Understanding Coxa Saltans in Athletes
Chapter 1
1.0 Introduction
Injuries associated with pelvis and hips represent at least 5% or 6% of athletic injuries experienced by adults. According to Boyd et al (1997), the athletes who most commonly experience this type of injury are runners, soccer players and dancers. There is a paucity of reports on the prevalence of Coxa Saltans compared to other hip disorders, particularly because it is considered a less-common type of hip injury (white et al, 2004). Generally, Coxa Saltans is a term that describes a palpable and or audible snap on the hip that sometimes presents with pain. The snapping, painful hip usually presents a diagnostic dilemma to many health practitioners due to the many etiologies associated with it. Consequently, the success of any treatment intervention depends on the practitioner’s understanding of what precisely causes it. The many potential etiologists for this condition can be placed within three major categories namely: internal causes, external causes and intraocular causes (White et al, 2004, Bellabarba et al 1998, Idjadi & Meislin 2004, Wahl et al 2004). Nonetheless, the pathology of iliopsoas tendon is most often considered as the source of internal hip snapping. Ideally, snapping often occurs when iliopsoas tendon snaps over the inner structure such as femoral head, lesser trochanter, and iliopectineal eminence (Wahl et al 2004). Schaberg (1984) also suggested that the snapping could be as a result of the movement of iliofemoral ligaments over the anterior hip capsule. On the other hand, intraocular snapping occurs as a result labral tears, synovial chondromatosis, and idiopathic hip instability (White et al, 2004, Bellabarba et al 1998, Idjadi & Meislin 2004, Wahl et al 2004). However, the most common of the three categories is external hip snapping, which involves various structures external to the hip joint (Provencher et al, 2004). When an athlete experiences an external hip snapping, the possibilities are that there could be a snapping of the proximal hamstring tendon over the ischial tuberosity, or more possibly, there could be a snapping of iliotibial band, gluteus maximus, fascia latae, or a combination of the abovementioned, over the greater trochanter (Wahl et al 2004, Brignall et al 1993, Larsen et al 1986, Waters et al, 1988). The variable causes and low prevalence of Coxa Saltans can lead to difficulties in identifying appropriate treatment plans (White et al, 2004). As such, several studies suggest that practitioners should first attempt non-operative treatment interventions. These conservatory treatments include avoiding any movements that are provocative to the snapping, use of oral nonsteroidal anti-inflammatory medication, stretching, and trochanteric bursa injections (White et al, 2004, Idjadi & Meislin 2004, Provencher et al, 2004). However, there is still a dearth of literature evidence regarding the most appropriate conservative treatment plan or the most effective intervention.
The focus of this study will be the delivery of a 4-week static stretching programme on external snapping hip syndrome (ESHS), which is the most common cause of a painful snapping hip, often associated with a characteristic noise, due to the flipping of the iliotibial band (ITB), a thickened band of tissue that runs down the length of the thigh over the greater trochanter, which is a bony prominence on the anterolateral surface of the proximal shaft of the femur, distal to the femoral neck. It serves as the insertion site for the gluteus maximus and gluteus minimus. Dancers and athletes with tight hip flexors and unbalanced strength in their pelvic, hip, and abdominal muscles are more prone to this condition, which can be brought on by spasmodic or jerky movement of the ITB overlying the greater trochanter, and spasmodic movement of the gluteus maximus muscle during hip motion. Iliopsoas tendonitis is characterized by pain and clicking or snapping in the groin or front of the hip. As the iliopsoas muscle acts as a hip flexor, symptoms are often worse when bending the hip, especially against resistance. The iliopsoas tendon is close to the skin and is a combination of two muscles, the iliacus; a flat, triangular muscle, and the psoas: a long spindle-shaped muscle. These muscles connect to form one single tendon commonly referred to as the iliopsoas or hip flexors, and separate in the abdomen, merging in the thigh. Owing to the considerable number of possible lower-body injuries, this study was restricted to treating amateur dancers with no known other lower limb injuries, concentrating on individuals suffering from coxa saltan, specifically external snappy hip syndrome (ESHS) around the tensor fascia latae (TFL), a fusiform muscle; muscle belly fibres arranged parallel to each other, located in the lateral aspect of the thigh. As discussed by Besomi, Maclachlan, Mellor, Vicenzino & Hodges (2020) and Trammell & Pilson (2018). Using static stretching exercises and measuring the outcome via the Hip dysfunction and Osteoarthritis Outcome Score (HOOS), will provide a clinical impression in the diagnosis of pathologies in the hip, lumbar and sacroiliac region. Many dancers suffer from ESHS; hence the logical hypothesis of this study examines whether a concentrated 4-week period of static stretching is an effective treatment for ESHS. This study focused on treating ESHS using a variety of applicable static stretching techniques covering the mechanism, aetiology, diagnosis, and treatments, using non-invasive static stretching, as opposed to soft tissue release (STR) and surgical intervention techniques as deliberated by Yen, Lewis & Kim (2015).

The literary review highlighted the treatment of all forms of coxa saltan has tended to focus on surgical intervention, with a recognizable gap in academic research concerning early injury awareness and preventative treatments in the form of static stretching. This research will be important for future clinicians using static stretching for this pathology to gauge its short-term effectiveness. Online research identifies lots of informal studies and blog posts on static stretching, but minimal formally approved research. The mechanism of SHS involves many factors and components. Although external and internal SHS share some clinical features, there are many different etiologies or causes. In most cases, non-invasive treatments, such as static stretching or soft tissue treatment (STR), can provide good results if SHS is diagnosed early (Spina, 2007). Static stretching studies have occurred on various anatomies, including patients with SHS, Sharda, Vaghela, Alshryda & Shaheen. (2011) and Bordoni & Varacallo (2020), who advocated muscle strengthening in the presence of weakened muscle areas within the psoas major muscle and all muscles participating in the movement of the hip, lower limb, and lumbar region. Bordoni & Varacallo (2020) believed exercising in front of a mirror to improve the quality of neuromotor intervention, and that it worked well to improve motor function. Lebert (2020), Prejbeanu, Predescu, Haragus & Mioc, (2020), Sirico Palermi, Massa & Corrado (2020), Olafsen & Simpson (2020) reiterated the need for a correct diagnosis and management of SHS, as echoed by Lee & Nam (2020). This study will look at the effectiveness of treating amateur dancers who present with a clinical impression of ESHS using static stretching exercises over an intensive 4-week program. The hypothesis being, that treatment will produce beneficial results, measurable utilizing the Hip dysfunction and Osteoarthritis Outcome Score (HOOS), as opposed to the FABER or Thomas tests, as Laskowski, Johnson, Shelerud, Lee, Rabatin, Driscoll & Terzic (2020, August), owing to Covid-19 restrictions. However, Laskowski et al., (2020) deliberated utilizing modern telecommunication technology to exchange medical information and provide clinical care to individuals at a distance were achievable; as current Covid-19 restrictions, HOOS enables one to measure progress if the clinician physically cannot meet with the patient. Kjeldsen, Reimer, Drejer, Hvid, Mechlenburg & Dalgas (2020), advised that where adduction with circumduction of the affected hip is done online to test for ESHS and the snap or pop over the proximal and lateral side of the femur called the greater trochanter, can be a positive sign. A version of the Faber test, as Bagwell, Bauer, Gradoz & Grindstaff (2016) considered, can be used to differentiate between internal (iliopsoas) or external (ITB) generating the snapping or popping hip inclusive of range of motion (ROM), which is a measurement of combined hip ROM.
Discussion exists with reference to whether limited ROM with this measurement may be symptomatic of hip pathology. ROM is examined in detail by Harris, Mather, Nho, Salvo, Stubbs, Van Thiel & Kivlan (2020), Mosler, Kemp, King, Lawrenson, Semciw, Freke & Ageberg (2020) and Kjeldsen, Reimer, Drejer, Hvid, G., Mechlenburg & Dalgas (2020). On completion of the 4-week treatment period, patients are expected to start to regain normal function of the hip drastically reducing the snap and often associated pain, which with continued self-help treatment over a period of 6 to 12 months, including advise on modifying their movement patterns and continuing their stretching programs, will prevent or reduce the snapping recurrence. Conservative treatment via static stretching, as advocated by Yen, Lewis & Kim (2015) should be attempted first with physical therapy evaluation focussing on the identification of the source of the muscle tightness is causing the snapping.
1.2 The Research Aim
The aim of the study is to investigate the effectiveness of the conservative treatment of coxa saltan on ESHS, utilising static stretches on dancers presenting with clinical impressions of coxa saltan.
1.3 Research Question
Will amateur dancers aged 18-26 years, presenting with clinical impressions of external snapping hip syndrome (coxa saltan), benefit from static stretches over a 4-week duration?
Chapter 2
2.0 Literature rereview
According to Yen, Lewis, & Kim, (2015), Coxa Saltans, otherwise known as snapping hip, is a condition that occurs when the hip flexors undergo sharp contraction, leading to an auditory snapping. The hip movement is often accompanied by pain as some critical muscles and tendons are translocated. Basically, Yen, Lewis, & Kim, (2015) observed that for snapping to occur, the iliotibial band and the iliopsoas tendon must be involved. Whereas the lateral impact involves the iliotibial band, the anterior movement takes place via the iliopsoas tendon. When the hip flexors contract, the type of sound produced can be used to detect the presence of coxa saltans. During hip movement, the impact of tendon translation can be detected through ultrasound as a diagnostic technique. Bordoni, & Varacallo, (2020) confirmed that there are three main causes of coxa saltans. The first cause associated with extra-articular can be either external or internal snapping, and the third cause can be intra-articular. In similar studies, Bordoni, & Varacallo, (2020) observed that most patients experience external extra-articular snapping. It is the condition whereby the snap is caused by the movement of either posterior iliotibial band or the anterior portions of the gluteus maximus. As the movement takes place, the bands can cover the entire trochanter, consequently leading to the extension of the hip, in a process known as the internal or external rotation. In the perspectives of Lebert, (2020), snapping can occur when the posterior iliotibial band or anterior aspects of the gluteus maximus tendons under the tensile movements, and in the process causes the victim to experience sensation and inflammation. As the pain advances, the trochanteric syndrome manifest in bursitis and strains, causing the hip to experience a catching sensation or give away. Sometimes, it is possible for the snapping to occur without the feeling of pain, especially when the strain does not involve critical internal hip flexion muscles.
Internally, Bordoni, & Varacallo, (2020) attribute the process of snapping to the movement of iliopsoas tendon over the iliopectineal protrusion of the pelvis. As a critical part of the hip region, the pelvis usually consists of muscles that rely on a determinate mechanism of movement to be able to prevent strain or tension that can result in abrupt pain. One way to recollect the component muscles involved in the hip movement, associated with coxa saltans is to view the iliopsoas tendon snapping over the iliopectinal or the femoral head. Whereas the thrust can sometimes be abrupt, it is uncommon to find that up to 4.3% of the patients experience total hip arthroplasty as the main cause of pain during the snapping process. Similarly, Bordoni, & Varacallo, (2020) observed from their studies that the most prominent cause of the pain during snapping is the malposition of the acetabular components of the hip region. As such, any diagnostic process must be based on the ability to detect the integrity or strength of muscles and tendons associated with the accessory ends of the pelvic region. As Yen, Lewis, & Kim, (2015) confirmed, the group of muscles that must be affected by the thrust movements are the iliopsoas tendon slips, the lesser trochanter, iliofemoral ligament, the femoral head, and the biceps of the ischium.
Having understood the process of snapping, and the anatomical positions or locations associated with coxa saltans, Bagwell, Bauer, Gradoz, & Grindstaff, (2016) proposed a scope of mechanisms to address the pain associated with the condition. One way to ensure patients have appropriate physical activity is to perform a regular and timely diagnostic procedure. In its management, health practitioners have proposed, like Bagwell, Bauer, Gradoz, & Grindstaff, (2016) confirmed that the first critical step is to understand the precise cause to be able to determine the right physical intervention exercise. On the same note, Balletto, (2019) asserted that various potential etiologies pose the greatest challenge as to understand or determine the precise mechanism or approach to use to manage the pain caused by snapping. The mode of manual therapy to implement depends on the understating of the precise cause because most of the patients affected experience pain and injuries due to various physical factors. Balletto, (2019) suggest that adult athletic injuries are mostly associated with the occurrence of hip problems. To exclude the possibility of other disorders, care providers must first conduct an accurate diagnosis, based on the origin and location of the pain. If the hip joint experiences severe pain, it can be accompanied by the fact that certain muscles and tendons undergo thrust or tension, resulting in movements majorly associates with pain and the sort of internal snapping symptoms. As the condition progresses, the affected muscles can be associated with three major aspects, which include internal, intraarticular, or external causes. Harris et al., (2020) observed that while there can be different etiologies, the most common result of pain occurs when the iliopsoas tendon goes through strain, and the associated movements lead to internal snapping hip. On the same note, Harris et al., (2020) affirmed that the snapping of the tendon can implicate various other structures that lie deeper beneath the hip region and the flexion muscles. The femoral head, being one of the proximal parts to the iliopsoas tendon, is among the first structures affected by the snapping. In the event snapping occurs, other structures such as the iliopectineal eminence and lesser trochanter are affected. The iliofemoral ligaments can also move over the anterior hip capsule so that most functions to do with muscle movements are not efficient enough to stabilize the hip region. Harris et al., (2020) also state that as an athlete or dancer, it is usually common for the proximal hamstring tendon to snap over the ischial tuberosity. On the other hand, Harrison, & Ruddock-Hudson, (2017) also suggest that dancers and athletes more commonly suffer coxa slatans as a result of snapping of the iliotibial band, facia latae, gluteus maximus, or the three combined can snap over the greater trochanter. As the posterior iliotibial band or anterior gluteus maximus travels over the greater trochanter, the body undergoes a derangement in the functional relationship, during the flexion and extension of the hip joint.
On a diagnostic scale, the patient ought to experience an audible snapping noise on the hip that is usually accompanied by pain. To associate the snapping with coxa slatans, it is Harrison, & Ruddock-Hudson, (2017) provides that the patient should have experienced persistent pain over a long period. The authors also observe that the noise and discomfort occur mainly when the patient goes through a training session. According to Kjeldsen et al., (2020), patients can either present no pain or severe incapacitating pain on a performance scale. The authors refer to the pain as incapacitating when it limits the ability of the patient to train and perform. If the hip joint experiences severe pain, it can be accompanied by the fact that certain muscles and tendons undergo thrust or tension, resulting in movements majorly associates with pain and the sort of internal snapping symptoms. It is the condition whereby the snap is caused by the movement of either the posterior iliotibial band or the anterior portions of the gluteus maximus. Usually, when pain occurs, the patient is advised to perform some general stretching and strengthening exercises involving the hip flexors and the hamstring.
Following diagnosis of external coxa saltans, which is the most common, Kjeldsen et al., (2020) suggested that treatment of the patient should involve an Active Release Technique. Under this method, the exercise will be conducted to target three major areas of the hip region. The lateral hip complex, the gluteus maximus and medius, the entire ITB as well as the fascia latae. Kjeldsen et al., (2020) also observed that the Active Release Technique could affect the functions of ipsilateral limb, which included the adductor longus, brevis and the magnus, as well as gracilis. As Lee, & Nam, (2020) also affirmed, the Active Release Technique is a treatment that intends to tissue tension around the regions affected by the condition. Similarly, the technique attempts to restore normal functions of the tissues. Following such an intervention, patients usually report increased efficiency of the body function and general reduced pain. To assert the results, Lee, & Nam, (2020) observed in their studies of Active Release Technique that almost all the participating patients treated were satisfied by the results of the intervention, claiming that they experienced reduced pain by almost 50% upon the first visit. This would suggest that the technique is quite efficient for the treatment of coxa saltans. Upon subsequent visits, Lee, & Nam, (2020) assert that the patients experienced a further reduction of pain, and they reported close to 100 % impact on the restored functionality. Although the patient might still suffer from non-painful snapping, the number of occurrences is greatly reduced following the fourth visit to perform the intervention exercise.
History and physical examination Conducting a careful history and physical evaluation will often lead to a correct diagnosis and the identification of the correct anatomic position in which it exists (i.e. whether it is internal, intra-articular or external). Furthermore, according to Bordoni, & Varacallo, (2020), the practitioner can identify the region of interest-based on the patient’s description of snapping. Coxa slatan can manifest in the form of snapping but patients often describe it as a sensation that the hip has dislocated. While internal snapping is described as getting stuck or just snapping, patients often describe it as an audible component to the snapping. Nonetheless, the pathology of intra-articular snapping is odten described as an intermittent catching or clicking (Ganz & Ayres, 2018). therefore, it is always useful to ask the patient to identify an area where of snapping and in many cases, they will point the figure at the correct anatomical region. Bagwell, Bauer, Gradoz, & Grindstaff, (2016) agree that evaluating the patient’s muscular strength or gait can easily help in identifying issues of muscle imbalance or stability. An externally rotated gait that is also abducted may indicate instability or capsular laxity (Rogers & Revesz, 2020). In most cases, coxa saltans in conjunction with weaknesses of the gluteus medius are found. But Bordoni, & Varacallo, (2020) argued that the area of interest can only be isolated through a physical examination of the snapping hip, as well as through palpation around the entire joint. It is also important to examine the joint’s range of motion as well as the flexion, adduction and internal rotation or impingement (FAdIR) test, which can be useful in assessing for intra-articular or labral pathology. While the patient is lying in a supine position, dynamic testing, starting in a position of flexion, abduction and external rotation (FAbER) to extension, adduction and internal rotation (EAdIR) will often elicit iliopsoas tendon snapping. If the snapping can be I identified via anterior hip palpation, a diagnosis of coxa saltans interna is said to have been diagnosed.
While the patient is lying in a lateral position, as their affected leg up, an ober test can be conducted to assess for iliotibial band tightness. Active hip flexion followed by a passive abduction and extension can reproduce the snapping over the greater trochanter. also, having the patient stand and adduct the hip with circumduction can reproduce a visible snapping over the greater trochanter. Practitioners have also relied on radiographic evaluation as a means of assessing coxa salta. According to Rogers & Revesz (2020), plain radiographs are a critical part of evaluating hip injuries, even though there are no significant radiograph findings that have indicated the coxa saltans interna (Ganz & Ayres, 2018). plain radiographs may display some evidence of femoroacetabular impingement and if the anterial deformity is too large, the iliopsoas can snap over the femoral head. Magnetic resonance is rarely used for assessment because of its involvement with iliopsoas but it may also reveal some evidence of snapping with inflammation of the iliopsoas muscle or iliopsoas bursa. However, the diagnosis of coxa saltan can be clinically made. As IT band snaps over the trochanta, the process is visible and can often be shown by the patient. If imaging is performed, a focal thickening of the anterior edge of the gluteus maximus muscle, and a thickening of IT band can be seen (Ganz & Ayres, 2018). This thickening can best be demonstrated by T1-weighted images. However, if the snapping cannot be seen, dynamic sonography can be used to detect the movement of the IT band over the greater trochanter. Approximately 5% to 10% of the population is affected by coxa saltan, most of them experiencing painless snapping. However, according to Bordoni, & Varacallo, (2020), the prevalence appears to be higher in women than in men. Similarly, Balletto, (2019) observes that typically, the groups affected include those who engage in extreme and repetitive hip motions such as competitive ballet dancers. That said, data by Balletto, (2019) indicate that of the ballet dancers, 90% reported symptoms of snapping hip syndrome and 80% with bilateral involvement. Some of the ballet movements that are notorious for causing snapping to include external hip abduction and rotation of over 90 degrees. Existing research evidence shows that snapping hip syndromes can effectively be managed through interprofessional teams that include nurse practitioners, sports physicians, pain specialist, physical therapist, emergency department physician, and orthopedic surgeon (Harris et al., 2020). On the same note, Harrison, & Ruddock-Hudson, (2017) observed that the treatment depends on the presence of symptoms and conversely, asymptomatic patients do not need any treatment. On the other hand, those presenting with pain are encouraged to avoid heavy physical activity or enrol on a therapy program.
Findings such as bursitis and tendinitis seen on magnetic resonance imaging can help in the diagnosis of external coxa saltan (Bordoni & Varacallo, 2020). However, Bordoni & Varacallo (2020) observed that static modality cannot be used to identify the snapping. Even though the findings can support diagnosis, Yen, Lewis & Kim (2015) noted that a few cases of hips with internal coxa saltans had sonographic evidence of a thickened bursa. Nonetheless, Trammell & Pilson (2018) wrote that the recent use of dynamic ultrasound has received more success, allowing for the analysis of iliopsoas tendon movement. Nonetheless, Bordoni & Varacallo (2020) insisted that more research is needed to substantively validate these findings. Current literature mostly suggests that primary treatment for coxa saltan should be treated through non-invasive procedures such as nonsteroidal anti-inflammatory medication, physical therapy and activity-specific rest. Ideally, there is significant evidence to show that this treatment protocol has assisted many dancers to go back to their normal activity. For instance, the study by Trammell & Pilson (2018) found this treatment protocol to be effective without any additional intervention. Ideally, physical interventions are mostly used to improve flexibility, prevent reinjury, strengthen the surrounding Musculature and restore function. Much success has also been achieved through iliopsoas-specific dynamic strengthening and stretching, pelvic mobilization, antilordotic exercises and range of motion exercises. However, according to Bordoni, & Varacallo, (2020), only therapists with specific training and familiarity with iliopsoas treatment protocols would effectively work with the patients. Existing literature has also explored the unlikely event that a patient does not respond to treatment. According to Yen, Lewis & Kim (2015), such a scenario would necessitate the use of invasive procedures such as surgical intervention and corticosteroid injections. In a study by Micheli & Solomon (1997), the researcher treated patients with iliopsoas tendonitis using corticosteroid injections. A group of 17 patients received the injection, 53% of them consisting of dances, all of whom had failed to respond to conservative treatment. The researchers did not document any specific duration or methods of treatment for the physical therapy. While there were no complications reported, two participants who returned to full level activity reported poor activity when returning to athletics or dance. For the patients that fail early conservative therapy and fail to respond to corticosteroid injections, there is a paucity of literature on effec6uve surgical management interventions. On a daily exercise regimen, patients can undergo a lateral pelvic stability program. Laskowski et al., (2020) define the program as an intervention designed to rectify decreased abduction strength. It also targets patients who experience faults in the pelvic abduction firing pattern, in the sense that exercises lead to increased friction between the lateral and ITB complex and the greater trochanter. Under increased tension, Laskowski et al., (2020) believe the rationale behind the exercise regimen is that when the hip abductor strength decreases, the internal rotation and hip adduction consequently increases as a result of the weight-bearing activity. With such interventions in place, the ITB complex is subjected to increased tension, thus prompting the need to place the patient on a supervised lateral pelvic stability program, whereby training sessions target the critical tissues affected. As a critical part of the hip region, the pelvis usually consists of muscles that rely on a determinate mechanism of movement to be able to prevent strain or tension that can result into abrupt pain. One way to recollect the component muscles involved in the hip movement, associated with coxa saltans is to view the iliopsoas tendon snapping over the iliopectinal or the femoral head. To ensure the program becomes effective, it is upon the instructor and the patient to attend the training sessions at regular intervals to allow for predictability and the ability to monitor the results or outcomes of the intervention. Laskowski et al., (2020) suggest the convenient time or duration for the training become effective and achieve positive results should not be less than 4 weeks, and the patient attends once per week, coupled with a daily exercise regimen. An effective model includes in-house sessions where the patient performs resisted abduction of the gluteus medius and straight leg abduction accompanied by manual biofeedback. As a practitioner, Michiels Hernandez, (2013) suggests that one should accomplish the manual biofeedback by palpating the gluteus group and be able to place the patient in such a position as to contract the designated muscles during the training session, or exercise regimen. The femoral head, being one of the proximal parts to the iliopsoas tendon, is among the first structures affected by the snapping. In the event snapping occurs, other structures such as the iliopectineal eminence and lesser trochanter are affected. The iliofemoral ligaments can also move over the anterior hip capsule so that most functions to do with muscle movements are not efficient enough to stabilize the hip region. According to Miehlke, & Schmidt, (2015), the intervention seeks to restore functionality in the patient by activating the musculature of the lateral gluteus. Besides, it facilitates a feedback mechanism between the central nervous system and proprioceptive neuromuscular tissues to recreate the cortical motor programs. Miehlke, & Schmidt, (2015) further suggested lateral wobble board training, whereby the patient performs both single and double leg stances. To make the exercise effective, the wobble seeks to progress from the double leg to single leg stances. The trainer supports the patient by making sure they manually push the pelvis in random directions. At home, the exercise involves resisted lateral walks, while performing hip hikes.
Chapter 3
3.0 Research Methodology
3.1 Research design
The study took a quantitative, experimental research design administered on a pretest-posttest design whereby, the dependent variable is measured once before the treatment intervention is implemented and once after the treatment intervention is implemented (Shen et al, 2019). The main aim of the study was to test whether amateur dancers aged 18-26 years, presenting with clinical impressions of external snapping hip syndrome (coxa saltan), benefit from static stretches over a 4-week duration. Therefore, the researcher needed to experiment to evaluate whether static stretches would work as a treatment intervention for coxa saltan. While the pretest-posttest experimental design is much like the within-subjects design where subjects are first tested under a control condition then later under a treatment condition (Zhou et al, 2017). However, it differs from within-subject experiments in the sense that the order of conditions is not counterbalanced because the participants cannot be tested in the treatment condition first before they are tested in the ‘untreated’ condition. Ideally, in a quasi-experimental design, the intervention is considered effective if the average posttest results are better than the average pretest score. Therefore, in the present study, the researcher conducted a pre-test Hip dysfunction and Osteoarthritis Outcome Score (HOOS) on the participants before the intervention (i.e. at baseline) then another HOOS test was conducted after the intervention to conclude on the effectiveness of the intervention to improve coxa saltan symptoms. There are several advantages of quasi-experimental design that warranted its application in the present study. For instance, the greatest advantage of experimental research design would only need a few resources and less expensive to conduct compared to other types of quantitative studies such as randomized control trials (Ganz & Ayres, 2018). Furthermore, according to Manshur & Husni (2020), the environment where the study is conducted could be easily controlled. More importantly, quasi-experimental designs meet the requirements of causality. However, this study design also exposed the study to potential selection bias, historical bias and instrumentation bias (Rogers & Revesz, 2020).
3.2 Research sampling
The COVID-19 pandemic has not only affected how people work but also how people go about doing research. While many researchers have had to suspend or postpone their data collection, others have had to re-design their projects to consider the social distancing requirements (Doughtery, 2017). According to Vass et al (2017), one of the major elements of experimental studies that must be redesigned is the sampling techniques, so that they can align with the current COVID-19 control measures. Against this backdrop, according to Hoeber & Shaw (2017), most researchers have opted for more flexible sampling techniques such as convenient sampling and snowball sampling . The study relied on convenient sampling to select participants. Convenient sampling entails the selection of only the conveniently available participants. It is one of the most commonly used sampling methods because it is economic, prompt, and uncomplicated. The inclusion criteria were amateur dancers aged 18-26 years, presenting with clinical impressions of external snapping hip syndrome (coxa saltan). Potential participants were invited to complete an online Survey Monkey quantitative questionnaire (see Appendix 2) to ensure they are only presenting with clinical impressions of coxa saltan, and no other known potential lower limb injuries are presenting. Twenty participants who present with the most extreme clinical impressions of SHS from the questionnaire were then chosen for the study, with the ten most affected by SHS chosen to undertake the online intervention programme. Each participant chosen completed the Hip dysfunction and Osteoarthritis Outcome Score (HOOS). This test was performed on all twenty participants at the start and end of the 4-week treatment plan regardless of whether they were part of the intervention group.
3.3 The intervention
Conservative treatment (applicable stretches) was performed twice a week for 2-sets of 30-seconds on each leg, over four weeks. The static stretching technique was used to impact the TFL and glute max muscles. If lockdown measures would be lifted during the 4 weeks, soft tissue release (STR) methods would also be incorporated via:
3.4 Gluteus maximus
-Patient lay in a prone position.
-Pin the elbow into the gluteus maximus
-Internally and externally rotate the patients hip slowly (the slower you do this the more tissue you go over, the faster you do this the more superficial muscle you go over) -Do 3 sets of this and 10 reps 3.5 Tensor-fascia Lata- -Patient lay in a supine position with the hip flexed off the end of the bed -Locate the TFL muscle and rest my thumb on it -Patient then flexed their hip -The patient slowly controlled the leg down -Apply pressure to the TFL -then let go -The patient flexed the hip -Do 3 sets of this and 10 reps
3.6 The Hip dysfunction and Osteoarthritis Outcome Score (HOOS)
The HOOS is a symptom assessment questionnaire that evaluates patients’ opinion regarding their hips and any associated problems while evaluating the functional limitations that relate to the hips as they undergo a treatment process (Lebert, 2020). according to Arbab et al (2017), the HOOS is a substitute for other questionnaires such as Algo Functional Index (AFI), intermittent and Constant Osteoarthritis Pain Index (ICOAP), and the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC). The HOOS, as a measuring instrument, a tool for judging the anatomical qualities and functions as well as a tool for measuring the patient’s participation in various hip-involving activities; is recommended for use when there is a hip disability with or without osteoarthritis (OA) (Arbab et al, 2017). According to Sunden et al (2018), hip osteoarthritis is a chronic musculoskeletal condition that causes pain, reduced quality of life and functional disability in patients. Therefore, the HOOS can be used over long-term and short-term intervals to assess any changes induced by a treatment intervention. The HOOS is a self-explanatory, user-friendly questionnaire that can be administered within 7 to 10 minutes. The outcome scores are assessed within 5 subscales of Activity limitations daily living (ADL), hip-related quality of life (QOL), Symptoms (S) and Pain (P).
3.7 Data Analysis and presentation
The responses to the Hip dysfunction and Osteoarthritis Outcome Score (HOOS) before treatment and after the 4-week treatment plan Were then collected and analyzed using statistical analysis via Microsoft excel and pivot tables. Ideally, a pivot table is data analysis tools that facilitate an easier analysis and synthesis of data by condensing them (Rogers & Revesz, 2020). Typically, a pivot table consists of data fields, rows, pages and columns that can be moved around to isolate, expand, group and sum data in real-time. Pivot tables also allow users to view differences between big sets of data – thereby helping with data organization in Microsoft excel. There are several advantages of pivot tables that qualified them for use in the current study. For instance, they can take user data and convert each column’s header into a data set that can easily be manipulated (Rogers & Revesz, 2020). Consequently, they allow for a user-friendly and informative summary to be created around spreadsheets of raw data. The other advantage of pivot tables is that they are easy to use because the researcher can summarize data by simply dragging the columns into different table sections. The columns can also be easily re-arranged during the data manipulation process.
3.8 Ethical considerations
Experiments involving human subjects must adhere to specific ethical standards that have been set by the university. In this regard, Orero et al (2018) strongly suggested that, regardless of the research design, researchers must make various ethical considerations to ensure that the subjects are not physically, emotionally or psychologically harmed. Against this backdrop, the present study made several ethical considerations as highlighted below: First, the study obtained ethical approval from the university’s ethics committee to ensure that the study aligned with the university’s research ethics standards. Secondly, before the experiment began, all participants were asked to sign an informed consent form (Appendix 1) to ensure voluntary participation. Apart from reinstating the aspect of freedom to participate, the researcher also ensured equity or justice – whereby all participants were considered the same way during the entire study. Moreover, the mere fact that there were no participant dropouts indicated that the entire research process adhered to the benevolence ethnical principle, whereby no nuisance nor harm was inflicted on any participant. More importantly, the researcher adhered to the confidentiality and privacy ethical principle, whereby no personal information (e.g. name, email address, institutional affiliation) was shared or gathered. Confidentiality was also maintained by storing all participant data in a password-locked flash-disk. The data was then discarded after use.
Chapter 4
4.0 Results
This chapter presents the results of the data analysis based on the underlying research question, as well as any results that emerge from further analysis. The results will be presented with minimum interpretation as the interpretation is reserved for the discussion section. That said, the study involved 20 participants, ten in the intervention group and the other ten in the non-intervention. The intervention group were exposed to static stretching techniques performed twice a week for two sets of 30 seconds on each leg, all conducted within four weeks. All the a20 subjects took part in a pre-test evaluation, filling the HOOS questionnaire to evaluate their coxa saltan symptoms before the intervention. Similarly, all the 20 subjects filled the HOOS at the end of the four-week experiment – implying that no participant dropped out of the experiment. The intervention involved a video demonstration of various static stretching techniques that each patient in the intervention group was supposed to follow. The static stretching techniques were applied to the lateral hip complex including the Maximus, gluteus medius, the TFL and the fascia latae. This treatment was aimed at decreasing the muscle tension while bringing the tissue function to normal. All the patients in the intervention group reported pain reduction after the four-week intervention. The following table illustrates the results of both the intervention and the control group:
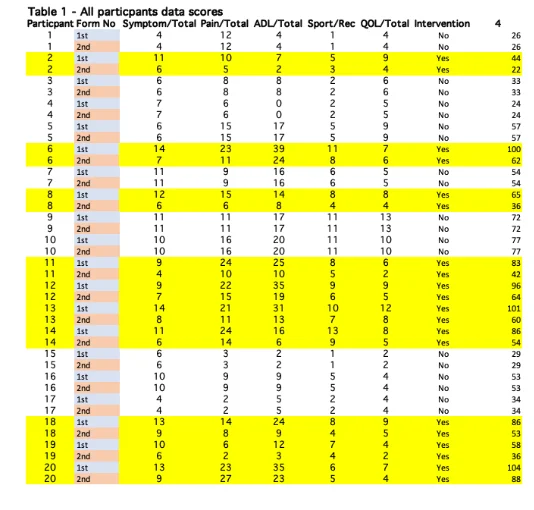
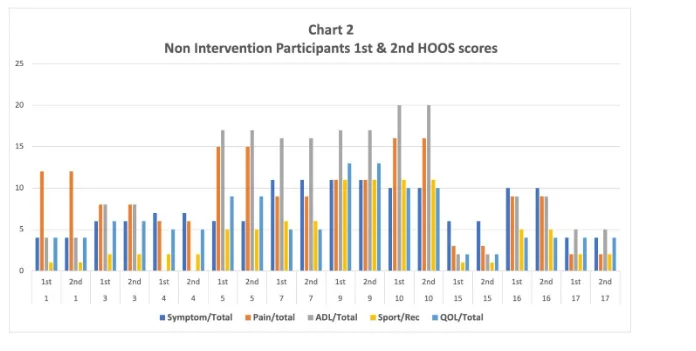
None of the participants indicate a total symptom score of below 4, while none of them displayed a total pain score of below 2 (before and after the intervention). On the other hand, the lowest score on ADL scale was 1, while none of the participants scored below 4 in the QOL scale. At week four, the minimum total score for all the participant was 22. Conversely, the highest score on the total symptom score for all the participants before and after the intervention was 13, while 27, 35, 11, and 13 were the highest scores among the participants in the total symptom, total pain, total ADL, sport, and total QOL scales respectively before and after the intervention. The non-intervention group did not display any change on the HOOS in the first and second HOOS test , indicating that generally, by not participating in the static stretching intervention, no change would be expected on their total symptoms scores, total pain scores, total ADL score, and total QOL score. An excel pivot analysis on the data revealed the following graphical presentation.
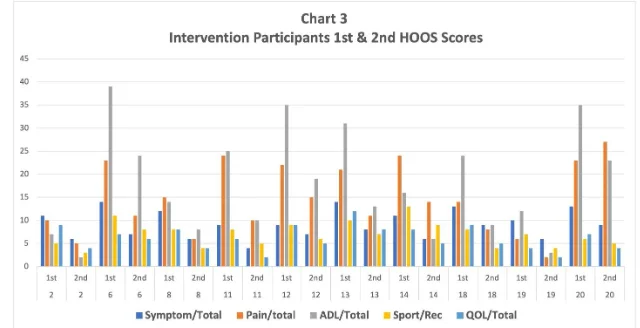
Contrastingly, all the intervention group participants indicated a change total symptom, total pain, total ADL, sport, and total QOL scales respectively. Participant 6 displayed the highest change in total symptom scale (from 14 in the first HOOS measurement to 7 in the second HOOS). On the other hand, participant 12 indicated the lowest change in the symptom scale (from 9 in the first HOOS test to 4 in the second HOOS test). Participant 11 displayed the highest change in the pain scale (from 24 in the first HOOS measurement to 10 in the second HOOS measurement) while participant 19 indicated the lowest change in the total pain score (from 6 in the first HOOS measurement to 2 in the second HOOS measurement). Interestingly, participant 20 recorded an increase in the total pain score from 23 in the first HOOS measurement to 27 in the second HOOS measurement.
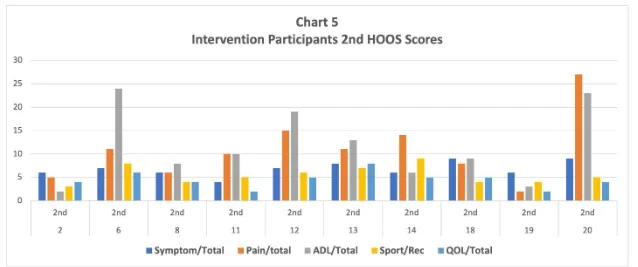
On the total ADL scores, participant 12 reported the highest change (from 35 in the first HOOS measurement to 19 in the second HOOS measurement); while participant 2 reported the lowest change in total ADL score (from 7 in the first HOOS measurement to 2 in the second HOOS measurement). On the other hand, participants 14 and 18 reported the highest changes (a change of 4 points between the first HOOS measurement and second HOOS measurement) in the sports and recreational activity scales, while participant 20 recorded the lowest change in sports and recreational activity scales (a change of 4 points between the first and second HOOS measurement). Lastly, participants 8, 11, 12, 13, and 18 recorded the highest change in quality of life scale of four points from the first HOOS measurement and the second HOOS measurement. On the other hand, participant 6 recorded the lowest change in quality of life scale (a 1-point change from the first HOOS measurement to the second HOOS measurement). An excel pivot analysis revealed the following graphical representation:
Chapter 5

5.0 Discussion and Conclusion
In the fourth week, all the patients in the intervention groups reported a general reduction in pain, even though non-painful snapping was still present in all of them at this time; however, the patients reported that the number of pain occurrences had significantly reduced. Ideally, as revealed in the literature review, a further physical exercise regimen can be initiated to create lateral pelvic stability to correct the diagnostic findings of faulty pelvic abduction firing pattern (TFL substitution) and decreased strength of abduction. According to Laskowski et al., (2020), such faults are believed to put the patients at a high risk of fibrosis because they increase the friction between the greater trochanter and the lateral ITB complex. This argument assumes that a decreased hip abductor dysfunction could lead to a decreased hip internal rotation and abduction during any weight-bearing activity, increasing the tension at the ITB complex (Miehlke, & Schmidt, 2015). Therefore, the intervention group participants would further benefit from a physical activity regimen that activates the lateral gluteus musculature to provide some proprioceptive neuromuscular feedback to the central nervous system; to trigger proper cortical motor programs. the structure of ITB originates from the iliac crest and joins with the collective fascia of the gluteus maximus posteriorly, the tensor fascia latae anteriorly, and indirectly from the fascia of the gluteus medius (Lee, & Nam, 2020). The ITB deeply inserts into the linea aspera of the femur and the lateral aspect of the Tibia at Gerdy’s tubercle, with some anterior fibres attaching to the lateral retinaculum and patella. It is the complex insertion and origin of this structure that allows it to be taut during all the hip motions. Any increase in tension combines with motion repetition increases the friction over the greater trochanter, which may cause inflammation or irritation of the trochentric bursa, as well as chronic degenerative changes that may be associated with fibrosis (Lee, & Nam, 2020). Miehlke, & Schmidt, 2015 confirmed that chronic fibrosis can also cause gluteus maximus, ITB, TFL, facia latae and a snap over the greater trochanter that can lead to external coxa saltans (Laskowski et al., 2020). The increased tension can be caused by various biomedical causes including internal tibial torsion, anteversion, an ipsilateral long leg, and excessive foot pronation. However, locomotion further complicates the biomechanics of ITB’s pull. But several studies have examined the effects of weak lateral hip muscles and described them in detail. For instance, Miehlke, & Schmidt (2015) was among the first to describe the contralateral hip drop on weight-bearing, which identified the weakness of ipsilateral gluteus medius. While tensor fascia latae and gluteus medius are both hip abductors, gluteus medius is also an external hip rotator. Therefore, any weakness in the gluteus medius can cause a decrease in the hip abduction control and affect internal rotation.
Subsequently, while dancing or running, the patient will depict an increased hip abduction and internal rotation; with an increased valgus vector at the knee (Lee, & Nam, 2020). It is assumed that this increases ITB complex’s tension on both the femur’s greater trochanter and the lateral epicondyle of the femur (Michiels Hernandez, 2013). Many surgical procedures have been proposed to address this increased friction, and each of those procedures has different degrees of difficulty (Lee, & Nam, 2020). According to Miehlke, & Schmidt (2015), some of the most common operative procedures include diagonal osteotomy of trochanter, Z-plasty, cruciate incision with sutured flaps to the tract, ellipsoid resection of tract over the trochanter, and anchoring of the iliotibial tract to the trochanter. While most of these operative procedures attempt to decrease the tension between the trochanter and the ITB complex, many authors (Michiels Hernandez, 2013; Miehlke, & Schmidt, 2015) still agree that conservative treatment should be adopted in the therapy. Also, even though many treatment options have been suggested, there is a paucity of evidence of any therapy that is better than the other. Static stretching is a technique of addressing soft tissue dysfunctions and lesions acquired through repetitive activities such as dancing. Miehlke, & Schmidt (2015) proposed a mechanism (cumulative injury cycle) that can be used to explain increased tissue tension or tissue stiffness. During this cycle, the small repetitive injuries in the tight muscles cause an increase in tension and friction within the myofascial structures. The tension can either lead to a decreased blood circulation in the tissue (chronic cycle) or a crush injury (inflammation cycle) (Miehlke, & Schmidt, 2015). Both the inflammation cycle and the chronic cycle leads to an accumulation of fibrosis and adhesions within the tissue. Thus, the cumulative cycle of injury occurs as a self-perpetuating phenomenon and as the downward spiral continues, the syndromes and symptoms of the cumulative injury disorder emerge. It is therefore the goal of static stretching to remove these ‘adhesions’ leading to a reduced tissue tension and thereby stopping this cumulative cycle of injury. During static stretching, the involved tissues are taken from a shortened position to a lengthened position while the contact hand longitudinally holds along the lesions and soft tissue fibres. Apart from the current study, the effectiveness of this technique has also been found by other practitioners using it to address various issues of tissue dysfunction (Howitt 2006; Pajaczkowski 2003, Kazemi 2000, Buchberger 1999, Buchberger, D. J., Rizzoto, H., & McAdam, B. J. (1996). Median nerve entrapment resulting in unilateral action tremor of the hand. Journal of Sports Chiropractic & Rehabilitation, 10(4), 176-179). In a study by Schiottz-Christensen (1999), the researchers found that the technique could be used in treating an upper extremity overuse syndrome with a 71% efficacy rate. In the current study, while the pain symptoms were significantly eliminated, a complete patient rehabilitation required a comprehensive rehabilitation plan aimed at correcting the pelvic stability issues reported by most patients.
5.1 Conclusion
In conclusion, compared to other hip conditions, coxa saltan is considered a common cause of hip dysfunction among athletes and dancers because they perform repetitive motions that lead to snapping of the hip. While there is a paucity of guidance in literature regarding the best and optimal treatment intervention for coxa saltan, practitioners should be tried before considering surgical treatment. In most cases, the practitioner is left to experiment with various treatment options that can resolve the patient’s condition. static stretching is one of the treatment options. It relieves tissue tension by removing adhesions/fibrosis that develops in tissues that are overloaded as a result of repetitive use. In most cases, coxa saltan is caused by increased tissue tension that causes increased friction between the proximal ITB complex and the greater trochanter. This study attempted to resolve this condition using static stretching and found significant pain and symptom improvement among the intervention group. However, an elaborate rehabilitation protocol should be developed to correct the contributing pelvic muscle imbalance that might persist after the intervention. Nonetheless, more research is needed to demonstrate the histological and pathophysiologic mechanisms of static stretching, as well as its clinical usefulness.
5.2 Implications for practice
To our knowledge, this is among the latest reported study that seeks to evaluate the effectiveness and efficacy of static stretching technique targeting the dancing population. The incidence of coxa saltan in dancers is significant, totalling 50% of the population in this study. Literature shows that the incidence is more prevalent in younger female dancers. Coxa saltan has a characteristic clinical presentation that was evaluated through the HOOS. The HOOS was considered the most reliable method of diagnosis. In the current study, static stretching technique proved to be effective in treating HOOS. However, a possible implication of this study is that should pain persist after the physical therapy, it is important to explore other treatment options or use MRI to evaluate other causes of the pain. This study has shown that coxa saltan is common with dancers who regularly engage in dancing activities. therefore, when treating any member of a dancing crew presenting with the above-discussed symptoms, coxa saltan should be considered. Dances are typically prone to coxa saltan because of the repetitive hip flexion movements they perform as they dance. Based on the findings of the current study, conservative treatment (i.e. Static stretching technique) can be used as primary treatment for these patients.
References
- validity, responsiveness and minimally important change of the German hip dysfunction and osteoarthritis outcome score (HOOS) in patients with osteoarthritis of the hip. Rheumatology international, 37(12), 2005-2011.
- Boyd, K. T., Peirce, N. S., & Batt, M. E. (1997). Common hip injuries in sport. Sports Medicine,
- approach in the correction of external coxa saltans: the snapping hip. The American journal of sports medicine, 32(6), pp.1504-1508.
- Unrecognized Cause of Coxa Saltans in the Adult. Clinical Orthopaedics and Related Research (1976-2007), 355, 261-271.
- Wahl, C. J., Warren, R. F., Adler, R. S., Hannafin, J. A., & Hansen, B. (2004). Internal coxa saltans (snapping hip) as a result of overtraining: a report of 3 cases in professional athletes with a review of causes and the role of ultrasound in early diagnosis and management. The American journal of sports medicine, 32(5), 1302-1309.
- Brignall, C.G., Brown, R.M. and Stainsby, G.D., 1993. Fibrosis of the gluteus maximus as a cause of snapping hip. A case report. JBJS, 75(6), pp.909-910.
- Waters, P. M., & Millis, M. B. (1988). Hip and pelvic injuries in the young athlete. Clinics in sports medicine, 7(3), 513-526.
- Manshur, F. M., & Husni, H. (2020). Promoting Religious Moderation through Literary-based Learning: A Quasi-Experimental Study. International Journal of Advanced Science and Technology, 29(6), 5849-55.
- Orero, P., Doherty, S., Kruger, J. L., Matamala, A., Pedersen, J., Perego, E., ... & Szarkowska, A. (2018). Conducting experimental research in audiovisual translation (AVT): A position paper. JosTrans: The Journal of Specialised Translation, (30), 105-126.
- Bagwell, J. J., Bauer, L., Gradoz, M., & Grindstaff, T. L. (2016). The reliability of FABER test hip range of motion measurements. International journal of sports physical therapy, 11(7), 1101.
- Brignall, C. G., Brown, R. M., & Stainsby, G. D. (1993). Fibrosis of the gluteus maximus as a cause of snapping hip. A case report. JBJS, 75(6), 909-910.
- Besomi, M., Maclachlan, L., Mellor, R., Vicenzino, B., & Hodges, P. W. (2020). Tensor Fascia Latae Muscle Structure and Activation in Individuals With Lower Limb Musculoskeletal Conditions: A Systematic Review and Meta-Analysis. Sports Medicine, 1-21.
- Caine, D., Bergeron, G., Goodwin, B. J., Thomas, J., Caine, C. G., Steinfeld, S., ... & André, S. (2016). A survey of injuries affecting pre-professional ballet dancers. Journal of Dance Medicine & Science, 20(3), 115-126.
- Harris, J. D., Mather, R. C., Nho, S. J., Salvo, J. P., Stubbs, A. J., Van Thiel, G. S., ... & Kivlan, B. R. (2020). Reliability of hip range of motion measurement among experienced arthroscopic hip preservation surgeons. Journal of Hip Preservation Surgery, 7(1), 77-84.
- Kjeldsen, T., Reimer, L. U., Drejer, S. M., Hvid, L. G., Mechlenburg, I., & Dalgas, U. (2020). Is progressive resistance training feasible in patients with symptomatic external snapping hip?. Physiotherapy Theory and Practice, 1-13.
- Laskowski, E. R., Johnson, S. E., Shelerud, R. A., Lee, J. A., Rabatin, A. E., Driscoll, S. W., ... & Terzic, C. M. (2020, August). The telemedicine musculoskeletal examination. In Mayo Clinic Proceedings (Vol. 95, No. 8, pp. 1715-1731). Elsevier.
- Malinowski, K., Kalinowski, Ł., Góralczyk, A., Ribas, M., Lund, B., & Hermanowicz, K. (2020). External Snapping Hip Syndrome Endoscopic Treatment:“Fan-like” Technique as a Stepwise, Tailor-made Solution. Arthroscopy techniques, 9(10), e1553-e1557.
- Lee, S. H., & Nam, S. M. (2020). Effects of Active Release Technique on Pain, Oswestry Disability Index and Pelvic Asymmetry in Chronic Low Back Pain Patients. Korean Society of Physical Medicine, 15(1), 133-141.
- Mosler, A. B., Kemp, J., King, M., Lawrenson, P. R., Semciw, A., Freke, M., ... & Ageberg, E. (2020). Standardised measurement of physical capacity in young and middle-aged active adults with hip-related pain: recommendations from the first International Hip-related Pain Research Network (IHiPRN) meeting, Zurich, 2018. British journal of sports medicine, 54(12), 702-710.
- Panhale, V. P., Walankar, P. P., & Sridhar, A. (2020). Analysis of postural risk and pain assessment in bharatanatyam dancers. Indian Journal of Occupational and Environmental Medicine, 24(2), 66.
- Pajaczkowski, J. A. (2003). Mimicking turf-toe: myofasopathy of the first dorsal interosseous muscle treated with ART®. The Journal of the Canadian Chiropractic Association, 47(1), 28.
- Pragassame, S. A., Kurup, V. K., & Kumar, R. S. (2019). Effectiveness of Active Release Technique Versus Myofacial Release Technique on Patients with Plantar Faciitis: A Comparitive Study. Indian Journal of Public Health Research & Development, 10(10), 460-465.
- Randelli, F., Mazzoleni, M. G., Fioruzzi, A., Via, A. G., Calvisi, V., & Ayeni, O. R. (2020). Surgical interventions for external snapping hip syndrome. Knee Surgery, Sports Traumatology, Arthroscopy, 1-8.
- Robinson, D. B., Randall, L., & Andrews, E. (2020). Physical education teachers’(lack of) gymnastics instruction: an exploration of a neglected curriculum requirement. Curriculum Studies in Health and Physical Education, 11(1), 67-82.
- Sadria, G., Hosseini, M., Rezasoltani, A., Bagheban, A. A., Davari, A., & Seifolahi, A. (2017). A comparison of the effect of the active release and muscle energy techniques on the latent trigger points of the upper trapezius. Journal of Bodywork and Movement Therapies, 21(4), 920-925
- Sundén, A., Lidengren, K., Roos, E. M., Lohmander, L. S., & Hansson, E. E. (2018). Hip complaints differ across age and sex: a population-based reference data for the Hip disability and Osteoarthritis Outcome Score (HOOS). Health and quality of life outcomes, 16(1), 1-6.
- Schiottz-Christensen, B., Mooney, V., Azad, S., Selstad, D., Gulick, J., & Bracker, M. (1999). The role of active release manual therapy for upper extremity overuse syndromes—a preliminary report. Journal of Occupational Rehabilitation, 9(3), 201-211.
- Winston, P., Awan, R., Cassidy, J. D., & Bleakney, R. K. (2007). Clinical examination and ultrasound of self-reported snapping hip syndrome in elite ballet dancers. The American journal of sports medicine, 35(1), 118-126.



- 24/7 Customer Support
- 100% Customer Satisfaction
- No Privacy Violation
- Quick Services
- Subject Experts