Bones of the Shoulder Girdle
Introduction
The key function of the shoulder girdle is to ensure proper strength to the arm and allow effective motion for movement. The three main bones present in the shoulder girdle are scapula, humerus and clavicle. In this assignment, the detailed structure and function of the shoulder girdle are to be explained. In addition, a condition of shoulder impingement is to be discussed and the intervention taken by the chiropractor to resolve the condition is to be mentioned.

Structure of Shoulder Girdle
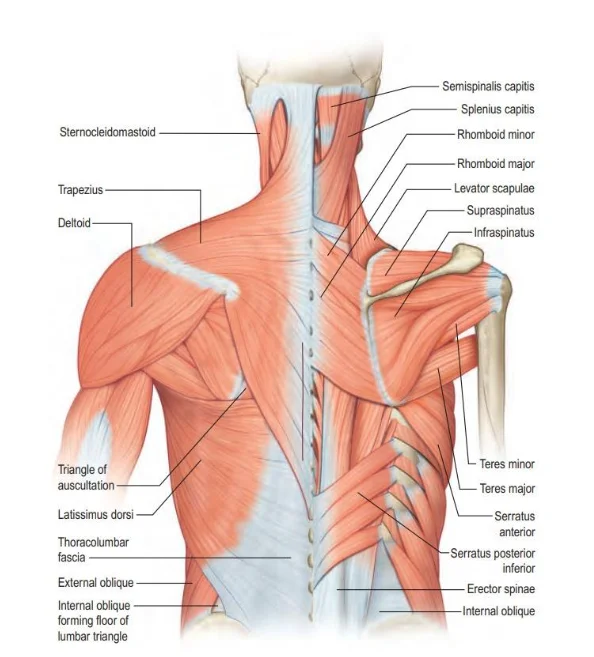
The shoulder complex structure includes three bones which are humerus, clavicle, and scapula. The scapula is uniquely framed by making it connected in a loose manner with the trunk during free sliding on the back. There are many muscles which support scapula ensuring the force is properly transferred from the arm to the trunk. The bones of the shoulder girdle are positioned such as the scapula is positioned posteriorly, the clavicle is anteriorly positioned and the humerus is laterally placed (Niyetkaliyev et al. 2017; Zheng et al. 2017). These bone structures form 3 joints that allow the movement of the shoulder. Firstly the primary “shoulder joint” known as the glenohumeral joint is the most lateral of the shoulder girdle joints. It is the articulation of the ball of the humerus with the very shallow glenoid fossa of the scapula. Secondly, the acromioclavicular joint is located superiorly where the clavicle articulates with the acromion process of the scapula (Ludewig & Lawrence, 2017). Thirdly the sternoclavicular joint located in the anterior aspect of the upper chest where the medial aspect of the clavicle articulates with the sternum of the chest wall. A fourth non-bony joint exists in the shoulder girdle. This is the scapula-thoracic joint between the scapula and the posterior aspect of the thorax and this joint account for thirds of shoulder movements (Qu et al. 2019).
Other structures involved in shoulder joint movements and stabilization are ligaments, tendons and muscles. There are two types of ligaments known as intrinsic and extrinsic. Ligaments that help support the shoulder joint include:
The Acromioclavicular is located superior and it is a quadrilateral ligament that is thin. It is between the upper aspect of the lateral end of the clavicle and the acromion where it provides attachment for the intra-articular disc (articular disc – completer fibrocartilaginous creating medial and lateral compartments). (Tunstall 2015, p. 810)
The Articular Capsule is a ligamentous structure that completely covers the shoulder joint complex. It is attached above to the circumference of the glenoid cavity beyond the glenoidal labrum and below the neck of the humerus near the articular cartilage. Though loose to allow movement, it confers stability to the entire joint and reduces the chance of humeral dislocation.
The Cocacoclavicularmakes the connection between the clavicle and the coracoid process of the scapular. Although it is a separate ligament, it has an important function. It supports the suspension of the scapula. (Tunstall 2015, p. 809 - 810)
The coracohumeral Ligament reinforces the upper part of the shoulder joint capsule. It is a broad band which travels from the coracoid process of the scapula to the greater tubercle of the humerus and blends with the tendon of the supraspinatus.
Glenohumeral Ligaments consist of three bands that provide strength for the shoulder capsule.
The Transverse Humeral Ligament (also known as the Brodie ligament) passes from the lesser to the greater tubercle of the humerus (Foster, Hacking 2019), superiorly to the epiphyseal line, converting the biceps bicipital grove into a canal (MacDonald 2007).
The Glenoidal Labrum is triangular in section that varies in size and thickness. Made of the fibrocartilaginous rim around the glenoid fossa, it protects the bone and assists with lubrication. (Tunstall 2015, p. 813)

Abduction of the shoulder
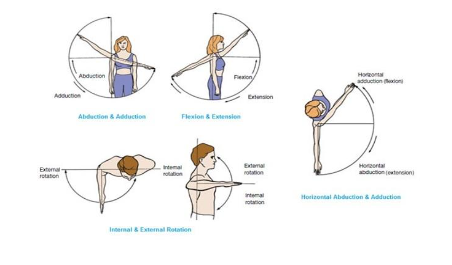
The normal movement of the shoulder requires all the four articulation that are glenohumeral joint (GH), sternoclavicular joint (SC), acromioclavicular joint (AC) and physiological-scapulothoracic (ST) and subacromial joints to be effectively working. In the frontal plane, for the lateral abduction of humerus, a number of joints are required along with group of muscles to work collaboratively (Kim & Deshpande, 2017). The GH joint for the initial 15-30º of shoulder abduction is seen to work by itself. The supraspinatus contraction is seen to be responsible for initiating much of the humerus abduction. In order to elevate humerus by contracting deltoid, the humeral head is required to be rolled and glided in the glenoid fossa. The muscular action executed by supraspinatus muscle leads the humerus head to be glided in a downward position on the glenoid fossa and this action is executed in relation with teres minor and infraspinatus muscles. The shoulder movement leads heads of the humerus to be rolled and translated and the degree of this translation is seen to be limited by the motion of the scapulothoracic muscles. At the 150º elevation, the deltoid becomes more activated and the acromial or lateral fibres of the deltoid muscles are found to be strong abductors of humerus located at the joints of the shoulder that is innervated by the presence of axillary nerves (Umehara et al. 2017). The scapula after initial mobility initiates to rotate in lateral way and for the scapula to rotate in upward position needs the upper trapezius to be contracted and the lower fibres of the serratus anterior muscles. The occurrence of the rotation of the scapula at the acromioclavicular joint leads it to get slide on the scapulothoracic joint resulting to tilt the glenoid fossa in upward position. At this moment, the movement of humerus and scapula is known as scapula-humoral rhythm. The clavicle is seen to be raised, rotated in a posterior position and protracted slightly for allowing the mobility of the AC joint (Ratanapinunchai, Mathiyakom & Sungkarat, 2019). At nearly 145º position, the humerus rotates externally for availing increased tuberosity from the lower side of the acromion process. The 180º of abduction is regarded as the end range of movement (Lawrence et al. 2017).

Shoulder Condition
Internal Impingement
Shoulder Impingement Syndrome (SIS) is regarded as one of the main causes of shoulder movement issues and it is defined as the condition in which disabling contact forms between bony structures and soft tissues in the shoulder area (Ettinger et al. 2017). The SIS mainly develops due to wear and tear of muscles and friction of bones caused as a result of repetitive tasks executed by labourers, swimmer and others. The SIS is of four types which include subacromial impingement syndrome, internal impingement syndrome, coracoids impingement and suprascapular nerve impingement (Fong et al. 2019). The Internal Impingement is the condition in which infraspinatus tendon and supraspinatus tendon present on the posterosuperior portion of the glenoid labrum is pinched or rubbed (Charalambous, 2019). The mechanism of internal impingement mentions that it occurs in case of maximum abduction of the arm and external rotation that happens during late cocking as well as early acceleration phase developed for throwing something with the arm (Corpus et al. 2016). This means that the impingement mainly happens when the arm is elevated during external rotation.
The repetitive impingement of the lower surface present behind the supraspinatus tendon leads to increased tuberosity making individuals face internal impingement. The humeral pathological micromotion allows the rotator cuff muscles to become impinged between the glenoid and humeral head that leads to the development of pain related to the internal impingement. This happens when humeral shaft proceeds posteriorly above the plane of the scapula during throwing and cocking position (Shah, Horsley & Rolf, 2017). During cocking phase to throw anything, the in internal impingement the scapula and the humeral shaft shows failure to remain in the same plane leads to encroachment of rotator cuff tendons present between the rim of the glenoid and head of the humerus (Chelli et al. 2019). The Internal Impingement is mainly seen among overhead sport athletes who are involved in cricket, basketball, tennis and others. The key symptom seen in internal impingement is pain experienced in the posterior region of the shoulder. The athletes tend to experience this pain in this type of impingement during the late cocking-phase of throwing making them face difficulty to warm up. The other symptoms of the impingement include failure to make internal rotation during the phase of 90º abduction (Peduzzi et al. 2019).
Intervention
A chiropractor is referred to the practitioner who uses complementary medicine for the basis of diagnosis and treatment of the misaligned joints. They usually provide hand-on spinal manipulation along with other nature of alternative intervention with the intention to ensure proper alignment of the musculoskeletal structure of the body to enable the person to get healed without medication or surgery (Emary & Taylor, 2016). The chiropractor can take various interventions to resolve and manage internal impingement among individuals. The stretching techniques which focus on raising the flexibility of the soft tissues present on the posterior shoulder area to be commonly implemented by the chiropractor (Thiruvarangan, Srigrishna, & Saravanan, 2019). The sleeper stretch is one the intervention that is to be performed by the chiropractor where they would make the patient lie on their injured side on the bed with the shoulder fixed in a 90º forward flexion with the scapula fixed manually to be retracted while passive internal rotation of the glenohumeral is performed. This would lead the individual experience stretch in the lower part of the shoulder and not in the upper part and by executing it would lower their rotation and intensity of the trunk to be backed slightly, in turn, reducing the intensity of the stretch (Reuther et al. 2016).
The cross-body stretch is another technique applied by a chiropractor for the lower capsule and it can be executed by the movement of the arm in horizontal position. The cross-body along with sleeper stretch is recommended by chiropractor in this condition as it leads to improve tissue flexibility and improve internal rotation of the glenohumeral joint along with horizontal adduction motion range in case of the overhead athlete (Vincent and Vincent, 2018). The grade IV along with dorsal glide mobilisations is executed with the supine of the patients by making their shoulder placed by the chiropractor in 90 abductions (Corpus et al. 2016). The GH anterior-posterior mobilisation of the joint is used by a chiropractor for stretching the posterior capsule and improving internal rotation but in case of instability is seen they are avoided for the treatment of internal impingement (Mine et al. 2017).

Conclusion
The Internal Impingement mainly occurs when the movement of the arm leads to impingement of rotator cuff between the posterosuperior and the humeral head of the rim of the glenoid. This nature of impingement leads to wear and tear of the rotator cuff of the glenoid labrum and it is hypothesised that laxity of the joints also leads to the internal impingement. The cross-body stretch, sleeper stretch, end-range mobilisation and others are used by chiropractor as intervention to manage internal impingement.
Discover additional insights on Challenges in Primary Mental Health Diagnosis by navigating to our other resources hub.
References
Charalambous, C.P., 2019. Shoulder Internal Impingement. In The Shoulder Made Easy. Springer, Cham.
Chelli, M., Grimberg, J., Lefebvre, Y., Peduzzi, L., Hardy, A., Sanchez, M., Holzer, N., Garret, J., Bertiaux, S., Kany, J. & Levigne, C., (2019). Internal impingement of the shoulder: An international survey of 261 orthopaedic surgeons. Orthopaedics & Traumatology: Surgery & Research, 105(8), 207-212.
Corpus, K.T., Camp, C.L., Dines, D.M., Altchek, D.W. and Dines, J.S., (2016). Evaluation and treatment of internal impingement of the shoulder in overhead athletes. World journal of orthopedics, 7(12), 776.
Corpus, K.T., Camp, C.L., Dines, D.M., Altchek, D.W. & Dines, J.S., (2016). Evaluation and treatment of internal impingement of the shoulder in overhead athletes. World journal of orthopedics, 7(12), 776.
Emary, P.C. & Taylor, J.A., (2016). Advanced hip joint degeneration associated with femoroacetabular impingement in a retired chiropractor. The Journal of the Canadian Chiropractic Association, 60(3), 260.
Ettinger, L.R., Shapiro, M. & Karduna, A., (2017). Subacromial anesthetics increase proprioceptive deficit in the shoulder and elbow in patients with subacromial impingement syndrome. Clinical Medicine Insights: Arthritis and Musculoskeletal Disorders, 10, 1179544117713196.
Fong, S.M., Ng, L.K., Ma, W.W., Wang, H.K., Bae, Y.H., Yam, T.T., Kam, W.K. & Chung, W.Y., (2019). Effects of kinesiology taping on shoulder girdle muscle activity and sports performance during badminton forehand overhead strokes in amateur badminton players with shoulder impingement syndrome. The Journal of sports medicine and physical fitness, 59(6), pp.994-1000.
Joseph, S.Y., (2019). Imaging Diagnosis of Shoulder Girdle Fractures. In The Shoulder. Springer, Cham.
Kim, B. & Deshpande, A.D., (2017). An upper-body rehabilitation exoskeleton Harmony with an anatomical shoulder mechanism: Design, modeling, control, and performance evaluation. The International Journal of Robotics Research, 36(4), 414-435.
Lawrence, R.L., Schlangen, D.M., Schneider, K.A., Schoenecker, J., Senger, A.L., Starr, W.C., Staker, J.L., Ellermann, J.M., Braman, J.P. & Ludewig, P.M., (2017). Effect of glenohumeral elevation on subacromial supraspinatus compression risk during simulated reaching. Journal of Orthopaedic Research, 35(10), 2329-2337.
Ludewig, P.M. & Lawrence, R.L., (2017). Mechanics of the Scapula in Shoulder Function and Dysfunction. In Disorders of the Scapula and Their Role in Shoulder Injury. Springer, Cham.
MacDonald, K., Bridger, J., Cash, C., & Parkin, I. (2007). Transverse humeral ligament: Does it exist? Clinical Anatomy, 20(6), 663–667.
Mine, K., Nakayama, T., Milanese, S. & Grimmer, K., (2017). Effectiveness of stretching on posterior shoulder tightness and glenohumeral internal-rotation deficit: a systematic review of randomized controlled trials. Journal of sport rehabilitation, 26(4), 294-305.
Niyetkaliyev, A.S., Hussain, S., Jamwal, P.K. & Alici, G., (2017). Modelling of the human shoulder girdle as a 6-4 parallel mechanism with a moving scapulothoracic joint. Mechanism and Machine Theory, 118, 219-230.
Peduzzi, L., Grimberg, J., Chelli, M., Lefebvre, Y., Levigne, C., Kany, J., Clavert, P., Bertiaux, S., Garret, J., Hardy, A. & Holzer, N., (2019). Internal impingement of the shoulder in overhead athletes: Retrospective multicentre study in 135 arthroscopically-treated patients. Orthopaedics & Traumatology: Surgery & Research, 105(8), 201-206.
Qu, Y.Z., Xia, T., Liu, G.H., Zhou, W., Mi, B.B., Liu, J. and Guo, X.D., (2019). Treatment of Anterior Sternoclavicular Joint Dislocation with Acromioclavicular Joint Hook Plate. Orthopaedic surgery, 11(1), 91-96.
Ratanapinunchai, J., Mathiyakom, W. & Sungkarat, S., (2019). Scapular Upward Rotation During Passive Humeral Abduction in Individuals With Hemiplegia Post-stroke. Annals of rehabilitation medicine, 43(2),178.
Reuther, K.E., Larsen, R., Kuhn, P.D., Kelly IV, J.D. & Thomas, S.J., (2016). Sleeper stretch accelerates recovery of glenohumeral internal rotation after pitching. Journal of shoulder and elbow surgery, 25(12), 1925-1929.
Shah, S.R., Horsley, I. & Rolf, C.G., (2017). Anterior internal impingement of the shoulder in rugby players and other overhead athletes. Asia-Pacific journal of sports medicine, arthroscopy, rehabilitation and technology, 8, 13-17.
Shehadeh, A., Ja’afar, A., Isleem, U., Hamad, A. & Salem, A., (2019). Shoulder girdle resection: surgical technique modification and introduction of a new classification system. World journal of surgical oncology, 17(1), 107.
Thiruvarangan, S., Srigrishna, P. & Saravanan, V., (2019). Conservative Approach for Restoring Subacromial Impingement Syndrome. SM J Orthop, 5(1), 1067.
Tunstall R. (2015), Gray's Anatomy; The anatomical Basis of Clinical Practice, 42 edn, Elsevier.
Umehara, J., Nakamura, M., Fujita, K., Kusano, K., Nishishita, S., Araki, K., Tanaka, H., Yanase, K. & Ichihashi, N., (2017). Shoulder horizontal abduction stretching effectively increases shear elastic modulus of pectoralis minor muscle. Journal of shoulder and elbow surgery, 26(7), 1159-1165.
Vincent, H.K. & Vincent, K.R., (2018). Cross Body Stretching for Internal Rotation Deficit. Current sports medicine reports, 17(3), 82.
Zheng, M., Zou, Z., Bartolo, P.J.D.S., Peach, C. & Ren, L., (2017). Finite element models of the human shoulder complex: a review of their clinical implications and modelling techniques. International journal for numerical methods in biomedical engineering, 33(2), 02777.



- 24/7 Customer Support
- 100% Customer Satisfaction
- No Privacy Violation
- Quick Services
- Subject Experts