0.05). That is, the negative reason for discharged patients will score significantly lower than 25 on the PCL-R
Anti-social and borderline personality disorders will negatively associate with positive discharge in comparison to other personality disorders (9 in total).
In the present case, different personality disorders are independent variables and positive discharge is dependent variable.

With 100% changes in the independent variables, a variation between 22.2% and 29.7 can be expected in the dependent variable.

The above table shows that apart from schizoid personality disorder, all the other personality disorders are positively associated with positive discharge.
Longer length of admission will significantly be associated with treatment outcome.

The mean stay for positive reason for discharge was 46.93 months whereas that of negative reason was 36.06 months with p>0.05 showing no significant difference in number of months admissioned between positive reason and negative reason for discharge. Thus, longer length does not significantly associated with treatment outcome.
DISCUSSION
In recent some years, an increase in discrimination in patients on the basis of their ethnicity has been observed. It has become a major issue in the health care sector and has a significant negative impact on the performance of the sector, as well as on efficiency and effectiveness of the industry. In this regard, Greer (2010) had observed a significant amount of disparities in diagnosis and treatment provided to patients on the basis of their race and ethnicity. They found that treatment given to ‘White’ people was far more effective and in accordance with their disease or illness as compared to individuals from other ethnic groups and minorities. Their study revealed that being a white person was actually beneficial to the patients in comparison to other ethnic minorities. This means that if a person was white, then their treatment would be far more effective and helpful in resolving their health issue. However, the results of the current study contradict the findings of Greer (2010). During the current study, it was determined that being white versus other ethnic minorities was not a positive predictor of successful outcomes. No statistically significant interaction was observed between ethnic groups and treatment results. On the basis of results of the current study, it can be said that being from the white community does not guarantee a positive outcome of treatment being provided to the patient.
Shavers, et al. (2012) and Chu, et al. (2016) in their respective studies, found that older people most of the times, complete their treatment. This means that older people are more likely to complete their treatment than individuals from the younger generation. Shavers, et al. (2012) stated in their research that older people exhibit better levels of calmness. This enables them to complete their treatment and thereby ensure that their health issue(s) are resolved to the greatest possible extent. According to the study by Shavers, et al. (2012), care professionals also tend to give more attention to older individuals because they think that these people are more in need for immediate and effective care. On the other hand, young people can wait a little longer if it is not an emergency case. Results of the study by Chu, et al. (2016) supported the findings of Shavers, et al. (2012). During the current study, it was observed that the vast majority of the older people did not have successful treatment. Similarly, the majority of young people also did not have successful treatments. On the basis of these results, it can be said that the success of treatments differs from case to case scenario. Age of the patients does not have any role to play in this context. In the current study, the researcher found that there was no statistically significant interaction between age group and treatment results.
Results of this study support the findings of Weech-Maldonado et al. (2012) instead. Weech-Maldonado et al. (2012) had found that care professionals tend to give more attention to the situation and issues faced by the patients rather than their age. This enables them to provide effective and appropriate care services. According to Weech-Maldonado et al. (2012), there is a very minimal impact of demographic factors such as the age of the patients on the treatment that they receive. Care professionals treat cases on the basis of their merit, and therefore they do not give much attention to the age of the patients. If they come across a case that requires urgent medical attention, then they will take actions accordingly. In such situations, they will not consider the age of the patient(s). However, Wandner et al. (2014) stated in their study that patient demographics have a significant impact on treatment and pain management. Several past studies also have shown similar results, as the past researchers have stated that modern-day regulations and policies governing operations of the sector are so strict that the care professionals cannot discriminate patients on the basis of demographic factors such as age.
The current results show that there is no significant difference in intelligence between the positive and negative reasons for discharge. This result correlates with the results of Schenker et al. (2010) and Ali et al. (2013). These authors had successfully determined that there is no correlation between positive and negative results for discharge. According to Schenker et al. (2010), most of the patients who were considered for their study were discharged from the hospital or care home due to the positive outcome they received from the treatment. This means that patients were discharged because their health issue had been successfully resolved. In such situations, the care staff and hospital administration tend to discharge the patients and does not aim to keep the bed occupied. Such situations can reduce the overall profitability of their operations and can also hinder operations of the hospital as it would diminish the effectiveness of functioning of the hospital.
Similar to this, Ali et al. (2013) found that patients were discharged from the hospital because of the negative outcome of their treatment. This meant that the majority of the patients were discharged because they did not react to their treatment and were not getting any better. Therefore they were referred or transferred to another hospital that could have cared for their needs and provided them with a more comprehensive treatment. In the current study as well, it was observed that there is no significant difference in intelligence between positive and negative reasons for discharge from the hospital.
A key aspect for the current study was that the negative reasons for discharged patients scored higher on the HCR-20 sum score. This was a major assumption of this investigation. During the study, it was found that there is a difference in all the scores between positive and negative reasons for discharge. According to Kengne (2010) and Sabin & Anthony (2012), determining the reasons for discharge from the hospital helps in understanding the effectiveness and success of the treatment given to the patients. If they were discharged for positive reasons, then it would mean that treatment given to them was successful and helped them to recover from their illness. On the other hand, if they were discharged for negative reasons, then it would mean that the treatment was not successful and the patients were not successfully treated. Herein it was further observed that the HCR-20 sum score was a little higher for negative reasons for discharge than the positive reasons for discharge. The gap between these two was very minimal and therefore indicated that there were more negative reasons for discharge than the positive ones. On the basis of these results, it may be said that a large number of the patients did not receive proper treatment, due to which they were discharged for negative reasons.
While conducting an independent samples test to determine whether the difference between positive and negative reasons for discharge was statistically significant or not, it was observed that there is no statistically significant difference in mean HCR20 scores between positive and negative reasons for the discharge of the patients. This correlates with the findings of Hansen & Tore (2012) who also found similar results. This similarity shows that the patients were discharged for positive and negative reasons from the hospitals. Treatment of some of the patients was successful while for some, it was ineffective and thus unsuccessful.
During the study, it was further found that there is no statistically significant difference in mean historical scores between positive and negative reasons for the discharge of the patients. This contradicts with the results obtained by Cheng & Elizabeth (2015) who found that there is a significant difference in historical scores for positive and negative reasons for the discharge of the patients. In their study, Cheng & Elizabeth (2015) found that these differences indicate a significant lack of correlation between effectiveness and appropriateness of the treatments given to the patients. These need to be managed adequately so as to ensure that the needs and requirements of the patients are fulfilled to the greatest possible extent and also that they are satisfied with the treatment they are being given. On the basis of the current results, it can further be said that this lack of statistically significant relationship between the positive and negative reasons for the discharge of the patients.
The current also showed that it is no statistically significantly different in mean CR Initial between positive reasons for discharge and negative reasons for discharge patients. Herein it can be said that the lack of statistically significant differences in positive and negative reasons for patient discharge shows that patients are discharged only after they have been properly treated and when they are satisfied with the treatment and care services they received. Cook & Samuel (2014) and Earnshaw et al. (2015) obtained similar results. While Cook & Samuel (2014) noted that the means CR Initial score tend to indicate the effectiveness of the treatment, Earnshaw et al. (2015) observed similar scores showcase reliability of the healthcare services and their overall effectiveness.
On the basis of the results obtained in the current investigation, it can be said that the negative reasons for discharged patients will not score significantly higher on the HCR-20 sum score, historical score and CR Initial scores. However, on the other hand, positive reasons for discharged patients will score higher on the HCR-20 sum score, historical score and CR Initial score as well.

During the study, it was further found that since the psychopathy scale score for negative reasons for discharged patients will be lower than 25 on the PCL-R scores. Herein it was noted that the p-value was less than the critical alpha value of 0.05. This finding is opposite to the results of Richardson (2010). They found that negative reason for discharged patients was significantly higher on the PCL-R scores. However, the results of Blair (2014) were different. They stated that anti-social and borderline personality disorders negatively related to positive reasons for discharged patients in comparison to other personality disorders.
Numerous elements may add to the social insurance inconsistencies saw in these investigations. A few analysts recommend that there might be unobtrusive contrasts in the manner that individuals from various racial and ethnic gatherings react to treatment, especially concerning some pharmaceutical mediations, proposing that varieties in certain types of treatment might be advocated based on patient race or ethnicity (Kengne, 2010). Furthermore, patients shift in help-seeking conduct, and some racial and ethnic minorities might be almost certain than whites to maintain a strategic distance from or defer looking for care. Be that as it may, most of the studies discover differences in clinical administrations that are similarly powerful for all racial and ethnic gatherings. Further, the investigations that the IOM surveyed recommend that racial contrasts in patients' mentalities, for example, their inclinations for treatment, do not differ enormously and can not completely clarify racial and ethnic aberrations in social insurance. Few examinations, for instance, locate that African Americans are marginally bound to dismiss medicinal proposals for certain medications. However, these distinctions in refusal rates are commonly little (Weech-Maldonado et al., 2012). It stays misty why African-American patients are bound to dismiss treatment proposals. Is it accurate to say that they are rejecting treatment in light of a general question of human services suppliers? Or then again do some decay treatment as a result of negative encounters in the clinical experience or recognition that their primary care physician is not put resources into their consideration? More research is expected to completely comprehend treatment refusal on the grounds that the purposes behind refusal may prompt various procedures to assist patients with settling on educated treatment choices (Cheng & Elizabeth, 2015).
Any level of vulnerability a doctor may have comparative with the state of a patient can add to incongruities in treatment. Specialists must rely upon surmisings about seriousness dependent on what they can see about the sickness and on what else they see about the patient (e.g., race). The specialist can in this way be seen as working with earlier convictions about the probability of patients' conditions, "priors" that will be diverse as per age, sex, financial status, and race or ethnicity (Earnshaw et al., 2015). At the point when these priors are considered close by data assembled in clinical experience, both impact medicinal choices. Specialists must adjust new data picked up from the patient (in some cases with fluctuating degrees of precision) and their earlier assumptions regarding the patient to make a conclusion and decide a course of treatment. On the off chance that the doctor experiences issues precisely understanding the side effects or is more uncertain of the "signal" – the arrangement of pieces of information and signs that doctors depend upon to settle on analytic choices – at that point the person is probably going to put more noteworthy load on "priors” (Schenker, et al., 2010). The outcome is that treatment choices and patients' needs are conceivably less, very much coordinated.
Discrimination is just conflictingly identified with getting screenings for malignancy, hypertension, and diabetes. A couple of critical connections discovered varied both by the proportion of segregation and the respondents' race and ethnicity (Hansen & Tore, 2012). Given the developing decent variety in the United States and the pervasiveness of separation, more research with respect to its effect on human services usage is required. Just when every one of the components impacting persistent practices is better, comprehended will arrangements and intercessions intended to improve them be fruitful. ) discovered Depressive indications and MDD were most basic in Turks and South-Asian Surinamese, and least in ethnic Dutch. PED had a positive relationship with burdensome side effects and MDD in just the ethnic minority gatherings (Greer, 2010). The commitments of PED to burdensome manifestations and MDD were around 25% in both the Surinamese gatherings, and Turks, and ∼15% in Ghanaians.
REFERENCES
Greer, T., 2010. Perceived racial discrimination in clinical encounters among African American hypertensive patients. Journal of Health Care for the Poor and Underserved , 21(1), pp. 251-263.
Shavers, V., Pebbles, F. & Dionne, J., 2012. The state of research on racial/ethnic discrimination in the receipt of health care. American Journal of Public Health , 105(2), pp. 953-966.
Chu, J., Leino, A. & Samantha, P., 2016. A model for the theoretical basis of cultural competency to guide psychotherapy. Professional Psychology: Research and Practice, 47(1), p. 18.
Weech-Maldonado, R., Allyson, H. & Thomas , B., 2012. The relationship between perceived discrimination and patient experiences with health care. Medical care, 20(902), p. S62.
Wandner, L., Heft, M. & Lok, B., 2014. THE IMPACT OF PATIENTS’ GENDER, RACE, AND AGE ON HEALTH CARE PROFESSIONALS’ PAIN MANAGEMENT DECISIONS: AN ONLINE SURVEY USING VIRTUAL HUMAN TECHNOLOGY. International Journal of Nursing Studies, 51(5), pp. 726-733.
Schenker, Y., Andrew, K. & Dean, S., 2010. The impact of limited English proficiency and physician language concordance on reports of clinical interactions among patients with diabetes: the DISTANCE study. Patient education and counseling, 81(2), pp. 222-228.
Ali, A., Katrina, S. & Victoria, R., 2013. Discrimination and other barriers to accessing health care: perspectives of patients with mild and moderate intellectual disability and their carers. PloS one, 8(8), p. e70855.
Kengne, A.-P., 2010. The Framingham and UK Prospective Diabetes Study (UKPDS) risk equations do not reliably estimate the probability of cardiovascular events in a large ethnically diverse sample of patients with diabetes: the Action in Diabetes and Vascular Disease: Preterax. Diabetologia, 53(5), pp. 821-831.
Sabin, J. & Anthony, G., 2012. The influence of implicit bias on treatment recommendations for 4 common pediatric conditions: pain, urinary tract infection, attention deficit hyperactivity disorder, and asthma. American journal of public health, 102(5), pp. 988-995.
Hansen, K. & Tore, S., 2012. Ethnic discrimination and psychological distress: a study of Sami and non-Sami populations in Norway. Transcultural psychiatry, 49(1), pp. 26-50.
Cheng, T. & Elizabeth, G., 2015. Race, ethnicity, and socioeconomic status in research on child health. Pediatrics, 135(1), pp. e225-e237.
Cook, B. & Samuel, Z., 2014. Assessing racial/ethnic disparities in treatment across episodes of mental health care. Health services research, 49(1), pp. 206-229.
Earnshaw, V., Laura, B. & John, D., 2015. Stigma and racial/ethnic HIV disparities: moving toward resilience. Health services research, p. 60.
Richardson, L., 2010. Access to health and health care: how race and ethnicity matter. Mount Sinai Journal of Medicine: A Journal of Translational and Personalized Medicine: A Journal of Translational and Personalized Medicine, 77(2), pp. 166-177.
Blair, I., 2014. An investigation of associations between clinicians’ ethnic or racial bias and hypertension treatment, medication adherence and blood pressure control. Journal of general internal medicine, 29(7), pp. 987-995.
Continue your journey with our comprehensive guide to Doping and Character in Triathletes.



- 24/7 Customer Support
- 100% Customer Satisfaction
- No Privacy Violation
- Quick Services
- Subject Experts