Parent-Child Interaction Therapy
Introduction:
The interaction between children and parents is critical and fundamental for language development (Allen & Marshall, 2010). Therefore, speech language therapists emphasize the importance of assessing and modifying the interaction patterns between child and his parent (Falkus et al., 2015). The intervention approach which is focused on modifying the interaction between children and parents become commonly used by clinicians that is called “parent – child interaction therapy” as an alternative approach for managing children’s language delay (Kelman & Schneider, 1994). Moreover, there is reciprocal relationship between language skills and interaction patterns which means that language delay may affect the parent- child interaction consequently the poor interaction affects language skills (Kelman & Schneider, 1994). One of the concept behind this approach, is generalization of the acquired skills in the real life and not restricted only in clinical settings, this generalization will occur if parents carry out acquired skill into daily life (Falkus et al., 2015). This approach besides involving parents in delivering the therapy, the interaction between child and his parents is recorded, then parent and SLT analyze the patterns and set the targeted patterns to be modified, then parents are asked to report any changes in child’s communication and to report the most effective strategies that being used in the intervention (Falkus et al., 2015). For those pursuing advanced studies in this field, seeking psychology dissertation help can provide valuable insights into such methodologies.
The PCIT approach is widely used in clinics by SLTs and proved to be beneficial, nevertheless, there is limited evidence in literature about its effectiveness. There is one study which investigated this intervention approach among preschool children with language delay and reported its effectiveness for language and communication skills, however, this study used within design and did not include a control group (Falkus et al., 2015). A second study which targeted school age children with specific language impairment and include delayed intervention group to be a control group, and revealed its effectiveness clinically and costly (Allen & Marshall, 2010). Most of previous studies explored the effect of this approach on the improvement of child parent interaction, but its benefit to language skills has not received enough attention. Additionally, the effect of this approach on language skills compared with regular focused language intervention has not been investigated yet. Therefore, this study will investigate the direct effect of PCIT approach to the improvement of language skills and the difference between PCIT and regular stimulated approach will be explored.
Aims:
1. Are the delayed language affect interaction patterns and is the poor interaction affects language development? Is there a relationship between child’s language skill and parent child interaction?

2. is there a difference between language skill before and after PCIT intervention?
3. Are the interaction patterns will improve after regular therapy of language skills?
4. What is the difference between 2 approaches in development of language skills among children with language delay?
5. Is the improvement of language skill among all participants due to different intervention approaches or due to age?
6. Are the modified interaction patterns will persist for long term period with PCIT group?
Method:
Participants:
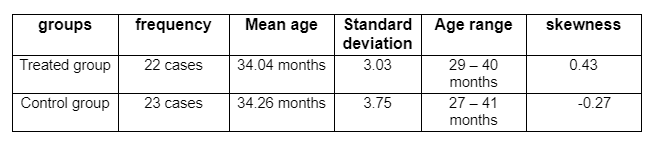
45 children who have been diagnosed with language delay were included with their parents in this study. The age range of participants is from 27 to 41 months (mean age = 34 months, SD= 3.38 months), and 24 of them were females and 21 were males. Children who had language delay secondary of other disability like hearing loss or who had additional disabilities besides language delay were excluded.
Design:
The 45 children with their parents were randomly assigned into two groups, the first group received the PCIT approach (treated group), and the second group received the regular language therapy approach (control group). The study design used is randomized control trail, that two groups involved in the study one of them used the new intervention and the second one used the regular therapy and it was a longitudinal study that carried out over 6 weeks.
Procedure:
The language skills of the two groups were assessed on three time points (pre therapy – post therapy – follow up) by using PLS4 (preschool language scale, 4th edition) and parent rating scale was used to assess the child parent interaction patterns on the three time points. A video was recorded of parent child interaction at the beginning of the study for both groups, then parents and therapists watched and analyse the interaction patterns used and parents rated their performance in the parent rating scale. For treated group, a video was recorded at the beginning of each session then parents and SLT discussed the good and poor patterns used by parents in the interaction, and an advice by SLT of how to practice the targeted patterns at home was given after watching and rating the video. On the other hand, with the control group only three videos were taken (pre therapy – post therapy – follow up), then parents and therapists analysed and discussed the positive and negative patterns, then advices by therapist were given to improve these patterns. Additionally, for the treated group, no direct therapy for language skills were delivered. However, for the control group, individualized therapy plan for each child’s language skill was performed by SLT and direct therapy was delivered once weekly over 6 weeks.
Data collected:
The data was collected from using PLS4 which measures language skills over 3 time points: before therapy (time 1 scores), 6 weeks after therapy (time 2 scores), and at follow up (time 3 scores), it is a continuous data. Additionally, parent rating scale which is a self rating scale completed by the parents to assess their performance when interacting with their children. The parent rating scale consists of 10 verbal and non verbal interaction patterns (allow the child to choose toys - follow what the child wants to do - paly down at child’s level - wait for child to start the talking with words, gestures, sounds or eye contact - give him/her extra time to talk - show that I am listening by repeating or answering him/her- comment on what the child is doing, seeing or hearing – not asking questions – give verbal praise – talking slowly so your child can understand) this scale is using 4 points Likert scale ( 0= never, 1= sometimes, 2= often, 3= always) these points collected to indicate the parent’s performance level during interaction with their child. The parent rating scale is ranging from 0 – 30, where zero indicates the poorest parent child interaction and 30 indicates normal parent child interaction. The self rating scale was collected over 3 time points (pre therapy = self image index time1), (6 weeks post therapy = self image index time 2), and (follow up = self image index time 3).it is ordinal variable which range from 0 – 30.
variables:
1. gender variable is categorical variable and its values coded into numerical values ( 0= female, 1= male).
2. Age variable is continuous scale, measured in months.
3. Time 1,2,3 are scale variables and were converted into pre, post therapy and follow up.
4. Intervention/ control variable is categorical which was coded into numerical values (0= control group, 1= treated group).
5. self index time 1,2,3 are ordinal variables and were converted into parent rating scale pre, post therapy and follow up.
Results:
1. Are the delayed language affect interaction patterns and is the poor interaction affects language development? Is there a relationship between child’s language skill and parent child interaction?
A Pearson’s r correlation was carried out to investigate if there is a relationship between language skills and interaction patterns, as some previous studies revealed that delayed language skills affects negatively the interaction between child and his parents, and the poor interaction affect the child’s language development. For this reason, the pearson’s r correlation was carried out to investigate the relationship between PLS4 pre therapy scores and parent rating scale pre therapy. There is a significant positive relationship between language skill and parent child interaction (R(45) = 0.33; p= 0.025).
2. is there a difference between language skill before and after PCIT intervention? What is the effect of PCIT intervention on language skills?
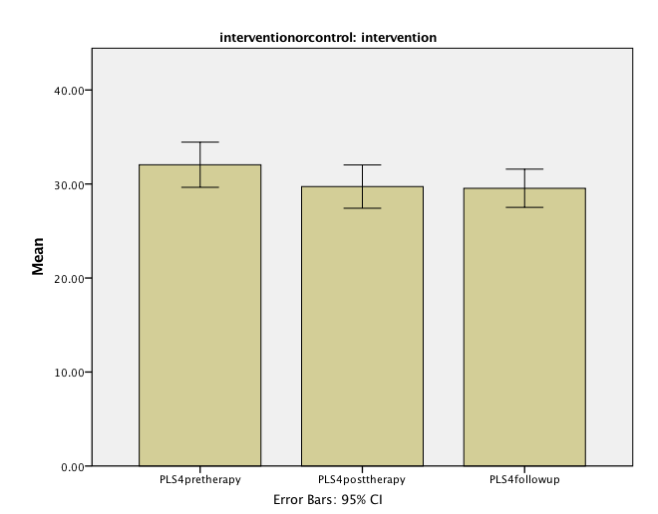
A one way repeated measure ANOVA was carried out to investigate the effect of the new intervention approach on development of language skills by comparing the difference between language scores (PLS4) over 3 time points (pre therapy, post therapy, and follow up). The findings revealed a significant difference in language scores at different time points (F (2,42) = 11, p < 0.05), with large effect size ηp2= 0.344. treated group scored better at pre therapy ( mean = 32.04, SD = 5.42) than at post therapy ( mean = 29.72, SD = 5.20) and better than at follow up ( mean = 29.54, SD = 4.59). additionally, pairwise comparison revealed that pre therapy scores were significantly better than post therapy and follow up scores (p = 0.006, p = 0.002), but the difference between post therapy and follow up scores were not significant ( p = 1.000 ).
A paired t-test was carried out to investigate the effect the new intervention approach (PCIT) on the development of language skill by comparing PLS4 scores before and after therapy among treated group. Before therapy Participants in the treated group scored significantly better (mean =32.04, SD= 5.42) than after 6 weeks after therapy (mean= 29.72, SD= 5.20) (t(21)= 3.534, p= 0.002).
3. Are the interaction patterns will improve after regular therapy of language skills?
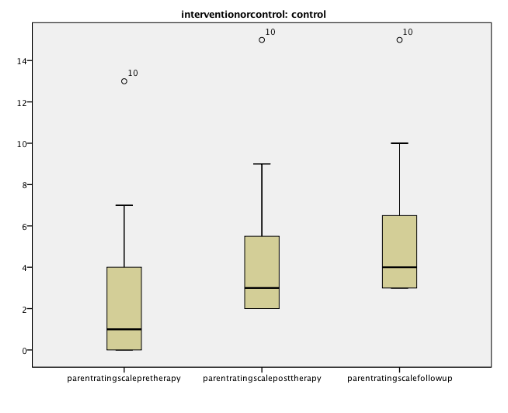
The impact of language therapy on the parent child interaction was investigated by comparing pre therapy, post therapy, and at follow up rating scale among control group by using Friedman’s ANOVA test. There was a significant difference in parent rating scale over the three time points (Friedman χ2 ( 2 ) = 42, p 0.001). The rating scale at follow up was better than at post therapy [(median = 4, IQR = 4), (median = 3, IQR = 4)] and the difference was significant (z = -3.83, p 0.001), also rating score was better at follow up than at pre therapy [(median = 4, IQR = 4), (median = 1, IQR = 5)] and the difference was significant (z = -4.41, p 0.001).Finally, post therapy rating score was better than pre therapy rating score [(median = 3, IQR = 4) (median = 1, IQR =5)], and the difference was statically significant (z= -4.563, p 0.001).
4. What is the difference between 2 approaches in development of language skills among children with language delay?
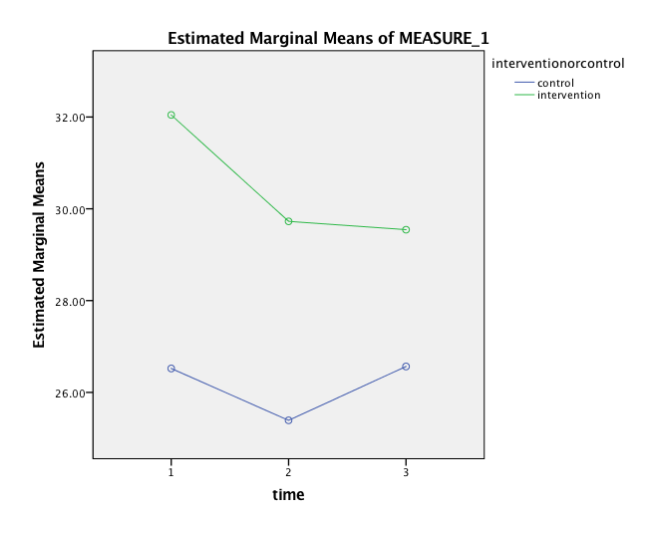
To investigate the difference between regular and new intervention, the language scores (PLS4) of the two groups will be compared at the three time points, therefore, two way mixed ANOVA was carried out. Means for language scores were decreased across time among treated group, from 32.04(5.4) to 29.72(5.2) to 29.54(4.5); whereas, the language score of control group deteriorated from pre therapy to post therapy [ 26.52(4.04) to 25.39(3.6)] but scores improved at follow up to be 26.56(3.3). the main effects of time and groups on language skill (PLS4) were explored by using a two way mixed ANOVA. There was a significant main effect for time F (2,86) = 13.84, p 0.05, ηp2= 0.244. Additionally, there was a significant main effect for intervention group F (1,43) = 11.48, p 0.05. finally, there was a significant interaction effect F (2,86) = 7.11, p 0.05, ηp2= 0.142.
5. Is the improvement of language skill among all participants due to different intervention approaches or due to age?
To investigate the linguistic scores post therapy of both groups when controlled the age variable by using ANCOVA. The difference between the two intervention was significant after controlling for age (F (1,42) = 10.19, p = 0.003). post hoc Bonferroni tests showed that PCIT group ( adj mean = 29.71, SE = 0.964) scored significantly better than language therapy group ( adj mean = 25.40, SE = 0.942, p = 0.003).
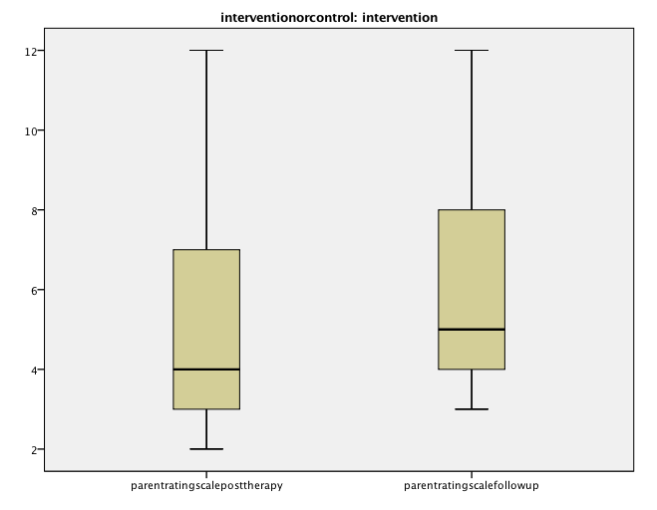
6. Are the modified interaction patterns will persist for long term period with PCIT group?

As some studies reported that one of limitation of PCIT approach is to generalize the modified interaction patterns by parents when the intervention was finished, therefore, measuring the difference in rating score between post therapy and follow up among treated group was carried out. Wilcoxon test was used and indicated the improvement of rating scale at follow up more than at post therapy, and the difference was significant (z = -4.47, p<0.001). which means the interaction patterns after the intervention terminated not only maintained but improved and generalized.
Discussion:
Parent child interaction therapy was investigated previously regarding its impact on child’s communication skills. However, PCIT impact on language skills has not investigated yet. Therefore, this study compared between this new intervention approach and the regular language therapy approach. Additionally, previous study did not include control group, for this reason, in this paper a control group was included how received the regular language therapy. The findings indicated positive relationship between language scores and parent child interaction pattern, which support previous studies, as they assumed that poor language affect negatively the interaction patterns and the poor interaction patterns affects negatively language development. The striking finding was that language scores did not improve after PCIT, that pre therapy language scores were better than at post therapy and follow up, and the difference between the three assessments was not by chance or random, it was statically significant. On the other hand, language scores of the control group who received the regular language therapy deteriorated from pre therapy to post therapy but improved at follow up, and the difference between three time points was statically significant. Notably, it was proved that interaction pattern may be affected by language score, as in control group where the intervention therapy was language focused therapy and not interaction focused therapy, nevertheless, the interaction patterns in the control group improved over the three time points and the difference between the three rating scales were statically significant. There was a significant main effect of time on the language scores and main effect of intervention and interaction between time and intervention. However, the language scores of treated group were better than language scores of control group before therapy, which means we have to interpret the findings with caution as the difference between the two groups in language scores may not due to the type of intervention but because of mismatching between 2 groups in language level. Finally, the different language scores between groups may due to different ages, therefore, ANCOVA test was carried out with controlling age and the finding indicated the significant difference between the 2 groups in language scores even after controlling age, which means the difference in language level is not because of age but it is a difference in language skills. As some studies reported that one of limitation of PCIT approach is to generalize the modified interaction patterns by parents when the intervention was finished, therefore, measuring the difference in rating score between post therapy and follow up among treated group was carried out and revealed that modified interaction patterns were generalize and improved after the intervention has been terminated as the difference between rating scale over the three time points of treated group was statically significant.
Using passive control group from the waiting list will be beneficial for future studies to investigate the effect of time, that any improvement is due to therapy and not because of language acquisition period, that the age of 0-5 years is the critical period for language development even without intervention. Also larger sample size is recommended for better generalization. Finally, children with different disordered and disabilities should be included in the future studies to investigate the effectiveness of PCIT approach for language development among more complex cases. This approach is cost and time effective, and it has been proved by clinicians to be effective, useful and within their recourses to do.
Implication for practice is to use this approach with children who have language delay or who have poor parent child interaction even with mild language delay,and to provide the language therapy approach for children who have more sever disorder and need language stimulated approach.
Looking for further insights on Overall Operative Time? Click here.



- 24/7 Customer Support
- 100% Customer Satisfaction
- No Privacy Violation
- Quick Services
- Subject Experts