UK Carbohydrate Intake and Health
Project Rationale:
The dietary recommended value in the United Kingdom of for total carbohydrate, free sugars and starch should be maintained to ensure a healthy weight which is 50% of the total dietary energy intake (Scientific Advisory Committee on Nutrition, 2015) (need ref??). It is also recommended that average intake of free sugars should not cross the level of 5% of the total dietary energy as mentioned for the age group 2 years and above (Scientific Advisory Committee on Nutrition, 2015) (need ref??). The guideline recommended the intake of saturated fat to be 20gms for women and 30gms for men (Scientific Advisory Committee on Nutrition, 2015). A survey on the nutritional consumption trend of the individuals of age in between 19-64 years in the UK highlighted that a median of 271gms and 248gms of carbohydrate consumption was observed within 2000 -2001 and 2008 -2009 respectively (Whitton, et al, 2011) (what survey?? REF). This survey was conducted to investigate about the food consumption pattern and nutritional status of the UK population. No significant changes were observed in the median of daily food consumption or energy intake in the form of carbohydrate or fat based on sex and age group in between the two surveys conducted. Similarly for protein the median value observed was 86.6gms and 88.8gms and for saturated fats it was 30.7gms and 29.2 gms respectively (Whitton, et al, 2011). (remove to focus on carbs?? & state significance, eg. increase/ decrease compared to past) The concept of a low carbohydrate diet is based on the hypothesis that a reduction in the production of the critical hormone insulin from due to decreased carbohydrate consumption results in anabolic process, stores fat, enhanced fat catabolism at adipocytes and improved the cardiometabolic functions and also helps in loss of weight thus is effective for weight loss. Therefore, this particular approach has been recently referred to termed as the “carbohydrate insulin model” (Oh, 2020). Several evidences studies have considered suggested that the low carb diet is considered to be advanced superior to other models of diet dietary models in terms of quick its weight loss potential within the initial 6 -12 months of intake assessed 6-12 months (Nordmann, et al, 2006; Bueno, et al, 2013; Tobias, et al, 2015). However, When there is deficiency in the carbohydrate intake, the compensation is made with the intake of macronutrient such as fat and protein. However, during periods of carbohydrate insufficiency, caloric compensation is fulfilled by the intakes of macronutrients such as fat and protein. Thus, this particular model of diet is subjectable to question as the induction of weight loss occurs because of can be directly correlated to a deficiency in the calorie intake (i rearranged the order, i think it makes more sense and flows better)

A hypothesis that offers a suitable answer to the issue is that primary consumption of fat and protein in a low carbohydrate diet enhances the satiety level satiety and results in the is responsible for the associated hypoglycemia. The combined effect of These two factors mutually decreases the hunger level appetite and eventually, and hence the overall intake of food resulting in deficiency of calorie calorie deficit. On the contrary, another hypothesis states that a low carbohydrate diet is implied to an increased metabolic burn utilization in comparison to a diet high in carbohydrate. The study also highlights that this type of diet burns about 200-300 calories in comparison to the iso-caloric high carbohydrate diet (Ebbeling, et al, 2018; Ebbeling, et al, 2012). The existing theories are not definite and also controversial in nature. So further research is required to confirm the facts.(so what??) In this respect, special mention about the ketogenic diet should be discussed because it is a special category of low carb diet in which carbohydrate intake is further restricted. This form of diet limits the intake of carbohydrate to 25 – 50gms daily (need ref??) which eventually results in nutritional ketosis(Paoli, et al, 2013). The mechanism of mechanistic workings of ketogenic diet is that the limit of carbohydrate intake to below 50 gms causes exhaustion of glycogen stores and production of ketones because the deposited fat is mobilized within the adipose tissue. Nutritional ketosis enhances the serum level of ketones (from 1 mmol/L to 7 mmol/L) but does not induce metabolic acidosis. (so what? How does having more ketones benefit us?) The benefits associated with keto diet are weight loss, lowers the risk of certain cancers, reduces the cholesterol level which in turn lowers the risk of developing cardiovascular disease, provides neuroprotective benefits and also reduces the episodes of seizures in epilepsy (Paoli, et al, 2013). However, there are certain adverse outcomes of low carb diet such as weakening of muscles, tiredness, dehydration which affects the physical activity more stressful, increased mortality rate and concern regarding to the renal function (Paoli, et al, 2013).
Continue your exploration of Healthy Aging Policies in the UK with our related content.
The clinical significance of low carbohydrate diet:
Cardiovascular diseases:
The effect of a low carb diet on cardiovascular diseases is controversial. Although a Though few studies had revealed that the application of a low carb diet is associated with increased LDL cholesterol levels (I changed the order & some plurals), several (no repeat) studies reported negligible effects. Similarly, the intake of a low carb diet may increase HDL and impact the other metabolic parameters. Moreover, with the increased intake of fat amongst the UK population, especially saturated fat (+REF?), has been associated with the increasing concentrations of lipid in their plasma (Dehghan, et al, 2017). According to the statistical records obtained from the British Heart Foundation, UK, 2020 7.4 million people are residing with heart and circulatory disease (Dehghan, et al, 2017; Noto, et al, 2013; British Heart Foundation, UK, 2020; Bhatnagar, et al, 2016). Therefore, individuals may suffer from adverse health effects from the intake of a low carb diet with in an attempt to lose weight. (This sentence is swapped with the prior below sentence, I think it makes more sense to give context first w/ stats, and it also gives a conclusive answer to the paragraph.)
Type 2 diabetes (T2D):
More than 90% of the individuals in the UK suffer from T2D and 8% of the individuals suffer from type 1 diabetes (Tay, et al, 2018; Ajala, et al, 2013).Without the use of medications, the approach of carbohydrate control was considered to be playing the major factor in the aspect monitoring carbohydrate intake is crucial in the management of glycaemic control in both type 1 and 2 diabetes. It is evident that the intake of dietary carbohydrates enhances the insulin demands and with, thus the a reduction of carbohydrate consumption can effectively improves reduce the blood sugar levels. Although there is evidence available concerning the appropriate reduction reduction intake?? of insulin, haemoglobin A1c and oral medication with the approach of when abiding a ketogenic diet, adherence to when this intervention must be adhered to andwas continued for a period of 12 months. (swapped some sentences around for understanding) The study highlighted that the markers associated with the cardiometabolic risk factors had also improved (Bhanpuri, et al, 2018). Therefore medical nutrition therapy has been included as an option in the current guidelines to control diabetes. (This sentence is definitely relevant, but im not sure what reference you are referring to? +REF?? and currently doesn't link well with the previous sentence & as well last statistical figure). More than 90% of the individuals in the UK suffer from T2D and 8% of the individuals suffer from type 1 diabetes (Tay, et al, 2018; Ajala, et al, 2013). (+concluding/ summarizing sentence? Similar to above, etc. therefore…)
Renal Function:
Low carb diets with potentially high intake of protein protein intakes have concerns regarding the functioning of renal function as it consistently increase the glomerular pressure and hyperfiltration (Martin, et al, 2005). (+How?) On the contrary, athletes must intake should consume a high protein diet to optimize the protein synthesis for in muscles (1.6 gm/kg) and for endurance sports (0.8 gm/kg). The high protein intake supports the physical activity and also augments the compositions of body and metabolic adaptations. The intake of the diet by the athletes helps them to retain muscle mass while losing body fat and weight. The performance level and fat free mass should be preserved among athletes to minimize the weekly weight loss (Thomas, et al, 2016).(positively or negatively? Explain more maybe??) Moreover, although there is no evidence that has been correlates with a high protein load with worsening conditions of kidney deteriorated kidney function from the normal operational state, patients with chronic kidney disease may be recommended with a very low protein diet (0.2-0.8 gm/kg/day) to prevent the further worsening of kidney any further decline in kidney function (Hahn, et al, 2018; Morton, et al, 2018). (The info is the same, but is made more compact??) Therefore, further research should be conducted on the impact of this type of ketogenic (specific is good) diet on several biomarkers such as lipids, resistance to insulin, metabolism of liver, gut hormones, inflammation and glycaemia to evaluate the prolonged outcomes on human health Moreover, future research should also (repetition on further research) and address the recommendations for the individualised nutritional intake.
Research Questions:
To what extent is the ketogenic diet related to the management of diabetes, cardiovascular indicators and other health indicators? = anson’s suggested
Research Hypothesis:
H0: The low carb diet does not show any effect on the health indicators in the management of cardiovascular disease and diabetes
H1:The low carb diet shows has an effect on the health indicators in the management of cardiovascular disease and diabetes
Recruitment Methods:
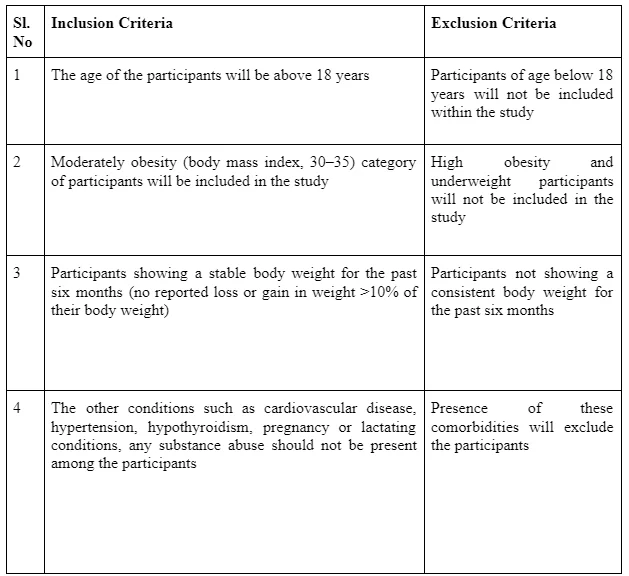
A randomised control trial will be conducted for comparing to compare the effect of a low carbohydrate diet to a normal isocaloric diet. (+ what is the normal diet, eg. isocaloric??) Two groups will be assigned both including a minimum of 10 numbers of adult participants: 1) Low carbohydrate diet group and 2) isocaloricNormal diet group or Control Group. The subjects will be recruited by advertisement or by conducting telephonic survey.(Do we need to worry about if this study is sufficiently powered? Ie. how did we get the number 10 participants) A low carbohydrate diet (a maximum intake of 60gms of carbohydrate per day) without having any restrictions on the energy intake will be followed by the participants. The trials will report the impact of this diet on parameters such as body weight, level of low density lipoprotein (LDL) cholesterol and plasma glucose level of the participants of both the group. Data from the eligible trials will be extracted in duplicates to ensure the reproducibility of the results. The main endpoint will be considered as the mean difference between the parameters from the baseline to 3 months and 6 months of follow up (Brehm, et al, 2003).
Experimental Design and Data Collection and Methods:
The data quality will be assessed based on the blinded outcome assessment, loss to follow up, the full description of the losses that occurred during the follow-up and due to the withdrawal of the participants. This type of trials requires an open intervention where no blinding of the trial participants and the investigators will be allowed. Subjects will be screened based on the medical history and measurements of the height, weight, fasting glucose, blood pressure (BP), LDL and HDL cholesterol. Individuals who will meet the criteria for the study will be enrolled in the study. Each of these measurements of the above parameters will be repeated after 3 months and 6 months of study. The blood cholesterol level (LDL and HDL), blood glucose (fasting) will be measured using the dual-energy x-ray absorptiometry (DEXA) total body scanner. The BP will be measured using auscultation method with an appropriate size cuff after allowing the participants to seat and rest for some time along with the other necessary interventions. The height and weight of the patient will be measured using the standard instruments respectively. The results of the biochemical analysis will be conducted by blinded personnel to the group assignment of the subjects (Brehm, et al, 2003; Nordmann, et al, 2006). Statistical analysis of the data will be conducted using Microsoft Excel, 2013. The data will be represented as the mean with SE (standard error).
Data Management Plan:
The data management involves the supervision and administration of the task concerning the documentation, transfer and preparation of the source data. The administrative process involves acquiring, authenticating, storing under the protection of the concerned data to ensure the principles of accessibility, reliability and timelessness for the data users. In the United Kingdom, the data of basic research are generally stored for a period of minimum 10 years. Otherwise, research records are maintained for a minimum period of three years. The data will be maintained in the electronic software with password system to restrict the access or it will be stored within the locked cabinet within a secured building. The process ensures the appropriate safety of the personalised data of the participants from the unauthorised access of the person, unlawful processing of the data, accidental loss or damage or destruction of the data. The statement of purpose should fulfil the justification as per the Data Protection Act, 2018 for the sharing of data (Chassang, et al, 2017; Data Protection Act, 2018).
Ethical Considerations for the study:
Participation and Informed Consent:
Informed consent will be obtained from all the participants before the study. It is a voluntary agreement for participation in the research. While obtaining the consent the participants will be informed about their rights of withdrawal at any step of the study without any fee, about the aim of the study, the procedures that will be involved within-study and the possible risks or benefits that are related with their participation (Nardini, et al, 2014).
Randomisation and blinding
Randomisation will be used in the study to prevent any selection bias and the other confounding factors within the study. Blinding will further reduce the opportunity for the introduction of bias within the study after the application of intervention (Nardini, et al, 2014).
Privacy and Confidentiality of the Participants:
The participant’s privacy will be respected by safeguarding the information and respect will be ensured between the participants and the researcher throughout the study even if the participant wants to leave the study at any step. The researcher will maintain the confidentiality of the personal information of the participants by using code to identify the identity of results which will maintain the process of anonymity (Nardini, et al, 2014).

Protection from overexploitation of the participants:
It states that the wellbeing of the participants should be considered above all the research interest. Providing the adequate level of protection which can be considered as a global standard is challenging within medical research. Moreover, the level of protection offered by the current guidelines shall not collide with the individual choices of the participants (Nardini, et al, 2014).
Dissemination:
The study will include the participants on a randomised basis based on the above-mentioned inclusion and exclusion criteria so that it represents the healthy general population. Therefore, the findings of the data may be extended to healthy subjects with careful investigation. The study cannot be established for those individuals who are suffering from any associated comorbidities. The data findings can be used by the other researchers conducting any similar research in future so that they also conduct a critical analysis of the data. The data findings will also be published in national or international peer-reviewed journals or will be presented in conferences or meetings of professional associations. This is an important part of the study as it is done with a hope that individuals within an organisation will improve their knowledge and therefore will be able to make better decisions in future (Dobbins, et al, 2010).
References:
Nordmann, A.J., Nordmann, A., Briel, M., Keller, U., Yancy, W.S., Brehm, B.J. and Bucher, H.C., 2006. Effects of low-carbohydrate vs low-fat diets on weight loss and cardiovascular risk factors: a meta-analysis of randomized controlled trials. Archives of internal medicine, 166(3), pp.285-293.
Bueno, N.B., de Melo, I.S.V., de Oliveira, S.L. and da Rocha Ataide, T., 2013. Very-low-carbohydrate ketogenic diet v. low-fat diet for long-term weight loss: a meta-analysis of randomised controlled trials. British Journal of Nutrition, 110(7), pp.1178-1187.
Tobias, D.K., Chen, M., Manson, J.E., Ludwig, D.S., Willett, W. and Hu, F.B., 2015. Effect of low-fat diet interventions versus other diet interventions on long-term weight change in adults: a systematic review and meta-analysis. The lancet Diabetes & endocrinology, 3(12), pp.968-979.
Ebbeling, C.B., Feldman, H.A., Klein, G.L., Wong, J.M., Bielak, L., Steltz, S.K., Luoto, P.K., Wolfe, R.R., Wong, W.W. and Ludwig, D.S., 2018. Effects of a low carbohydrate diet on energy expenditure during weight loss maintenance: randomized trial. bmj, 363.
Ebbeling, C.B., Swain, J.F., Feldman, H.A., Wong, W.W., Hachey, D.L., Garcia-Lago, E. and Ludwig, D.S., 2012. Effects of dietary composition on energy expenditure during weight-loss maintenance. Jama, 307(24), pp.2627-2634.
Paoli, A., Rubini, A., Volek, J.S. and Grimaldi, K.A., 2013. Beyond weight loss: a review of the therapeutic uses of very-low-carbohydrate (ketogenic) diets. European journal of clinical nutrition, 67(8), pp.789-796.
Dehghan, M., Mente, A., Zhang, X., Swaminathan, S., Li, W., Mohan, V., Iqbal, R., Kumar, R., Wentzel-Viljoen, E., Rosengren, A. and Amma, L.I., 2017. Associations of fats and carbohydrate intake with cardiovascular disease and mortality in 18 countries from five continents (PURE): a prospective cohort study. The Lancet, 390(10107), pp.2050-2062.
Tay, J., Thompson, C.H., Luscombe‐Marsh, N.D., Wycherley, T.P., Noakes, M., Buckley, J.D., Wittert, G.A., Yancy Jr, W.S. and Brinkworth, G.D., 2018. Effects of an energy‐restricted low‐carbohydrate, high unsaturated fat/low saturated fat diet versus a high‐carbohydrate, low‐fat diet in type 2 diabetes: a 2‐year randomized clinical trial. Diabetes, Obesity and Metabolism, 20(4), pp.858-871.
Brehm, B.J., Seeley, R.J., Daniels, S.R. and D’Alessio, D.A., 2003. A randomized trial comparing a very low carbohydrate diet and a calorie-restricted low fat diet on body weight and cardiovascular risk factors in healthy women. The Journal of Clinical Endocrinology & Metabolism, 88(4), pp.1617-1623.
Nordmann, A.J., Nordmann, A., Briel, M., Keller, U., Yancy, W.S., Brehm, B.J. and Bucher, H.C., 2006. Effects of low-carbohydrate vs low-fat diets on weight loss and cardiovascular risk factors: a meta-analysis of randomized controlled trials. Archives of internal medicine, 166(3), pp.285-293.
Dobbins, M., DeCorby, K. and Robeson, P., 2010. Dissemination and use of research evidence for policy and practice. Models and frameworks for implementing evidencebased practice: Linking evidence to action, pp.147-167.
Whitton, C., Nicholson, S.K., Roberts, C., Prynne, C.J., Pot, G.K., Olson, A., Fitt, E., Cole, D., Teucher, B., Bates, B. and Henderson, H., 2011. National Diet and Nutrition Survey: UK food consumption and nutrient intakes from the first year of the rolling programme and comparisons with previous surveys. British journal of nutrition, 106(12), pp.1899-1914.
Morton, R.W., Murphy, K.T., McKellar, S.R., Schoenfeld, B.J., Henselmans, M., Helms, E., Aragon, A.A., Devries, M.C., Banfield, L., Krieger, J.W. and Phillips, S.M., 2018. A systematic review, meta-analysis and meta-regression of the effect of protein supplementation on resistance training-induced gains in muscle mass and strength in healthy adults. Br J Sports Med, 52(6), pp.376-384.
Bhanpuri, N.H., Hallberg, S.J., Williams, P.T., McKenzie, A.L., Ballard, K.D., Campbell, W.W., McCarter, J.P., Phinney, S.D. and Volek, J.S., 2018. Cardiovascular disease risk factor responses to a type 2 diabetes care model including nutritional ketosis induced by sustained carbohydrate restriction at 1 year: an open label, non-randomized, controlled study. Cardiovascular diabetology, 17(1), p.56.
Thomas, D.T., Erdman, K.A. and Burke, L.M., 2016. Nutrition and athletic performance. Med. Sci. Sports Exerc, 48, pp.543-568.



- 24/7 Customer Support
- 100% Customer Satisfaction
- No Privacy Violation
- Quick Services
- Subject Experts