Pressure Sores and Nursing Care
1.0 Introduction
Pressures sores, which are also known as pressure ulcers, decubitus or bedsores ulcers, are simply defined as a localized injury to the underlying tissues and the skin. Pressure sores often take place over a bony prominence. It usually results from prolonged exposure to shear, friction or pressure (Levine et al., 2013). Long term exposure to pressure leads to a decrease in the flow of capillary, blood and lymphatic vessels obstruction, and subsequent ischemia of tissue (Rich et al., 2011). Pressure sores affect individuals’ life quality through suffering, pain and loss of self-esteem. Pressure sores are also considered to be a burden on the economy. Risk factors as a result of pressure sores development include cognitive impairment, chronic illness, and poor nutritional status and mobility. It has been denoted that approximately 20 per cent of patients in community setting will develop pressures sores (Cooper, 2013). The highest percentage is generally observed in elderly patients suffering from orthopedic problems.
Pressure sores are often classified according to their severity. They range from stage one (least severe) to stage four (tissue loss and full-thickness skin). Stage four is considered to be the most severe stage of pressure ulcers. Notably, pressure sores deterioration is not necessarily a linear process. In some instances, the severity of pressure sores may be difficult to group into stages. In 2007, about 7400 individuals from different healthcare setting in the UK had pressure sores at the time when the data was reported. According to Solis (2007), individuals with pressure sores have disturbances of sleeping and limited daily living activities and social task. Caring for patients with pressure sores can diminish the quality of life aspect that relates to mental and social health amidst informal care providers (Gray, 2011). Pressure sores are a strain on NHS resources due to the fact that additional care is needed with regard to both treatment and staff time, they are equally expensive in terms of litigation. The cost of treating pressure sores has been estimated to be £1200 for stage one and £14000 for stage four. Guidelines of clinical practices are available to help in pressure sores prevention (Dealey & Lindholm, 2006). However, these guidelines are restrained by poor-quality evidence based on randomized trials that may have a high risk of bias (Moraes et al., 2012).
The continuous problem of pressure sores has additionally had an effect on nursing. Prevention of pressure sores have been identified as an essential nursing care aspect by the devolved and the national governments. In the UK, nurses’ code of conduct categorically stipulates that nurses have been entrusted with a mandate to ensure that patients are free from pain, comfortable and they live a quality life (Baumgarten et al., 2006). However, some nurses have been found to be reluctant in placing a high priority on an important aspect of patients care such as pressure sores. When considering investment in training and education, one clear explanation that is coming out is that poor care of pressure sores is as a result of behaviors and attitudes of the nurses. However, this is an explanation that is still under investigation by a big number of researchers. Predisposing factors are grouped as intrinsic (poor nutrition, aging skin, limited mobility and ageing skin) or extrinsic (moisture, friction, pressure, shear) (Krapfl & Gray, M, 2008). Pressure sores significantly tend to affect the wellbeing of individuals with limited mobility especially the elderly (Webster et al., 2011). Approximately 70 percent of pressure sores tend to occur among the people older than 65 years. However, young people suffering from severe illness or neurological impairment can equally be affected. The rate of prevalence ranges from 4.7 to 32 per cent in the community sphere. Pressure sores are commonly caused by unrelieved pressure that has been applied with an enormous force over a short period of time. It can also occur when low pressure has been applied for a long period. This effect results in disruption of the supply of blood into the capillary network, thereby impeding the flow of blood and curtailing nutrients and oxygen tissue (Schoonhoven, 2006). The external pressure must have a large impact in order to result into tissue damage, resultant ischemia and inflow impairment (Park et al., 2011). The commonly known sites for pressure sores include heels, lateral malleoli, greater trochanter and ischia tuberosity. In pressure sores, the risk assessment often begins by the identification of the risk factors and inspection of the skin. Pressure ulcers risk factors are grouped as extrinsic or intrinsic (Tchanque-Fossuo et al., 2011). It is essential that caregivers are educated about prevention and risk assessments, this will enable them to be in a position to carry out inspection among the patients in order to prevent pressure sore or identify them as early as possible. Assessment of risk can increase awareness, however, it has less predictive ability. Additionally, the risk assessment does not have any verified impact on pressure sores prevention (Clark et al., 2011).

Notably, measures of prevention should only be applied to risk patients. Reduction of pressure in order to preserve microcirculation is a preventative mainstay therapy. According to Li et al (2011), there is no documented evidence that is required for the determination of an optimal repositioning of patient schedule. According to agencies recommendation, from the Research and policy of healthcare, bedridden patients are required to be repositioned after an interval of two hours. It has also been suggested that in order to reduce shears, bed head should be increased in height by more than thirty degrees. It should also be maintained at a low elevation degree in order to prevent any possibility of contracting other complication (Krapfl, 2008). Some patients can diminish pressure sores or rather relieve themselves of pressure by the use of manual aids. Devices designed for reducing pressure can diminish pressure or can be used to relieve pressure. They are grouped as dynamic or static. These static devices include water, foam, gel, air mattress. Dynamic devices (low-air loss, alternating devices of pressure and air-fluidized surface) uses sources of power to help in redistribution of localized pressure (Linder-Ganz et al., 2009). Static devices are less costly and noisy as compared to dynamic devices. It has been denoted that Surface of pressure reduction tends to reduce incidences of pressure sore by approximately 60 per cent, a value which is much higher as compared to mattresses of the standard hospital (Terekeci et al., 2008). However, there is no coherent disparity between devices of pressure reduction. The benefit of static and dynamic surfaces is not coherent. Dynamic surfaces should be given consideration in circumstances where patients are not able to independently reposition themselves or if the patient has a sore that heals poorly. The device may not be effective if the material between the pressure sore and the bed is less than one inch and for that reason, an alternative device should be used. Other alternative devices that can be used to reduce pressure include foam wedges, pillows and chair cushions (Dealey & Lindholm, 2006). Ring cushion often is not used since they can cause points in pressure. Other interventions of prevention include skincare and nutritional evaluation (Cox, 2011). There is a close association between poor nutrition and pressure sores. However, a causal relationship that exists between the two is yet to be established. Recent research has demonstrated that supplementation of oral nutrition diminishes risk by a significant percentage. According to the Cochrane review, there is inadequate evidence that supports the relationship between prevention of pressure sore and nutrition. A meta-analysis carried out recently concluded that application of skin moisturizers and consultation of a dietitian are a more logical measure of prevention. However, the bactericidal role and preparation of growth factor are incoherent. Despite preventative intervention and proper evaluation of risk, some pressure sores remains inevitable (Hyun et al., 2014).
Established Pressure sore evaluation entails a complete and thorough assessment of the patient. A detailed history includes ulcers duration and onset, risk factors, previous care of the wound, and a list of medications and health problems (Yip et al., 2009). Other factors such as cognitive and behavioural status, financial and social resources, psychological health, and access to care provider are essential in the initial evaluation and can possibly control treatment plans (Gehin et al., 2006). Pressure sore presence may show that the patient is not accorded the necessary support or services. In many cases, the patient often needs proper support services, and for that case the caregiver should be offered good training or help in turning and lifting the patients. According to Thomas (2014) patients with sensory or communication disorder are more prone to pressure sores this is because they may not be in a position to express their problems in an ordinary way that can be easily understood. It is advisable that the physician should always take note of the size, location, and number of the sores and evaluate for the presence of sinus, exudate, odor, tunneling, healing, infection, undermining, wound margins, and necrosis (Hulsenboom et al., 2007). Additionally, the physician should identify the stage of every sore found. In an individual with dark skin, a stage one sore may appear as purple, red or blue discoloration (Cooper, 2013). Ulcer stage cannot be determined until a good number of eschar or slough has been eliminated in order to expose the wound base. Notably, ulcers do not grow through stages of healing or formation. The pressure sore scale can be used to monitor the progress of healing (Sewchuk et al., 2006).
1.1 Aim
The aim of this study is to explore the experiences of Community Nurses in preventing and treating pressure sores in the elderly population
1.2 Objectives
In order to meet the aim of this research, it was broken down into achievable objectives, which would later be met in the study. These areas presented below:
1. To provide an insight into the experiences of community nurses in preventing and treating pressure sores in the elderly population
2. To identify the interventions used in preventing pressure sores
3. To identify the risk factors of pressure sores
2.0 Methodology
2.1 Systematic reviews
Systematic reviews are a type of literature review that employs systematic methods in the collection of secondary data, qualitative or quantitative synthesis of findings, critical appraisal research studies (Chan et al., 2019). Systematic reviews frame questions of research that are narrow or broad in scope. It also determines and synthesizes research studies that directly relate to the creation of a systematic review. They are particularly designed to provide an exhaustive and complete summary of recent evidence that is pertinent to the research question (Kaufman et al., 2019). For that case, this study employed a systematic review to identify the challenges faced by community nurses in preventing pressure sores among the elderly. There are critical steps that must be included in a study when a systematic approach has been undertaken. First, the study should provide and an elaborate explanation concerning the output of the research both unpublished and peer-reviewed (Whiting et al., 2015). The type of study to be included is often determined by the research question and the objectives of the study. Secondly, when performing a systematic review is essential to consider the kind of persons who should be involved due to the fact that it may not be possible to perform a systematic review alone to satisfaction. In this regard, this study allowed for a collective collaboration librarian and supervisor who helped in the formulation of the search strategy. Additionally, it is important to use systematic review question tools to help in the formulation of the search problem. It is also essential to use critical appraisal tools to critically appraise the assessment quality (Shamseer et al., 2015).
2.2 Characteristics
The first step in carrying out the systematic review is to formulate a structured question that assists in guiding the review. The first step is followed by performing a rigorous search of the literature for pertinent papers (Moher et al., 2015). Systematic review methodology section list all the citation indexes and databases that were searched. For instance, Embase, Pubweb, Science web and any other journal that was searched. It should be noted that searching for various databases is a clinical trial for hallmark, and for that regard, there has been a wider recognition of the essence of applying various search technologies. The abstract and titles of articles identification are examined against criteria that are already determined for relevance and eligibility to come up with an inclusion setting (Dealey & Lindholm, 2006). Different steps have been identified when conducting this systematic review. The four main stages of a systematic review include:
1. Question definition and agreement on an objective method. This is regarded as one of the best practices to publish systematic review protocol prior to initiating it in order to prevent the occurrence of unplanned duplication and also to provide room for comparison of methods of reported reviews with what was schemed in the protocol (Chan et al., 2019).
2. A thorough search of pertinent data that are in line with given criteria. For instance, the selection of high-quality research that answers defined questions. A trained librarian or information professional can assist in improving systematic review quality (Chan et al., 2019).
4. Relevant data extraction. This generally includes how the research was carried out, the participants, what happened (research outcome) and the source of funding (Shamseer et al., 2015).
5. Analysis and combination of data. This is achieved through the use of intricate statistical methods of data analysis which provides the overall results from all the data (Whiting et al., 2015).
2.3 Hierarchy of evidence
Many scientific experts agree that when the study design is placed high up the hierarchy then there is a likelihood that the design of the study will refuse a bias effect on the outcomes of the study. For that reason, this study employed systematic review due to the fact that it occupies a higher position in the hierarchy of evidence (Prince et al., 2013).
2.4 Inclusion and exclusion of studies
2.4.1 Types of studies
Several approaches were covered in this systematic review such as qualitative study, grounded theory, descriptive approach and the use of phenomelogical approach. This study used up to date inclusion and exclusion criteria, as such, only relevant materials were thoroughly evaluated to meet the objectives of the study. Materials such as letters, discussion papers among others were excluded since they never met the inclusion criteria.
2.5 Types of participants
This study included elderly patients suffering from pressure sores and community nurses who have been entrusted with a responsibility to care for them. This study strictly based its findings within the community sphere and for that reason it excluded nurses and elderly patients suffering from pressure ulcers within the acute hospital setting. The study majored on elderly patients with a long history of pressure sores. This is due to the fact that comprehensive and accurate information could be gotten from. It excluded elderly patients with a short history of pressure sores.
2.6 Geographical context
The fact that pressure sores among elderly patients is a global challenge, there are a few studies that have been conducted within the geographical sphere of the UK (Chan et al., 2019). For that reason, this study included research that has been carried out in other countries within the community sphere. This research also narrowed review language to English.
2.7 The timeframe of the data
In this study, the type of studies and literature search that was employed in this study will be conducted between 2010 and 2019 in order to authenticate it is up to date, in terms of evidence and research.
2.8 Ethical consideration
This research was approved due to the fact that it met all ethical consideration, as such, all necessary efforts were put in place to ensure that there is transparency in the whole research. This has been achieved by acknowledging all individuals who put in their efforts so as to make this research to achieve its objectives. Secondly, this research has ensured that there is accuracy in the extracted data and therefore there is no attempt to slant extracted data in any form. Additionally, this research ensured that there is no form of duplication.
2.9 Bias
Systematic reviews are widely known to have several advantages. However, they are considered vulnerable to biases that tend to cover the true findings of the study (Prince et al., 2014). For this reason, it is prudent that they are interpreted with a lot of caution. This study reviewed a number of possible biases that could arise from the study. These biases include (1) Duplicate publication bias. This type of bias can lead to the introduction of a significant bias into a systematic review suppose the studies have been included inadvertently more than once (Kaufman et al., 2019). According to Moher (2015), several studies are often published in two or more journals in order to increase the effectiveness of the study outcomes and to maximise on readership. (2) Citation bias. The reference lists perusal of articles is commonly used to determine additional journals that may be pertinent, however, there is insignificant evidence present to back up the methodology. One of the major challenges with this approach is the fact that the process of citation of previous work is quite far from the objective and therefore retrieving literature by scanning the lists of references may result into a biased sample of studies. Citation bias may significantly affect the systematic review (whiting et al., 2015). (3) Language bias. Generally, reviews have often been published in English. For instance, all the thirty-six meta-analyses medicine journals that were reported from 1991 to 1994. Twenty-six restricted their search study to be reported in English. Notably, the effect and extent of language bias seem to have reduced significantly in recent years due to the change that has been made in the publication of studies in English (Prince et al., 2014). (4) The bias of reporting an outcome. In several studies, the outcome range measure is usually recorded but not everything is always reported (Shamseer et al., 2015). The choice of findings on what should be reported is greatly determined by the results. Outcome reporting bias contributes to total waste in research this is because it is a threat to the evidence.
3.0 Formulation of the question
A systematic review is generally based on a research question that has been predefined. According to Cochrane handbook, a well-formulated question assists in guiding a lot of specific review aspects process. These include determination of eligibility criteria, presentation of findings, search for studies, and collection of data from included studies. The research question should be focused and coherent. Some of the techniques commonly used to establish research questions include PICO- used to search for questions that require quantitative review. Where, P-patient population, I-Intervention, C-Comparison, and O-outcome (Chan et al., 2019). Another technique used in formulating research question is SPIDER- it is used to search for mixed methods and qualitative research studies. Other techniques include ECLIPSE and SPICE. This study however employed PEO technique as a way of formulating search question. There are three elements that are contained in the PEO strategy to ensure that all aspects of the search question have been covered.
Population- community nurses Exposure- pressure sores on elderly patients Outcomes- management and prevention
From the use of PEO technique, the following questions were formulated.
What are the challenges faced by community nurses in the management of pressure sores on elderly patients?
Are there perceived challenges faced by community nurses in the management and prevention of pressure sores among the elderly patients?
3.1 Search strategy
Systematic reviews extensively identify, search and summarise most recent evidence that answers a particular clinical question, with the help of a specific quality of methodology. When such reviews include meta-analysis then they are a position to provide accurate estimates of the treatment effect or association. These results can then be used to a greater array of patients that does not vary significantly from those covered in the summarised study (Price et al., 2013). This study employed various search strategy in finding a systematic review that was used to find out the underlying challenges faced by community nurses in the management of elderly patients suffering from pressure sores. These databases included cinahl full text, Medline, Pubmed and ebcohost. Finding of reviews in the Medline has two challenges. Only a small citation proportion in Medline are meant for literature reviews, and therefore only a small fraction is for systematic reviews. Additionally, the Medicine national library for Medline excludes systematic review as a type of publication. In this research, validation, generation and characteristics of the performance of the new search strategy have been included in order to help in the identification of systematic reviews in pressure sores.
3.2 Cochrane library
Cochrane database is the leading database and journal for systematic reviews used in healthcare. CDSR include protocols and systematic reviews for Cochrane reviews as well as supplements and editorials (Whiting et al., 2015). CDSR was extensively used in this research due to the fact that it is relevant in the healthcare. This study used protocols to synthesize and evaluate prevention techniques that can be used by the community nurses to help in minimizing pressure sores among elderly patients. According to Qi (2013) a protocol help in highlighting the question that is being addressed. It provides comprehensive information about the criteria against which the research will be evaluated in order to be included in the review. The protocol includes critical information that defines health challenges. Additionally, it contains intervention to be investigated, harms and benefits to be measured, and an appropriate type of study design. The protocol also provides the process of identification, evaluation and summarization of studies in the review (Prince, 2013).
3.3 Strengths and limitation
A small database subset was used in this research to derive out strategies, as a result, this approach may have overestimated the identified strategies performance metrics. Notably, the generation of the strategy was limited to the addition of terms (Boolean OR)); better-performing strategy may be as a result of the restriction of the adding terms by applying NOT operators and Boolean AND. However, Boolean AND typically reduced the sensitivity when testing was done with other excluded work in the database, on the other hand NOT operators led to significant improvement in the current research. According to Kitchenham et al (2015), users are likely to observe a significant improvement in a highly sensitive strategies. This implies that the number of reviews are reduced in order to get one systematic review on the topic. Strength of this approach is quite unique. These include a thorough process pursued in the generation of a criterion standard systematic reviews dataset, generation of search strategies and a large number of terms, and identification of appropriate strategies in subset derivation. This approach proved beneficial due to the fact that it yielded search strategies with optimal sensitivity and minimal terms, optimal precision, and precision and sensitivity balance that superseded the best-published strategies performance (Prince et al., 2013).
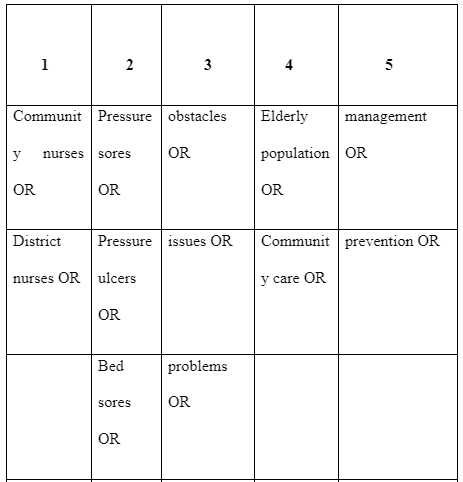
3.4 Table one
From table one, a number of key words that was applied in the search process is depicted. This was achieved through the use of thesaurus in order to find out various distinct words with similar meaning that could be used to search for the same explanation during the search process. Use of key words enables the database to find numerous citations that can be used in the literature search (Prince et al., 2014).
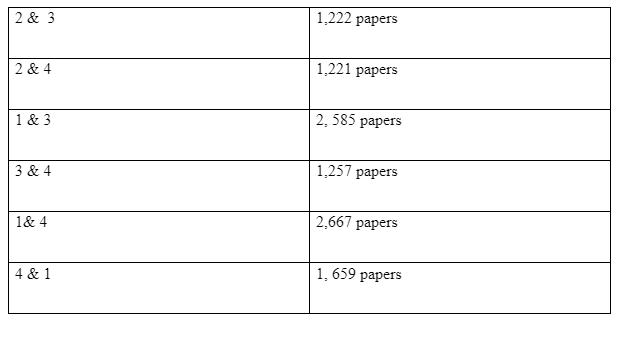
3.5 Table two
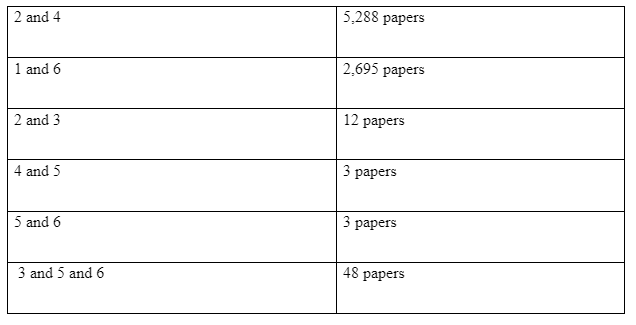
Table two shows the data that was used for the literature search for the whole process of review. It also illustrates the data which was used to identify common challenges faced by community nurses while caring for the elderly patients with pressure sores. From the search undertaken which is shown in table two, 30 papers were chosen to read from while basing the search process on prevention of pressure sores. This was done to identify the most common prevention techniques that can be used by district nurses to curb pressure sore among the elderly. In this study, a system of open coding was applied to help in coding pertinent information and also to group the papers into separate barriers so as to determine the common challenge faced by community nurses while addressing the issue of pressure sore among the elderly. According to Kaufman et al (2019), coding is generally used to differentiate categories and concepts. Therefore, it provides security for possible loss of information. From the 30 papers read in detail, management and prevention, elderly population, obstacle related search was chosen and most spoken about in the papers prevention of pressure sores was chosen for further searches. The following tables show the searches for the separate searches which was used in getting the information.



3.9 Excluded records
When a large volume of data on a given topic is being reviewed, not all levels of evidence are valued in a similar manner. Some data may not meet the inclusion criteria and therefore they are excluded from the study (Chan et al., 20190. There exist a scale that can be used in the stratification of evidence. They range from weakest to strongest. According to Shamseer (2015), randomized control trials systematic reviews have the highest level. There are various reasons why some journals may be excluded from the systematic review. They include; exclusion due to loss of qualitative data, repetition of publication, limitation of language, unavailability of full text, the disparity between the traditional protocols and the designed protocols, low-quality RCT among others. Notably, several journals that were excluded from this study were found to be having low-quality RCTs (Whiting et al., 2015).
4.1 Data extraction tools
While conducting a systematic review it was noted that the process involved a large amount of data and for that reason, there was a need to extract data from various relevant studies in order to facilitate examination and comparison of the results. While the data was being extracted, good practices of data management were employed and this helped in the determination of the type of data to be detained.
4.2 Data Synthesis
Literature provides several approaches for the synthesis of qualitative data. In this study, a narrative thematic approach was widely used. A narrative thematic approach can include both qualitative and quantitative data (Prince et al., 2014). The reviewers study an issue and then interpret data in order to create an overarching summary of different outcomes. This entails data iterative exploration rather than literature exhaustive search. Thematic analysis assists in the determination of a number of factors that are important in comprehending a given phenomenon, which in turn puts factors into themes and subthemes (Moher et al., 2015). There was a division of papers into different themes. However, all papers had moved over on every theme. For that reason, an extensive analysis was done for all the themes. After analysis of all the chosen papers, data was determined. Data that met the inclusion criteria was extracted and written in the findings chapter.
4.3 Critical appraisal
This research employed appraisal tools that have been developed by the Joanna Briggs Institute. JBI is an international, development and research organisation that has been recognized globally. The institute has specialized in supporting and promoting evidence-based healthcare. According to Kaufman et al (2019), systematic reviews integrate appraisal or critique proves of the study evidence. The aim of this appraisal was to evaluate the methodological standard of this research and identify the degree to which the study managed to address the arising bias in its analysis, conduct and design. All the papers that were chosen in the systematic review were subjected to thorough appraisal by three important appraisers. The outcome of the appraisal was then used to inform the interpretation and synthesis of the findings. In this study critical appraisal skills tool checklist (CASP) proved to be important due to the fact that it helped in identifying essential papers that needed to be included in the study. Additionally, it helped in identifying some studies that were not pertinent to the area under review. Appendix 1 shows an example of CASP that was used in completion of the seven papers.
5.0 Results and Findings
5.1 Characteristics of the studies
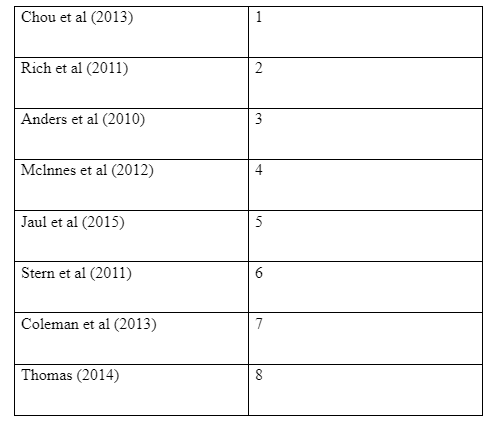
Eight studies were conducted in nine different countries and it was ascertained that they conformed to the criteria and that they were done between the years 2010-2018. 2 separate studies carried out in Australia and the remaining studies in Italy (n=1), France (n=1), South Korea (n=1), Portugal (n=1), Brazil (n=1), Chile (n=1), Germany (n=1), and Agentina (n=2) related to the English Language bias of the databases examined. The standard method used uniformly in these studies was qualitative methods data collection.
5.2 Critical evaluation of the methodological quality of the studies
All conducted studies were severe and conformed to the longutual approach. Furthermore, each method upheld confidentiality, and maintained a deep ethical standard. Out of all the studies, three of them employed use of focus groups for their method. They included a series of 26 subjects grouped such that each group had a minimum of 3 and a maximum of 8 people. Whitting (2015) submits that there is ideal number of participants who must be contributing to a certain focus group. However, it was established that a maximum of 10 people ensures that the group is up and running. The studies adopted a policy that capped the number of participants. Using people who are less than 10 makes it manageable. Focus groups were included as a means of study because they enable the bringing together of collective methods views and meanings that guarantees a deep insight into people’s beliefs and attitudes. During the study, only 6 focus groups did not maintain the researcher to take charge of the discussions on the premise that they would do so based on their own points of view. Instead, different people were contracted to carry out the focus group. In the 6 special focus groups, the researcher carried out the research themselves so that they may have an understanding of the objectives they desire and be able to make an informed bias analysis. This would have been relied upon fully if several other independent researchers were contracted to perform the same .Despite this limitation, the published results were insightful and was relevant according to the study. Despite being subject to further review, it was included after critical analysis. In contrast, the other four studies employed semi- structured interviews (3, 4, 6 and 7). 1 study used methods consisting of both focus groups and interviews (4). Gehin (2006) admits that because they are conducted face to face, semi-structured interviews have the researcher at an added advantage as he can control the interview and uphold the quality of data captured. It is largely reliant on the ability of the researcher to be a good listener and or ask the right questions. The need to ensure high quality work is produced, standard Interview guides were used to regulate all the 5 studies that employed this method. All the studies done by the employed interviewer took between 20 and 35 minutes instead of the planned 25 minutes. This is attributed to the greetings and introduction that comes before the actual study. It is worthwhile to note that studies 3 and 5 recruited subjects from rural based community nurses and study 1 paid attention to recruits sourced from one health center. This makes the sampling of the study used specific in that sense. The result cannot be confidently used to generalize the information presented. Effective sampling could have been achieved had other means been used to bring on board diverse array of participants. Finally, this evaluation used the same type of analysis procedure for all the studies conducted. The narrative thematic analysis is used to code and synthesize the collected data for presentation. This method ensures uniformity that enables standardization of the results needed. There are many other advantages of this analysis method that does not lie within the scope of our analysis today. This final step of data processing employed a set of other researchers who were not privy to the findings of the raw data from the field to avoid bias.
5.3 Results of the findings
The result shows a wide range of problems faced by the community nurses dealing with pressure sore management. They vary from different aspects of legal system, patient health status, nature of relationship between the nursing staff, incompetence and unwarranted patient disturbances among others.
5.3.1 Threat of legal accountability
Patients as well as their kin now are more willing and capable of taking legal action against community nurses due to the suffering and pain caused in one way or the other when in the care of a professional resulting in pressure ulceration. Normally, the penalties are always sued for; with the lawsuits coming down on the nursing homes and establishments that the community nurses work under. This is irrespective of the fault coming from the community nurses. Lately however, community nurses have gradually been held responsible for pressure ulcers. Some governments worldwide have advocated for prosecution of some professionals whenever pressure ulcers has led to the death of the patient involved. Some prosecutors have brought criminal charges against persons and institutions (Thomas, 2014). All this development is premised on the fact that “ignorance is no defence”. Proper knowledge of basic common anatomical sites susceptible to pressure sores and how to avert their formation is a fundamental aspect of nursing which every community nurse is expected to know. Failure to know could be interpreted as ignorance and thus is deemed punishable. The only way out for one is to muster and perform the clinical guidelines which certainly improve healthcare.
5.3.2 Questionable bandaging skills
Insufficient knowledge and practical skills around leg ulcer management. Some community nurses underscored that despite being a requirement of their profession, they complained that there was scanty knowledge about standard leg ulcer practice. 3 journals showed that there were negative changes with respect to the volume and quality of coaching they could access. Within the same establishment, the bandaging for instance was not standardized as dictated by best practice. Such operational discrepancies show the questionable level of organisation. According to one journal, this could be either interpreted as some participants getting a chance to participate in the training whereas some were denied access. Some participants even noted that their colleagues were not as good as them (Rich et al., 2011).
5.3.3 Community nurses’ wrangles
Community nursing is a teamwork involving all the players taking part in the healing process of the pressure ulcers. Wrangles however leads to total chaos that hinders perfect service delivery to the patients. Teamwork is a tenet of the nursing profession just as it is in every other field .1 journal shows that this is true. It enables the workers to work together in harmony. Absence of harmony may cause documentation errors which may have been done deliberately to make the other community nurses to have a hard time dealing with the patients during their shifts. The pressure sore patient ends up paying the price of warring co-workers either by aggravated wounds or even end up dying (Anders et al., 2010).
5.3.4 Prolonged immobilization of patient
Patients who have been bed-ridden for long have a higher risk of suffering aggravated wounds further making the pressure wounds harder to manage. The known pressure points are limited and therefore for very long periods of immobilisation, the patient could lie on the areas susceptible to pressure ulcers for way more than the 2 hours turning limit. When someone is not mobile and not active, the skin and the subcutaneous layer experience pressure by the say a mat. Bony prominence that bear heavy weight are the most predisposed to bedsores whose formation further complicates the care of the professional. The areas susceptible to bedsores include the heels, lateral malleolus, medial malleolus, fibular head, and the medial condyle of tibia, ischial tuberosities, greater trochanter, sacrum, elbow, scapula, ear and the occiput (Stern et al., 2011). While in the same state, the patients who have developed some pressure sores say in the sacrum due to the prolonged immobilisation may pass stool and urine thereby soiling themselves. These wastes may find a way into the wounds and cause devastating outcome of festering them. Such a happening complicates the situation for the professional caregiver who has to clean up the bedding, the sores and time the patient so that such a misfortune does not happen again .It also lengthens the convalescence period .This is results in more work for the community nurse.
5.3.5 Poor nutrition
Nutritional inadequacies, metabolic disorders and deficiency of iron element in the blood contribute to development and sustainment of pressure sores. Any type of anemia in the body greatly exposes the patient to bedsores regardless of its cause. Poor feeding habits can lengthen the inflammation phase of bedsore healing and or as a result compromise the strength and a quality of wound healing. All the 8 journals show that serum albumin below 3 grams per dL are related to hypoalbuminemic tissue edema and increase risk of bedsores. Going by these findings, we see that any development that seeks to impede quick recovery of a patient under care is a problem to the community nurse. Lack of or inability of the patient to purchase a given dietary arrangement leads to poor nutrition which impact inflammation tissues negatively. This forces the professional to give more care and or even overstay their contract (Chou et al., 2013).
5.3.6 Limited resources
Community nurses who are professional caregivers take an oath of service to stick by their patients accordingly and be selfless in their service to them. Those personnel that are operating in remote parts of the world with little or no supply of recommended products are forced to improvise to ensure survival of their clients. Lack of resources forces the community nurse to settle for makeshift solutions. For instance, the cleaning and dressing product for the pressure wounds the ensuing lesions is the zinc oxide. However, in its absence, one is forced to improve to use the Vaseline according to 5 journals. The zinc oxide is by far more potent when used compared to when the Vaseline petroleum oil is used. Such inadequacies make the caregiver under review to take longer time to dispense his or her services and this runs a high cost of treatment on the patient (Mclnnes et al., 2012). Other examples include usage of rag clothes (old clean clothes) whenever bandages are fully spent. Whereas the bandage could be disinfected using a disinfectant, it is not as compact and comfortable as the bandage itself. Even so, despite the disinfection, we cannot guarantee that the rag is safely sterilized.
5.3.7 Dysfunctional system
Community nurses always works to ensure that services given to the bedsore patient are personalized and attentive as much as much as possible. This shows us that the caregivers feel disenfranchised and are given something that they did not sign up for. Despite the zeal to serve a patient with pressure pores for instance, they see no reason why they should not quit. They may feel that the medical system is too large and too complex for them to actually have any significant impact. This unfolding results in professional dissatisfaction. Literally every gifted person I come across who is still in or has already graduated from the medical school in any capacity is always proud of the hope and faith the humanity bestows upon them to help keep them safe and secure from all medical related harm. Therefore, it is clear that the driving force is service to the community and the appreciations here and there which keep them going. Imagine a rot that that stems from too much bureaucracies, poor working conditions, unfair wages and rude supervisors. This is a meltdown that lowers the morale of the community nurse and reduce their work to nothing. Some would embrace neglect of the patience to cope up with the status quo or go out on strike. The above factor is a conglomeration of emotional, socio-economic and political statement (Andres et al., 2010).
5.3.8 Inadequate caregiving personnel
All the 8 journals underscore that a given set of patients being monitored by community nurses require a given number of professional caregivers to take care of them. To understand the statistical specifics of this matter, the areas susceptible to pressure ulcers have a maximum of 2 hours period which must not elapse before turning of the patient in the bed. Aside from other services a given community nurse is mandated to do, he or she must see to it that all the bed-ridden patients under his or her care are turned (Rich et al., 2011). Suppose one is charged with more patients that he can manage to comfortably handle, there will be a crisis that will result in most of the patients developing pressure sores due to an operational negligence. Such like are the cases that occur in isolated areas with few personnel to take adequate care of the needs of that area. Other notorious areas are underfunded government hospitals or the overcrowded national referral hospitals. Ambitious private start-up hospitals are also complicit with this vice to get large turnover by using as few human resources as possible. However, this is one of the easiest challenges to solve.
5.3.9 Patient preference
It should be noted that just like any other buyer (of services in this case), the bedsore patients are free humans with the will to choose and make decisions despite their temporary physical impairment. Some patients pay a lot of money for such kinds of services and the sad part is that some want the bandages and some don’t bother. Of those who had the bandages, some would opt to have them removed as it was too hot and sweaty. This is most common during the sum mer. This decision is understandable as it is based on the harsh prevailing weather condition. One could therefore comfortably say that the reason is well informed. Some other patients complain that they are tight and bulky according to all the 8 journals. This they do as soon it is put to take care of their wounds. It is important to note that the bandage is put appropriately for every type of patient irrespective of their class of race once they develop the bedsores. Therefore, the only reason one may quit on the bandage considering constant weather conditions is for person beliefs or others such as religion. With regards to religion, some of them consist of staunch members that believe that healing can only be achieved by divined intervention by their deities (Thomas, 2014). The faith cuts too deep to allow a qualified caregiver the opportunity to attend to them. Any attempt to offer services are immediately declined and any attempt to coerce cooperation could lead to verbal or physical assault. The community nurse is therefore always on a tight leash and is restricted by the types of patients they can attend to and the places they can actually to. They are not able to attend to certain minorities who believe that ultimate deliverance comes from their supreme healer. It rests with the Community nurse to make a decision on whether to risk his or her life to attend to the deeply conservative patient notwithstanding or chose to abandon the oath sworn to offer care to one and all irrespective of their biases and leanings in life. The community nurses could also be forced to join security forces deployed to quell armed resistances in areas with a prevalence in bed-ridden patients who do not support the new ways thereby further aggravating the expected retaliation by the people. This further risk their life. It is sad and when looking at the rational aspect, it is uncalled for that a given people can actually fight help coming their way. Such like problems encounter the community nurses.
5.4.0 Impaired sensory Cognition
Dealing with patients that have developed appreciable impaired sensory losses and are unconscious are difficult to handle. When the patient is paralysed for instance, they have lost the sense of touch and therefore that of pain in the area of paralysis. They are therefore not aware of the discomfort that could help them note and report to the qualified caregiver of the necessary action to take. Aside from the 2 hourly shifting of the position of the patient that is well known, the community nurse relies on complaints by the patient to actually take the necessary action to help alleviate the probability of bedsore formation. The underlying result is that the patient will not frequently change their position due to no report of pressure discomfort from the patient (Stern et al., 2011). The prolonged pressure slows or stops flow of blood and some tissue fluid. This impedes the necessary nourishment of the skin and the neighbouring adipose tissue which work in coordination and in tandem to maintain the integrity of the skin. All the 8 journals show that pressure ulcers have a higher chance of occurrence in paralysed patients than patients with all their faculties working properly. And this all takes an even shorter time duration to develop. The community nurse will thus be forced to be at the bedside of the patient round the clock to ensure quality care. Alternatively, they may be forced to increase caregiving nurses to increase quality of health. This stretches the nurse due to the increased volume of work.
5.4.1 Effects of gerontological considerations
In three journals, we established that in the aged and the elderly patients, the expected aging process causes reduced epidermal thickness. Also affected are the dermal collagen and tissue elasticity. The result of this development is a drier than normal skin which as pointed above is caused by the reduced sebaceous secretion. Sweat glands also take a dip in activity leading to reduced sweat given out as waste. Prominence of bone structure and muscular atrophy follow. These developments make the elderly predisposed to pressure sores and therefore the problem comes with tasking activity of taking care of them. They have even more pronounced pressure ulcers with more pain and more suffering (Mclnnes et al., 2012). The community nurse has to watch as the elderly lives a low quality of life couples by the fact that they are also susceptible to diminished sensory perception. It is true to point out that older patients are the worst hit of all the patients and the professional caregivers have to watch as they live out their last miserable days.
5.4.2 Additional tasking responsibility
The community nurse is forced to take part in other auxiliary services other than those they are contracted to do. In this instance we study the additional responsibility of acting as the patient’s Advocate. Advocacy for the well-being of the patient has been stressed in several integral community nursing forums as an important aspect of life. They may include but not limited to the summation of caregiving, offering of the expected emotional support and enlightening the patients and their immediate family on the necessary knowledge needed to enhance the patients’ quality of life (Jaul et al., 2011). They could also include helping with compensation for loss of the bodily functions. This helps the patients be able to stand up for themselves as they are empowered. Generally, the underlying principle of this advocacy is help monitor and adjust status of the patient. All these must be championed for since they cannot just appear. The community nurses are forced into a series of policy making process followed by the complicated appropriated and implementation of the suggestions. The community nurses seek to alert the institution managements and boards on the safety and risks facing patients. The other problem faced in this matter is the fact that only nurses are uniquely endowed with the relevant expertise to come up with such policy formulation. They are likened to the cord between quality life of the bedsore patients and quality healthcare. This is captured in one of the journals studied. When they are not appreciated enough to be comfortably brought wholly on board, they may not give their best. Also, they are the only ones who are both technically and legally qualified, provided other players do not take part in such undertakings, the right kind of content will be produced and used (Jaul et al., 2015).
5.4.3 Limited exposure in complex bedsores
The community nurses in 3 of the journals studied have some complaints about limited exposure to certain instances of pressure sores and it is worth it to note that this observation is quite different from incompetence (lack of basic nursing knowledge). We have seen before that colleagues from the same health establishment have reported that there is favoritism in giving the appropriate training. In this respective however, we observe the limited knowledge not based on the requisite knowledge but the vast hands on experience accrued by giving continual pressure sore management care to a series of different patients with different attention needs in different parts of the country (Chou et al., 2011). A community nurse could be aware of how to care for a typical patient. For instance, a patient admitted into a care due to a conventional bacterial infection. The patient has a defined care protocol. However, caring for a patient with very special need could prove tasking and very hard. Beginning community nurses could have very little on how to deal with an elderly patient with several terminal illness and has a limiting physical impairment. The situation may prove even harder if the same patient has been on a poor diet and has poor blood circulation to some parts of the skin covering the pressure points. It gets even interesting when one asks the course of action to be taken if the patient has declined some packages of assistance like covering of the bedsores using bandages (Rich et al., 2011). Alternatively, the patient may be cooperating but the weather and climate may make the sweaty patient infect the ulcers. All the 8 journals used in the study have not addressed such a happening and have the professional caregivers with nothing concrete. Despite the chances of such an occurrence being bleak, such examples could occur making the care management ineffective thus putting the quality of life the patient in jeopardy. The patient could succumb to a devastating infection.
5.4.4 Lack of clinical guidelines
According to 2 journals it is noted that there is almost a lack of conclusive clinical guidance on how to manage bedsores. This is a major problem for the community nurses. However, they are not free from blame because they have been reported to show unsatisfactory compliance with the drawn clinical guidelines on how to combat development of pressure sores. They could argue in defence that they meet different guidelines which have conflicting directions and chose to cherry-pick sound steps from various sources and come up with systems they think would work for them. We are shown that the other form of lack of guidelines comes about as follows: following the complex nature of the number and type of patients attended to, it is very hard for the caregivers to follow through with care. In the case of a single community nurse for several patients, the care is given intermittently for all of them making it difficult for him or her to capture all data of the patients for future reference. This problem sets precedence for a dangerous care package for all the patients attended to as the professional caregiver will not have the much-needed history for reference but will resort to his or her instinct which. They therefore give care that they think is appropriate for that day. This is both lack of planning and individual based guidelines which could be attributed to limited time and other resources. This results in unnecessarily long healing rates (Stern et al., 2011).
5.4.5 Poor documentation and communication
Poor documentation and general communication are a major hindrance of quality healthcare for patients with pressure sores. These two are mentioned to be notorious in the process of trying to make bedsore care a success. This leads to questionable handovers from one community nurse to another. Suppose two nurses are writing down a given patient’s information and do a poor job of correctly capturing the observed information, they may relay different necessary course of action to be taken. You could find two caregivers arguing over what to do with a patient instead of referring to the record-book and this alone creates doubt. Those charged with initial assessment of the patient could be charged with professional negligence. They make the next handlers not well briefed on the care plans. As a result, even following the sanctioned course of action could lead to formation of the pressure ulcers one seeks to prevent and manage in the first place (Coleman et al., 2013).
5.4.6 Little respect for the pressure sore caregiving
Generally, the community nurses according to one journal view pressure ulcer prevention to be not as important as the other aspects of the nursing profession. This attitude influences how the other nurses respond to call for help from patients or their colleagues for assistance. It directly undermines the healthcare management plans and guidelines of the patients. One professional caregiver could decide to be unethical and totally ignore a caregiver and other patients seeking for help (Thomas, 2014). Alternatively, they could choose to give poor quality services which may cause formation of pressure sores anyway. Even worse, providing care half-heartedly could lower the morale of a patient who may give up their fight and succumb to their ailments.

Discussion
The results and findings of this qualitative review show the problems faced by community nurses when managing pressure sores among patients. There arose several themes which were conclusively addressed to highlight the objective under review. They include legal, nutrition, establishment management and relationship between the community nursing colleagues, availability of resources and the patients’ health status and preferences. Sub-themes stemming from the above mentioned were studied. The threat of legal accountability was put in place after several years of deliberation to ensure that the community nurse are answerable for every decision they take during caregiving and medical records are presented in court during litigation. This is to keep the caregivers in check and ensure that best medical practices are maintained. This is a problem because the community nurses cannot dare help save patients with other working methods which are not technically sanctioned and thus limiting the quality of life for the patient (Anders et al., 2010). Community nurses with questionable bandaging skills put the lives of the patients at risk and even in case they survive such an ordeal, they could have a generally poor quality of life. The caregivers have little confidence to manage patients and whenever they do so, they offer low quality care. This prevents them from proper patient management. Quality pressure sore management by community nurses of patients greatly depends on the good relationship between the nursing colleagues and thus any misunderstandings may put his or her life at the mercy of flaring tempers. A patient’s data could be withheld during handover forcing the community nurse in care to give the care he or she thinks is appropriate at that time. Alternatively, the patient could be physically injured or entirely neglected (Qaseem et al., 2015). Poor nutrition by the patient who is currently under care as well as metabolic disorders and anaemia in the body is a major problem. It is understood that lack of iron leads to development and sustaining of pressure sores in the body. Failure of a patient to buy a given diet impacts inflammation badly causing pressure sores to heal slowly. They also do not heal properly.
Patients who have been in admitted for long have a high risk of getting pressure ulcers due to the limited time required to constantly change his or her sleeping position. Caregivers are more likely fail to make constant checks due to their long stay. When the patient soils himself due to his state of continuous immobilisation, he may cause further infection on the already formed bedsores. Limited resources to be used to help in the care of the patient range from those that help prevent formation of pressure ulcers to those that help with the treatment of the already formed ones. The example given in this study was the community nurse opting to use the Vaseline petroleum jelly in the place of the standard zinc oxide. It will work but not as efficiently as the missing component causing the caregiver to spend more time with the patient than had probably been planned for (Baumgarten et al., 2012). Inadequate professional caregivers result in a situation such that the patients being managed are not receiving the best medical care. They are more likely to develop bedsores. Areas that are susceptible to pressure ulcers have a maximum of 2 hours within which a patient must be turned. This necessitates that patients have adequate caregivers. Community nurses are aware that the patients have a right to choose how they are treated. Some patients could choose to not be dressed in the bandages for any number of reasons and this complicates the situation of the professional caregiver who either has to find another way or try to convince the patient to accept the bandaging (Rich et al., 2011). Addressing the needs of patients who have advanced loss of sensory faculties or are partially unconscious is tasking. They have no sense of touch and may not be able to feel pain. When the maximum time of 2 hours for the tissue integrity to withstand pressure has elapsed and the caregiver is away, the patient develops pressure ulcers. Such occurrence force the community nurse to be around at all times.
The elderly patients are aged and thus have reduced epidermal thickness. Also, they have a skin that is drier than the normal skin which is caused by reduced secretion from the sebaceous glands and reduced sweat output. Prominence of bone structures and atrophy make the aged population predisposed to pressure sores. The problem is the management of the elderly which is very tasking when compared to the average aged patient. There is a general view among the community nurses that bedsore management is not as important as other aspects of community nursing hence it is not given the respect and attention it deserves. The developed attitude undermines service delivery on the both fronts of the caregiver and the patient (Teague et al., 2011). Nurses may fail to offer help where needed or even give poor quality services. Patients who feel neglected may choose to give up and succumb to their sicknesses. Poor documentation and general communication of the patient data from the community nurses who did primary assessment to those who take up the care during takeovers can lead to argument over the type of care to be given to them. This comes about when the patient’s data were not properly captured. In case such issues are not sorted, the caregivers currently in charge are thus left to take steps they deem appropriate which may not be good enough. There is limited exposure of the community nurses to complex bedsore management care. This involves patients with complicated medical status. Instead of a typical patient admitted with one of the common diseases, a caregiver would have a hard time to take care of an elderly patient with a terminal ailment and has a physical handicap probably on a poor diet, has anaemia and has personal and religious bias against conventional medical dressing of ulcers. Few community nurses have a working special guideline on how to handle such oddities. Dysfunctional system expects the community nurses to work based only on the drive of the need for community service alone and makes little investment. There is an array of rot within the system from poor funding to corruption, poor working conditions, rude supervisors and low wages. This meltdown lowers the drive of the professional caregivers to give their best services (Jaul, 2010).
Strengths and limitations of the study
In the systematic review that was used the study, there arose several concerns. 8 journals were used for the review out of which only 7 proved informative when considering the material content. Journal 6 had little knowledge on the matter under review and was not conclusively addressed hence could be attributed to either wrong choice of research literature or lack of prior attention on the matter. The collection of the data used in the study was strictly qualitative. It has its advantages and disadvantages. Adoption of a more holistic approach involving usage of several other approaches alongside the qualitative review would result in a more conclusive and complete conclusion on the problems facing community nurses who are managing pressure ulcers among the bed-ridden patients (Dwan et al., 2013). The other problem faced was the limited access of some of the best journals used for the study. Even when found, the journals accessible were either very expensive or for those in the local library collection, when requested took a long time to be dispatched. Some papers asked for from the library did not even get reply. Narrative thematic analysis was employed to synthesise after coding the data for this review. The other journals from which this study is based had used several conflicting analysis methods in terms of formatting and objectives to be achieved and therefore relevant information came up with from one journal could not be applicable in this case.
The systematic review involves critical review of information from a series of secondary sources of data and therefore needs thorough research and spending a lot of time resources into it. Also, it needs a reading culture that has been inculcated into the researcher over a long period of time. Lack of such kind of drive could prompt one to do a shoddy work. This is common with the critical systematic review (Prince et al., 2013). This is unlike the primary collection of data which involves interacting with other people on a larger scale.
Conclusion
The 8 journals used for the study proved helpful in debunking the problems facing community nurses when combating pressure ulcers. We see that there are several reasons that make the care of these professionals fail to be absolute. They vary from the risk of legal accountability on the part of the concerned nurse. This raises fear and apprehension among them. Some include poor bandaging and general sore-dressing skills of the community nurse. They help exacerbate the condition of the patient. There are reports of limited exposure to more complex patient condition resulting in the need for more attention and specialised adjustments to the general clinical guidelines to be followed (Litchford et al., 2014). Still, on the side of the community nurse, there is the poor documentation and communication as appertains to the health assessment of the patient thereby throwing their well-being into a disarray. The disturbing report of little respect accorded to the pressure sore management care by the community nursing fraternity and the opinion that it plays a second fiddle to the other more important aspects of nursing. On the part of the patient, the limitations faced directly range from prolonged immobilisation of the patient which comes with its set of problems as addressed before. Others stem from the impaired sensory cognition, the special aspects associated with the gerontological considerations and poor nutrition which is mainly brought about by poverty. Findings from this review can help the relevant authority with the guidelines on how to best combat the challenges facing the community nurses and give them the platform to perform at peak.
Future research
Resources have to be channeled to a future research into why the community nursing fraternity has little respect for the pressure ulcers management care and establish if some of the problems they face have a direct relationship with this subject. Another area of interest would be to study why some community nurses would deem it fit to train some caregiving colleagues and exclude others for whatever reason. Finally, I would recommend a further study into why there is lack of clear guidelines on how to deal with pressure sores and whenever there are developments, the nurses opt to violate them.
Implications to clinical practice
The findings of this study could be deliberated on to come up with solutions as is the objectives of every research. The insight can help the community nurses or those that head organized group of caregiving professionals come up with policies to help solve the pointed problems. For instance, they have a chance of figuring out to navigate the personal, cultural and religious beliefs of the patients under their care to help them achieve the best quality of health. They find a chance to advice on alternative diets and healthy living. Finally, they get the chance to work on their interpersonal skills that helps them integrate well into the community nursing fraternity. This improves the quality of healthcare by providing a healthy working environment (Park et al., 2016).
References
- Jaul, E. (2010). Assessment and management of pressure ulcers in the elderly. Drugs & aging, 27(4), 311-325.
- Teague, L., Mahoney, J., Goodman, L., Paulden, M., Poss, J., Li, J., ... & Krahn, M. (2011). Early prevention of pressure ulcers among elderly patients admitted through emergency departments: a cost-effectiveness analysis. Annals of emergency medicine, 58(5), 468-478.
- Baumgarten, M., Rich, S. E., Shardell, M. D., Hawkes, W. G., Margolis, D. J., Langenberg, P., ... & Kinosian, B. P. (2012). Care‐Related Risk Factors for Hospital‐Acquired Pressure Ulcers in Elderly Adults with Hip Fracture. Journal of the American Geriatrics Society, 60(2), 277-283.
- Chou, R., Dana, T., Bougatsos, C., Blazina, I., Starmer, A. J., Reitel, K., & Buckley, D. I. (2013). Pressure ulcer risk assessment and prevention: a systematic comparative effectiveness review. Annals of Internal Medicine, 159(1), 28-38.
- Qaseem, A., Mir, T. P., Starkey, M., & Denberg, T. D. (2015). Risk assessment and prevention of pressure ulcers: a clinical practice guideline from the American College of Physicians. Annals of internal medicine, 162(5), 359-369.
- Rich, S. E., Margolis, D., Shardell, M., Hawkes, W. G., Miller, R. R., Amr, S., & Baumgarten, M. (2011). Frequent manual repositioning and incidence of pressure ulcers among bed‐bound elderly hip fracture patients. Wound Repair and Regeneration, 19(1), 10-18.
- Anders, J., Heinemann, A., Leffmann, C., Leutenegger, M., Pröfener, F., & von Renteln-Kruse, W. (2010). Decubitus ulcers: pathophysiology and primary prevention. Deutsches Ärzteblatt International, 107(21), 371.
- McInnes, E., Jammali-Blasi, A., Bell-Syer, S., Dumville, J., & Cullum, N. (2012). Preventing pressure ulcers—are pressure-redistributing support surfaces effective? A Cochrane systematic review and meta-analysis. International journal of nursing studies, 49(3), 345-359.
- Mervis, J. S., & Phillips, T. J. (2019). Pressure ulcers: prevention and management. Journal of the American Academy of Dermatology.
- Jaul, E., & Calderon‐Margalit, R. (2015). Systemic factors and mortality in elderly patients with pressure ulcers. International wound journal, 12(3), 254-259.
- Stern, A., Chen, W., Sander, B., John-Baptiste, A., Thein, H. H., Gomes, T., ... & Krahn, M. (2011). Preventing pressure ulcers in long-term care: a cost-effectiveness analysis. Archives of internal medicine, 171(20), 1839-1847.
- de Souza, D. M. S. T., de Gouveia Santos, V. L. C., Iri, H. K., & Oguri, M. Y. S. (2010). Predictive validity of the Braden Scale for Pressure Ulcer Risk in elderly residents of long-term care facilities. Geriatric Nursing, 31(2), 95-104.
- Cooper, K. L. (2013). Evidence-based prevention of pressure ulcers in the intensive care unit. Critical care nurse, 33(6), 57-66.
- Brienza, D., Kelsey, S., Karg, P., Allegretti, A., Olson, M., Schmeler, M., ... & Holm, M. (2010). A randomized clinical trial on preventing pressure ulcers with wheelchair seat cushions. Journal of the American Geriatrics Society, 58(12), 2308-2314.
- Coleman, S., Gorecki, C., Nelson, E. A., Closs, S. J., Defloor, T., Halfens, R., ... & Nixon, J. (2013). Patient risk factors for pressure ulcer development: systematic review. International journal of nursing studies, 50(7), 974-1003.
- Rich, S. E., Shardell, M., Hawkes, W. G., Margolis, D. J., Amr, S., Miller, R., & Baumgarten, M. (2011). Pressure‐redistributing support surface use and pressure ulcer incidence in elderly hip fracture patients. Journal of the American Geriatrics Society, 59(6), 1052-1059.
- Fossum, M., Alexander, G. L., Ehnfors, M., & Ehrenberg, A. (2011). Effects of a computerized decision support system on pressure ulcers and malnutrition in nursing homes for the elderly. International journal of medical informatics, 80(9), 607-617.
- Demarré, L., Van Lancker, A., Van Hecke, A., Verhaeghe, S., Grypdonck, M., Lemey, J., ... & Beeckman, D. (2015). The cost of prevention and treatment of pressure ulcers: a systematic review. International journal of nursing studies, 52(11), 1754-1774.
- Iizaka, S., Okuwa, M., Sugama, J., & Sanada, H. (2010). The impact of malnutrition and nutrition-related factors on the development and severity of pressure ulcers in older patients receiving home care. Clinical Nutrition, 29(1), 47-53.
- Agrawal, K., & Chauhan, N. (2012). Pressure ulcers: Back to the basics. Indian journal of plastic surgery: official publication of the Association of Plastic Surgeons of India, 45(2), 244.
- Moraes, G. L. D. A., Araújo, T. M. D., Caetano, J. Á., Lopes, M. V. D. O., & Silva, M. J. D. (2012). Evaluation of the risk for pressure ulcers in bedridden elderly at home. Acta Paulista de Enfermagem, 25(SPE1), 7-12.
- Gray, M. (2010). Optimal management of incontinence-associated dermatitis in the elderly. American journal of clinical dermatology, 11(3), 201-210.
- Spector, W. D., Limcangco, R., Williams, C., Rhodes, W., & Hurd, D. (2013). Potentially avoidable hospitalizations for elderly long-stay residents in nursing homes. Medical care, 673-681.
- Hyun, S., Li, X., Vermillion, B., Newton, C., Fall, M., Kaewprag, P., ... & Lenz, E. R. (2014). Body mass index and pressure ulcers: improved predictability of pressure ulcers in intensive care patients. American Journal of Critical Care, 23(6), 494-501.
- Sprigle, S., & Sonenblum, S. (2011). Assessing evidence supporting redistribution of pressure for pressure ulcer prevention: a review. J Rehabil Res Dev, 48(3), 203-13.
- Beeckman, D., Schoonhoven, L., Fletcher, J., Furtado, K., Heyman, H., Paquay, L., ... & Defloor, T. (2010). Pressure ulcers and incontinence-associated dermatitis: effectiveness of the Pressure Ulcer Classification education tool on classification by nurses. Qual Saf Health Care, 19(5), e3-e3.
- Mallah, Z., Nassar, N., & Badr, L. K. (2015). The effectiveness of a pressure ulcer intervention program on the prevalence of hospital acquired pressure ulcers: controlled before and after study. Applied Nursing Research, 28(2), 106-113.
- Cox, J. (2011). Predictors of pressure ulcers in adult critical care patients. American journal of critical care, 20(5), 364-375.
- Van Anholt, R. D., Sobotka, L., Meijer, E. P., Heyman, H., Groen, H. W., Topinkova, E., ... & Schols, J. M. G. A. (2010). Specific nutritional support accelerates pressure ulcer healing and reduces wound care intensity in non-malnourished patients. Nutrition, 26(9), 867-872.
- Prince, M., Bryce, R., Albanese, E., Wimo, A., Ribeiro, W., & Ferri, C. P. (2013). The global prevalence of dementia: a systematic review and metaanalysis. Alzheimer's & dementia, 9(1), 63-75.
- Qi, X., Yang, M., Ren, W., Jia, J., Wang, J., Han, G., & Fan, D. (2013). Find duplicates among the PubMed, EMBASE, and Cochrane Library Databases in systematic review. PLoS One, 8(8), e71838.
- Kitchenham, B., Brereton, O. P., Budgen, D., Turner, M., Bailey, J., & Linkman, S. (2009). Systematic literature reviews in software engineering–a systematic literature review. Information and software technology, 51(1), 7-15.
- Luppino, F. S., de Wit, L. M., Bouvy, P. F., Stijnen, T., Cuijpers, P., Penninx, B. W., & Zitman, F. G. (2010). Overweight, obesity, and depression: a systematic review and meta-analysis of longitudinal studies. Archives of general psychiatry, 67(3), 220-229.
- Vaismoradi, M., Turunen, H., & Bondas, T. (2013). Content analysis and thematic analysis: Implications for conducting a qualitative descriptive study. Nursing & health sciences, 15(3), 398-405.
- Moher, D., Shamseer, L., Clarke, M., Ghersi, D., Liberati, A., Petticrew, M., ... & Stewart, L. A. (2015). Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Systematic reviews, 4(1), 1.
- Coleman, S., Gorecki, C., Nelson, E. A., Closs, S. J., Defloor, T., Halfens, R., ... & Nixon, J. (2013). Patient risk factors for pressure ulcer development: systematic review. International journal of nursing studies, 50(7), 974-1003.
- Dwan, K., Altman, D. G., Arnaiz, J. A., Bloom, J., Chan, A. W., Cronin, E., ... & Ghersi, D. (2008). Systematic review of the empirical evidence of study publication bias and outcome reporting bias. PloS one, 3(8), e3081.
- Dwan, K., Gamble, C., Williamson, P. R., & Kirkham, J. J. (2013). Systematic review of the empirical evidence of study publication bias and outcome reporting bias—an updated review. PloS one, 8(7), e66844.
- Webster, J., Coleman, K., Mudge, A., Marquart, L., Gardner, G., Stankiewicz, M., ... & McClymont, A. (2011). Pressure ulcers: effectiveness of risk-assessment tools. A randomised controlled trial (the ULCER trial). BMJ quality & safety, 20(4), 297-306.
- Litchford, M. D., Dorner, B., & Posthauer, M. E. (2014). Malnutrition as a precursor of pressure ulcers. Advances in wound care, 3(1), 54-63.
- McInnes, E., Jammali‐Blasi, A., Bell‐Syer, S. E., Dumville, J. C., Middleton, V., & Cullum, N. (2015). Support surfaces for pressure ulcer prevention. Cochrane Database of Systematic Reviews, (9).
- Li, Y., Yin, J., Cai, X., Temkin-Greener, H., & Mukamel, D. B. (2011). Association of race and sites of care with pressure ulcers in high-risk nursing home residents. Jama, 306(2), 179-186.
- Park, S. H., Lee, Y. S., & Kwon, Y. M. (2016). Predictive validity of pressure ulcer risk assessment tools for elderly: a meta-analysis. Western Journal of Nursing Research, 38(4), 459-483.
- Clark, M., Black, J., Alves, P., Brindle, C. T., Call, E., Dealey, C., & Santamaria, N. (2014). Systematic review of the use of prophylactic dressings in the prevention of pressure ulcers. International Wound Journal, 11(5), 460-471 Tchanque-Fossuo, C. N., & Kuzon Jr, W. M. (2011). An evidence-based approach to pressure sores. Plastic and reconstructive surgery, 127(2), 932-939.
- Baumgarten, M., Margolis, D. J., Localio, A. R., Kagan, S. H., Lowe, R. A., Kinosian, B., ... & Ruffin, A. (2006). Pressure ulcers among elderly patients early in the hospital stay. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences, 61(7), 749-754.
- Hopkins, A., Dealey, C., Bale, S., Defloor, T., & Worboys, F. (2006). Patient stories of living with a pressure ulcer. Journal of advanced nursing, 56(4), 345-353.
- Linder-Ganz, E., Yarnitzky, G., Yizhar, Z., Siev-Ner, I., & Gefen, A. (2009). Real-time finite element monitoring of sub-dermal tissue stresses in individuals with spinal cord injury: toward prevention of pressure ulcers. Annals of biomedical engineering, 37(2), 387.
- Solis, L. R., Hallihan, D. P., Uwiera, R. R., Thompson, R. B., Pehowich, E. D., & Mushahwar, V. K. (2007). Prevention of pressure-induced deep tissue injury using intermittent electrical stimulation. Journal of Applied Physiology, 102(5), 1992-2001.
- Levine, S. M., Sinno, S., Levine, J. P., & Saadeh, P. B. (2013). Current thoughts for the prevention and treatment of pressure ulcers: using the evidence to determine fact or fiction. Annals of surgery, 257(4), 603-608.
- Gallagher, P., Barry, P., Hartigan, I., McCluskey, P., O'Connor, K., & O'Connor, M. (2008). Prevalence of pressure ulcers in three university teaching hospitals in Ireland. Journal of tissue viability, 17(4), 103-109.
- Papanikolaou, P., Lyne, P., & Anthony, D. (2007). Risk assessment scales for pressure ulcers: a methodological review. International journal of nursing studies, 44(2), 285-296.
- Yip, M., Da He, D., Winokur, E., Balderrama, A. G., Sheridan, R., & Ma, H. (2009, September). A flexible pressure monitoring system for pressure ulcer prevention. In 2009 Annual International Conference of the IEEE Engineering in Medicine and Biology Society (pp. 1212-1215). IEEE.
- Sewchuk, D., Padula, C., & Osborne, E. (2006). Prevention and early detection of pressure ulcers in patients undergoing cardiac surgery. AORN journal, 84(1), 75-96.
- Gehin, C., Brusseau, E., Meffre, R., Schmitt, P. M., Deprez, J. F., & Dittmar, A. (2006, June). Which techniques to improve the early detection and prevention of pressure ulcers?. In 2006 International Conference of the IEEE Engineering in Medicine and Biology Society (pp. 6057-6060). IEEE.
- Schoonhoven, L., Grobbee, D. E., Donders, A. R. T., Algra, A., Grypdonck, M. H., Bousema, M. T., ... & Buskens, E. (2006). Prediction of pressure ulcer development in hospitalized patients: a tool for risk assessment. BMJ Quality & Safety, 15(1), 65-70.
- Terekeci, H., Kucukardali, Y., Top, C., Onem, Y., Celik, S., & Öktenli, Ç. (2009). Risk assessment study of the pressure ulcers in intensive care unit patients. European Journal of Internal Medicine, 20(4), 394-397.
- Dealey, C., & Lindholm, C. (2006). Pressure ulcer classification. In Science and practice of pressure ulcer management (pp. 37-41). Springer, London.
- Moher, D., Shamseer, L., Clarke, M., Ghersi, D., Liberati, A., Petticrew, M., ... & Stewart, L. A. (2015). Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Systematic reviews, 4(1), 1.
- Shamseer, L., Moher, D., Clarke, M., Ghersi, D., Liberati, A., Petticrew, M., ... & Stewart, L. A. (2015). Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. Bmj, 349, g7647.
- Whiting, P. F., Wolff, R. F., Deshpande, S., Di Nisio, M., Duffy, S., Hernandez, A. V., ... & Schmidlkofer, S. (2015). Cannabinoids for medical use: a systematic review and meta-analysis. Jama, 313(24), 2456-2473.
- Kaufman, B. G., Spivack, B. S., Stearns, S. C., Song, P. H., & O’Brien, E. C. (2019). Impact of accountable care organizations on utilization, care, and outcomes: a systematic review. Medical Care Research and Review, 76(3), 255-290.
- Chan, J., Griffith, L. E., Costa, A. P., Leyenaar, M. S., & Agarwal, G. (2019). Community paramedicine: A systematic review of program descriptions and training. Canadian Journal of Emergency Medicine, 1-13.



- 24/7 Customer Support
- 100% Customer Satisfaction
- No Privacy Violation
- Quick Services
- Subject Experts