Effect of Arc Length and Intraocular Pressure on Corneal Radius of Curvature
Computing the change in refractive power is exceptionally gainful, in light of the fact that it will empower us to examine what influences the refractive power of the cornea, with regards to the mechanical properties of the implants. The code likewise delivers the precarious and level meridian edges this is significant data to know for the parametric examination just as for the future information base for other parametric investigations. For students seeking biomedical science dissertation help, getting familiar with all these intricate calculations and their implications. It is said to be crucial for advance research in the field.
Three examinations were led which measured the change in radius of curvature with Arch based on changing IOP values (17.5 mmHg, 20 mmHg, 27.5 mmHg, 30 mmHg, 37.5 mmHg and 40 mmHg), changing values of Thickness (150, 200, 250), changing diameter (5 mm and 6mm) and changing Modulus of Elasticity E (0.2, 0.6, 1). Inside those examination various segments where differed to represent the adjustment in relationship of each investigation. Based on the findings, the deformations of cornea while actualizing the implant were anticipated.

Arc Length Over Radius of Curvature
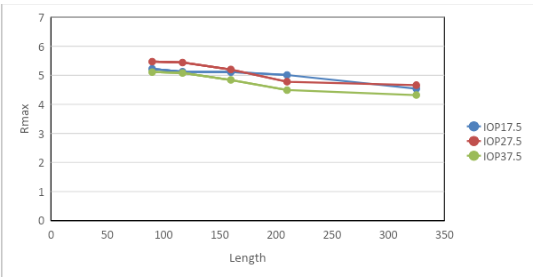
1. Effect of arc length over maximum radius of curvature (Rmax) with changing values of Intra Ocular Pressure (IOP) (mmHg):
Changing Intra Ocular Pressure (IOP) (mmHg)
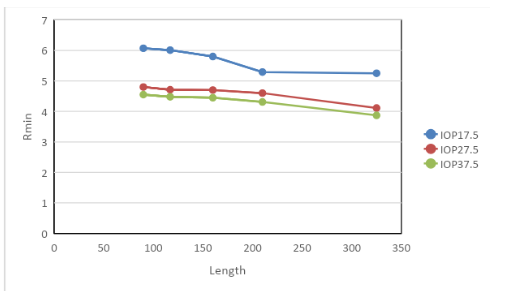
IOP (intraocular pressure) assumes a significant job in the investigation, when the corneal inserts were tried to gauge the pressure they could retain just as the refractive power of the eye. In this way IOP could have an immediate relationship to the size of a refractive error. This stems from a perceptions that that IOP value is higher among nearsighted subjects contrasted with Emmetropes and Hypermetropes .Due to this hypothesis an investigation was done test the its legitimacy. The investigation demonstrates there is an immediate connection among's IOP and refractive errors. It has been observed that when the IOP values were kept in between 17.5 mm Hg, 27.5 mm Hg and 37.5 mm Hg, whereas the CCT (Central Corneal Thickness), E (Modulus of Elasticity), diameter and R values are kept constant at 595mm, 0.2 Mpa, 5mm and 7.8mm respectively the highest non linear decreasing trend had been observed with IOP 37.5 mm Hg. There is a gap between IOP 27.5 mm Hg and 37.5mm Hg all throughout the curve length of Rmax but in case of Rmin the gap between IOP 17.5 mm Hg and 37.5 mm Hg was large. It was also observed that with the increasing arc length the maximum radius of curvature was constantly decreasing for IOP 27.5 mm Hg and 37.5 mmHg but the trend was not similar for IOP 17.5 mm Hg. In case of Rmin all the three curves showed a decreasing trend with increasing arc length (Refer Fig: 1 and 3).
Looking for further insights on The Psychological Effects of Urinary Incontinence and Bedwetting in Children? Click here.
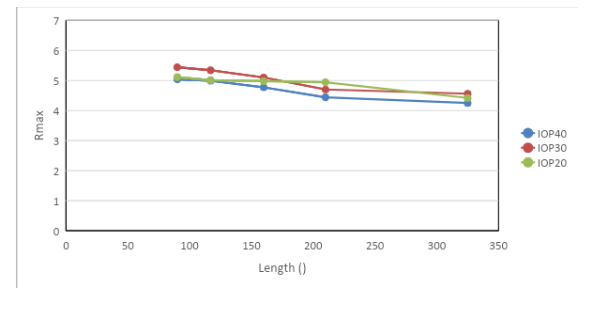
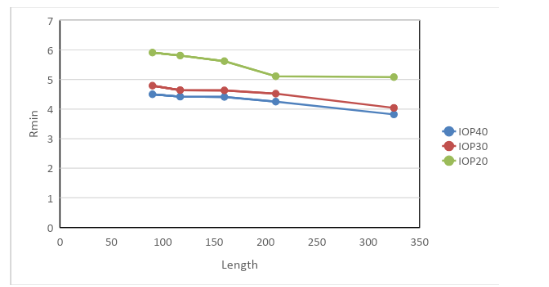
Similarly for IOP values 20 mm Hg, 30 mm Hg and 40 mm Hg the non linear smooth decreasing trend was observed with IOP 40 mm Hg which denotes that IOP 37.5 mm Hg and 40 mm Hg have significant impact upon the radius of curvature. The other IOP values did not demonstrated a decreasing or increasing significant pattern in comparison with IOP 37.5 mm Hg and 40 mm Hg. The gap observed between IOP 30 mm Hg and 40 mm Hg in Rmax was constant all throughout the curve but in case of Rmin the gap between IOP 20 mm Hg and 40 mm Hg was large. Here also IOP 30 40mm Hg and 40mm Hg showed a decreasing trend with the increasing arc length but the curve pattern was different for IOP 20 mmHg for Rmax but for Rmin all the curves showed a decreasing pattern (Refer Fig: 2 and 4).
The graph given below demonstrates the impact of arc length on the corneal change of the radius of curvature with different IOP values (17.5 mmHg, 20 mmHg, 27.5 mmHg, 30 mmHg, 37.5 mmHg and 40 mmHg) whereas the CCT (Central Corneal Thickness), E (Modulus of Elasticity), diameter and R values are kept constant at 595 mm, 0.2 Mpa, 5 mm and 7.8 mm respectively.
2. Effect of arc length over minimum radius of curvature (Rmin) with changing values of Intra Ocular Pressure (IOP) (mmHg):
3. Effect of arc length over maximum radius of curvature (Rmax) with changing values of E (Modulus of Elasticity) at 0.2, 0.6 and 1Mpa:
Changing E (Modulus of Elasticity)
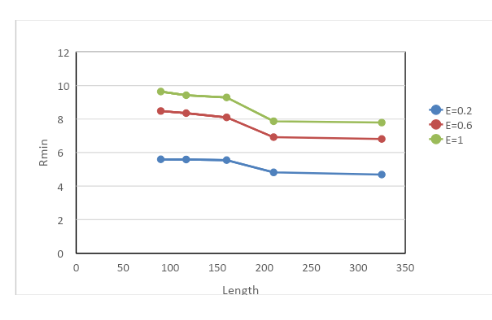
For changing values of E at 0.2 Mpa, 0.6 Mpa, 1 Mpa the impact of arc length on the corneal change of the radius of curvature with the CCT (Central Corneal Thickness), Intra Ocular Pressure (IOP), diameter, thickness and R values kept constant at 595 mm, 30 mm Hg, 5 mm, 250 and 7.8 mm respectively it was observed that a sharp decrease was observed in Rmax with E = 0.6 Mpa and 1 Mpa whereas 0.2 Mpa maintained a more or less linear trend. For Rmin it was found that E values 0.6 Mpa and 1 Mpa showed a smooth non linear decreasing trend. The curve of E = 0.2 Mpa had a significant gap in between with the curves of E = 0.6 Mpa and E = 1 Mpa in case of Rmax and this gap was consistent in case of Rmin also. However, all the curves showed a decreasing trend with respect to increasing arc length for both Rmax and Rmin (Refer Fig: 5 and 6).
The thickness of implant was fluctuated to get its actuated impact on curvature; this examination was differed over a scope of E. The watched general linear trend pattern was that the induced curvature and flow would be higher for decreased young’s modulus of cornea because of a diminished protection from deformation. This was found in the examinations; anyway the consistency to which the patterns were isolated differed. Figures 5 and 6 demonstrated that the incited change in shape in diminishing for diminishing CCT. It tends to be seen that for little change in CCT, R and E inserts greatly affected the initiated change in curvature; all inserts had a flattened impact on the cornea.
The graphs given below demonstrates the impact of arc length on the corneal change of the radius of curvature with different values of E (Modulus of Elasticity) whereas the CCT (Central Corneal Thickness), Intra Ocular Pressure (IOP), diameter, thickness and R values constant at 595 mm, 30 mm Hg, 5 mm, 250 mm and 7.8 mm respectively.

4. Effect of arc length over minimum radius of curvature (Rmin) with changing values of E (Modulus of Elasticity) at 0.2 Mpa, 0.6 Mpa and 1 Mpa:
5. Effect of arc length over maximum radius of curvature (Rmax) with values of E (Modulus of Elasticity) at 1Mpa and changing values of Diameter 6mm:
Change in Diameter (5mm and 6mm)
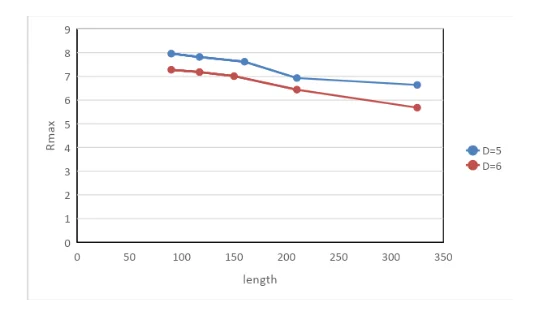
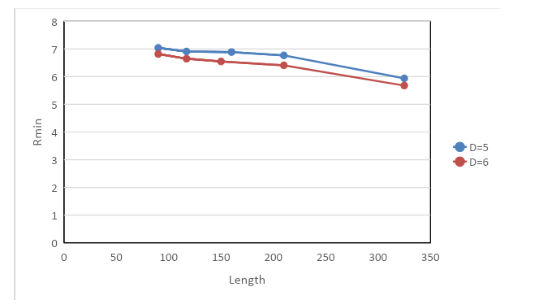
When leading an investigation of the impact of diameter on the difference in radius of curvature flow, it has been discovered that the difference in radius of curvature diminishes as the Arch length increments. Which implies, for a bigger implant diameter across, a littler change on the radius of curvature will happen after the cornea has twisted. It was noted that the impact of arc length on the corneal change of the radius of curvature values of E (Modulus of Elasticity) at 1 Mpa only and a change in diameter from 5 mm to 6mm and the CCT (Central Corneal Thickness), Intra Ocular Pressure (IOP), thickness and R values constant at 595 mm, 30 mm Hg, 150mm and 7.8 mm respectively demonstrated that D = 6 mm showed a smooth non linear decreasing trend in comparison to D = 5 mm with respect to both Rmax and Rmin. The gap observed between the curve D = 5 mm and D = 6 mm was narrow in both Rmax and Rmin but in both cases the two curves showed a decreasing trend with increasing arc length. As it is plainly delineated in all figures, a diminishing pattern has happened in all charts for al lines demonstrating the connection between the adjustment in change in the radius of curvature and implant length across. Moreover, the lines are framing an inward bend shape. No distinctive change in behaviour happened in the graphs (Refer Fig: 7 and 8).
The graphs given below demonstrates the impact of arc length on the corneal change of the radius of curvature with different values of diameter of 5 mm and 6 mm whereas the CCT (Central Corneal Thickness), Intra Ocular Pressure (IOP), E value, thickness and R values constant at 595 mm, 30 mm Hg, 1 Mpa, 150 mm and 7.8 mm respectively.
6. Effect of arc length over minimum radius of curvature (Rmin) with changing values of E (Modulus of Elasticity) at 0.2 Mpa, 0.6 Mpa and 1 Mpa and Diameter of 5mm and 6mm:
7. Effect of arc length over maximum radius of curvature (Rmax) with changing values of T (Thickness) at 150mm, 200mm, 250mm; Diameter 5mm; E (Modulus of Elasticity) at 0.2 Mpa, 0.6 Mpa, 1Mpa:
Change in Thickness with Changing E (Modulus of Elasticity)
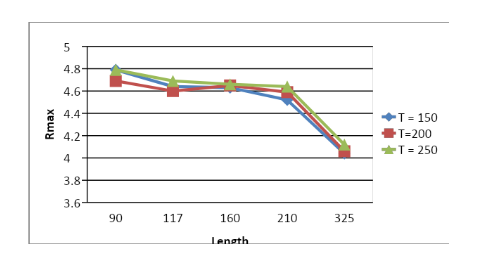
The graphs given below demonstrates the impact of arc length on the corneal change of the radius of curvature with different values of T (Thickness) whereas the CCT (Central Corneal Thickness), Intra Ocular Pressure (IOP), diameter, E (Modulus of Elasticity)and R values constant at 595 mm, 30 mm Hg, 5 mm, 0.2 Mpa and 7.8 mm respectively.
The combinations: Thickness = 150 mm; E = 0.2 Mpa; Diameter = 5 mm; Thickness = 200 mm; E = 0.2 Mpa; Diameter = 5 mm; Thickness = 250 mm; E = 0.2 Mpa; Diameter = 5 mm
8. Effect of arc length over minimum radius of curvature (Rmin) with changing values of T (Thickness) at 150 mm, 200 mm, 250 mm; Diameter 5mm and 6mm; E (Modulus of Elasticity) at 0.2 Mpa, 0.6 Mpa, 1 Mpa:
The combinations: Thickness = 150 mm, 200 mm, 250 mm; E = 0.2 Mpa; Diameter = 5 mm
The combinations: Thickness = 150 mm, 200 mm, 250 mm; E = 0.6 Mpa; Diameter = 5 mm
The combinations: Thickness = 150 mm, 200 mm, 250 mm; E = 1 Mpa; Diameter = 5 mm
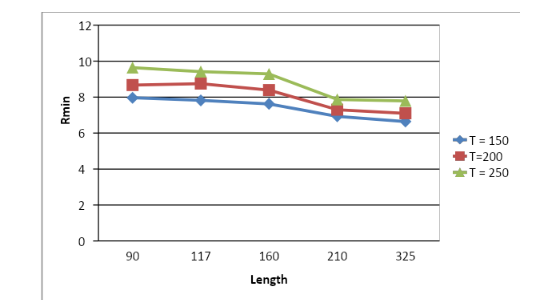
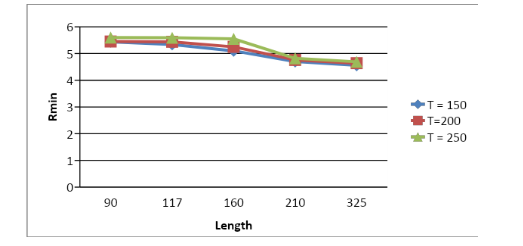
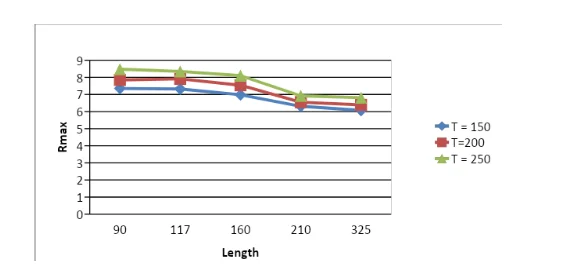
The diagrams above demonstrates the impact of arc length on the corneal change of the radius of curvature with different values of T (Thickness) such as 150 mm, 200 mm, 250 mm along with changing values of E at three different values 0.2 Mpa, 0.6 Mpa and 1 Mpa whereas the CCT (Central Corneal Thickness), Intra Ocular Pressure (IOP), diameter and R values are kept constant at 595 mm, 30 mm Hg, 5mm and 7.8 mm respectively. It was observed that by keeping the value of E constant at 0.2 Mpa and diameter 5mm initially the thickness varying in between 150 mm, 200 mm, 250 mm values there was a sharp decreasing trend of the graph in all three cases at Rmax. But when the graph of Rmin was studied the significant decreasing trend was observed for T = 250 mm. All the curves showed a steep decreasing trend with increasing arc length and no gap in between the curves were observed for Rmax and for Rmin the trend was similar but not that sharp with no gap in between the curves (Refer Fig: 9 and 10).
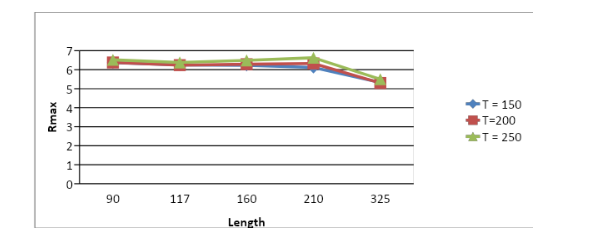
In the second case when E value was kept constant at 0.6 Mpa and diameter at 5mm with varying thickness of 150 mm, 200 mm and 250 mm it was observed that T = 250 showed sharp decreasing trend in comparison to the other two with respect to Rmax and for Rmin all the three chosen values of thickness represented a smooth decreasing non linear trend. For Rmax the curves showed no gaps in between and the decreasing trend with increasing arc length was not that sharp but for Rmin the curves exhibited gaps in between and the steep down was smooth in all the cases (Refer Fig: 11 and 12).
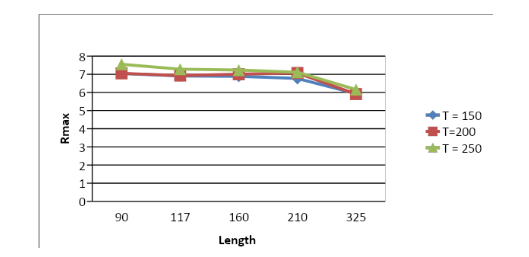
In the third case where the value of E was kept constant at 1 Mpa and diameter at 5mm the three different values of T 150 mm, 200 mm and 250 mm demonstrated that all the three graphs showed similar trend with respect to Rmax but in Rmin better trend was observed for T = 200 mm and 250 mm. Similarly, for Rmax the curves showed no gaps in between and the decreasing trend with increasing arc length was not that sharp but for Rmin the curves exhibited gaps in between and the steep down was smooth in all the cases (Refer Fig: 13 and 14). When directing an investigation of the impact of thickness on the difference in range of radius of curvature, it has been discovered that the difference in radius of curvature increments as the Arch length increments. Which implies, for a bigger implant thickness, a littler change on the range of radius of curvature will happen after the cornea has disfigured. The thickness of implant was fluctuated to get its actuated impact on curvature; this examination was differed over a scope of E. The watched general linear trend pattern was that the induced curvature and flow would be higher for decreased young’s modulus of cornea because of a diminished protection from deformation. This was found in the examinations; anyway the consistency to which the patterns were isolated differed.
Discussion
As found in the figures introduced in the predecessor, segment Keraring intrastromal corneal ring portions directly affect changing the shape of the cornea by instigating curvature shape because of the implants being stiffer than in vivo tissue. It would then be able to be surmised that the adjustment in overall shape that would associate to improved visual keenness. As talked about in the literature review and background study portion this is accomplished by changing where the refracted light assemble into, suitably in the retina. A great part of the writing has fretted about considering the impacts and viability of refractive medical procedures, in any case despite the fact that ICRS gives an increasingly effective other option, an absence of comprehension forestalls its pervasiveness. This examination intends to fill this stipulation by leading a numerical parametric investigation to decide how the implants perform inside various recreated in vivo circumstances. This means to encourage the objective of making an arranging apparatus that would permit clinicians to settle on educated choices, the same number of decisions with regards to which measurement ring is to be utilized is based off experience instead of quantitative techniques. Because of a wide scope of eye parameters, a parametric report has been led. That is to convey the most productive arrangement of results which can convey the point of the task. Each gathering up-and-comer was set to rehearse an alternate arrangement of results. In any case, some had comparable parameters to work with. There were various sorts of parametric investigations included for the undertaking which are: effect of curve length on the difference in radius of curvature, effect of width on the difference in range of radius of curvature, effect of thickness on the difference radius of curvature.
The parameters are partitioned into two sorts such as:
Corneal parameters: which include Curvature, E (Modulus of Elasticity), CCT (Central Corneal Thickness) and IOP (Intra Ocular Pressure).
Implant parameters: The implant parameters include the thickness, diameter/ width and length.
So as to have look at a wide scope of embed and corneal parameters utilizing numerical models strategy, a parametric report has been finished. The parametric examination assisted with looking at the impact of each change in parameter on the usage procedure.
Three examinations were led which measured the change in radius of curvature with Arch based on changing IOP values (17.5 mmHg, 20 mmHg, 27.5 mmHg, 30 mmHg, 37.5 mmHg and 40 mmHg), changing values of Thickness (150, 200, 250), changing diameter (5 mm and 6mm) and changing Modulus of Elasticity E (0.2, 0.6, 1). Inside those examination various segments where differed to represent the adjustment in relationship of each investigation. Based on the findings, the deformations of cornea while actualizing the implant were anticipated.

When leading an investigation of the impact of diameter on the difference in radius of curvature, it has been discovered that the difference in radius of curvature diminishes as the Arch length increments. The graphical figures imply that for a bigger arc length of implant, a littler change on the radius of curvature will happen after the cornea has twisted. This means, a bigger measure of distortion happens after the deformation of cornea. When figuring changed implant thickness, a comparable change in behaviour of cornea was observed as an impact upon breadth. Furthermore, fluctuation in the E parameter for a fixed value of R and CCT parameters bring about an expansion of the adjustment in the radius of curvature. The finding implies that the elasticity of the cornea develops with the increment of the radius of curvature. Besides, rates between two corneas with various E parameters bring about a diminishing nature with expanding R values. Shifting R value for a particular CCT value brought about an increase or decrease in the change of radius of curvature based upon the values of CCT. Nevertheless, distinctive implant thickness brings about various corneal dimensions with the impact of curve length. With fluctuating R, it is difficult to anticipate the behavioural patterns of the cornea. That is a direct result of the extension or lessening in change of radius of curvature range. In any case, for all assortments related with effect of estimation study, the relationship happened to be lessening non-direct which a bended shape. Notwithstanding, for all varieties related with impact of measurement study, the relationship happened to be diminishing non-directly with the inward shape. When directing an investigation of the impact of thickness on the difference in range of radius of curvature, it has been discovered that the difference in radius of curvature increments as the Arch length increments. Which implies, for a bigger implant thickness, a littler change on the range of radius of curvature will happen after the cornea has disfigured. The thickness of implant was fluctuated to get its actuated impact on curvature; this examination was differed over a scope of E. The watched general linear trend pattern was that the induced curvature and flow would be higher for decreased young’s modulus of cornea because of a diminished protection from deformation. This was found in the examinations; anyway the consistency to which the patterns were isolated differed. The thickness of implant was shifted to acquire its incited impact on radius of curvature; this investigation was differed over a scope of R. It was normal that smaller radii would have bigger initiated changes in radius of curvature because of the geometry. Having higher preoperative change in radius of curvature and this change happened would be amplified or decreased by CCT and curve length. In any case, model dependability was restricting component right now getting reliable outcomes was testing. Results can be seen to uncertainly take after the normal non-straight pattern; be that as it may, more outcomes are expected to increase any connection between the two. IOP (intraocular pressure) assumes a significant job in the investigation, when the corneal inserts were tried to gauge the pressure they could retain just as the refractive power of the eye. In this way IOP could have an immediate relationship to the size of a refractive error. This stems from a perception that that IOP value is higher among nearsighted subjects contrasted with Emmetropes and Hypermetropes. Due to this hypothesis an investigation was done test the legitimacy. The investigation demonstrates there is an immediate connection among's IOP and refractive errors. It has been observed that when the IOP values were kept in between 17.5 mm Hg, 27.5 mm Hg and 37.5 mm Hg, whereas the CCT (Central Corneal Thickness), E (Modulus of Elasticity), diameter and R values are kept constant at 595mm, 0.2 Mpa, 5mm and 7.8mm respectively the highest non linear decreasing trend had been observed with IOP 37.5 mm Hg. Similarly for IOP values 20 mm Hg, 30 mm Hg and 40 mm Hg the non linear smooth decreasing trend was observed with IOP 40 mm Hg which denotes that IOP 37.5 mm Hg and 40 mm Hg have significant impact upon the radius of curvature. The other IOP values did not demonstrated a decreasing or increasing significant pattern in comparison with IOP 37.5 mm Hg and 40 mm Hg. Anyway when contrasting the impact of every parameter on the refractive force, figures show that the inward width largely affects the refractive force contrasted with the internal width. This is perhaps because of the way that, the internal width changes first making a bump in the cornea structure, the external width acts the equivalent. However this impact on the cornea is coming in type of a response to the difference in the internal width, despite everything has comparative behavioural impact on the cornea yet contrasted with the inward width, the internal width has an increasingly huge impact on the refractive power contrasted with external width. The initial radius of the cornea imparts a similitude to the external width that is its impact on the refractive power is infinitesimal contrasted with the internal width as appeared in the outcome area above. The expansion of the inserts to handle Myopia highlighted the overall curvature of the eye. Inserts safeguard the shape of the eye because of the nearsighted impact on the eye, while few inserts will extend the curvature and stream just on the territories at which they are set. So at 0 degrees and 180 degrees, the inserts will bring about the formation of curvatures all around the cornea and this helps when the structures in the eye don't adequately focus the light that enters the eye onto the retina, which handles the Astigmatic impact on the eye. When the inserts are completely set up and unblemished it makes the fringe cornea become more extreme and the focal cornea to smooth, which handles Myopia by moving where the light is centred around to the retina. The consequences of the implants all have one regular angle; this is because of progress in shape in the structure of the eye, which will influence the general refractive intensity of the eye. The inward width hopes to frame a negative connection with regards to the inserts. Additionally to the inserts graphs the external width has comparative impact on the refractive power as the inward width, for the situation as the external width expands the refractive power diminishes. On the off chance that the external and the internal width must be analyzed, it shows that the inward width largely affects the refractive power contrasted with the external width, the refractive force diminishes more as the internal width increments, also similarly as with the two implants the change between the parameters is exceptionally miniscule. This was a comparable case in all the outcomes by different understudies that embraced the parametric examination. No doubt the initial radius is the prevailing parameter with regards with its impact on the refractive intensity of the cornea. The inward width estimation appeared to have the most impact on the refractive intensity of the eye, which is inverse to the implant diagrams this is because of the distinction among Astigmatism and Myopia, because of utilizing the implants on the model the internal width value can be little so it permits the eye to bend less which can help to handle the impact of nearsightedness, when the cornea bends excessively. Based on the findings it can be inferred that the CCT worth can be considered the parameter with minimal impact on the refractive intensity of the cornea. The graph likewise demonstrated a contrary outcome, as the effective inward width value is reasonable on the grounds that with it's the least values also so the eye doesn't bend excessively, which permits the cornea and the lens to worth in symphonies movement to centre the light beams before the retina rather than on the retina. The littlest dimension of the inward width additionally shows the more prominent dioptre change between all the estimations of the internal width which is on the grounds that it causes less deformation in the eye model which cause greater dependability in the eye model ,thus expanding its refractive power value. As appeared in several figures there are a couple of inconsistencies in the outcomes, practically all the understudies who embraced the parametric examination have experienced similar impacts testing this particular mix of parameters. This all stems from the constrained segment illustrate, as the position where the inserts and the cornea reach may not been sketched out adequately or clearly perceived by Abaqus, which probably made the sporadic results, as appeared in the diagrams. The pocket for the inserts is made first (step1) at that point the inserts are embedded into the pockets (step2). The initial contact can likewise be one reason why there are a few inconsistencies in the outcomes; this might be because of the contact simulation. This may be the genuine reasons on the grounds that the charts introduced in the segment above have sensible patterns separated from the diagrams that include the contact reproduction, which cause enormous deformations resulting in failures in the intermingling of numerical qualities. Anyway the real purpose for the issue is obscure; it will require future work to take a look at the issue. Catching a particular behaviour of the cornea was impractical because of the irregular patterns of certain outcomes. Incorrectness happened in the outcomes gathered which oblige to appraise a general pattern and disregarded those out outcome which break specific patterns. Limitations of the study included - stiffness of the cornea was considered to consistent for all examinations directed; the cornea was analyzed with 6 visual fragments and 2 visual layers; rings shaped in the model were just in the cornea which was just 50 rings; it has been taken in thought to just inspect corneas with flexible properties; stress free conduct was considered for all models to identify with the genuine eye parameters.
Continue your journey with our comprehensive guide to Diagnostic Medical Ultrasound.



- 24/7 Customer Support
- 100% Customer Satisfaction
- No Privacy Violation
- Quick Services
- Subject Experts