Biomarkers in Detecting Fetal Brain Damage
Chapter 1: Introduction
1.1 Background information
For the past 10 years, researchers have invested significant resources in extracting the next generation of the blood biomarkers. Research has it that over 1.15 million babies have developed hypoxic-ischemic encephalopathy (HIE) on annual basis. Almost 60% of the infants having HIE eventually die as a result of the severe disabilities the moment they hit the age of 2 years (Graham et al., 2016). The most common complications include epilepsy, mental retardation and cerebral palsy. The greatest challenge, however, lies behind the perinatal medicine utilized when assessing the fetus. Therefore, Early diagnosis of fetuses with brain damage would provide for the opportunity of early intervention, possibly leading to improved cognitive and motor outcomes for the neonate (Spittle, Orton et al. 2015). So, identifying biomarkers that can provide a sign that the fetus is experiencing complications prior to birth is essential to assist in early detection (Douglas-Escobar and Weiss 2013). The greatest value would be the identification of biomarkers in the mother that can signal impending or actual fetal brain damage (Douglas-Escobar and Weiss 2013). Hence, this study finds a gap of identifying new methods of finding biomarkers and metabolic signatures such as metabolomics. Today, if a biomarker is identified, it would give room for early intervention immediately after birth.
1.2 Aims and Hypothesis
The aim of this research is to conduct a systematic evaluation of the evidence for the use of maternal biomarkers; S100β, carbonic anhydrase, kynurenine, and fetal cells as diagnostic tools for fetal brain damage. The overall hypothesis is that maternal blood carries a biological signature (biomarker) of fetal brain damage.

Chapter 2: Systematic Literature Review
Part 1: Biomarkers
2.1 Defining Biomarkers
Biomarkers are a subcategory of medical signs that can be observed in patients, either from outward signs or simple biological samples (Strimbu and Tavel 2010). A clinically valid and reliable biomarker must be able to produce consistent results across a range of patients (Holland 2016). This includes being cost-effective and culturally acceptable allowing them to be sampled across a variety of different socioeconomic and cultural settings (Holland 2016).
Maternal-Fetal Biomarkers
For clinical detection of fetal abnormalities, there is a disadvantage that fetal cells have to be sampled invasively from the placenta (e.g., chorionic villus sampling [CVS]); amniotic fluid (amniocentesis), or fetal blood sampled from the umbilical cord (Irwin 2014), all of which increases the risk of miscarriage (Irwin 2014). Yet, false positives may occur from maternal cell contamination (Tabor and Alfirevic 2010). Furthermore, mid-trimester amniocentesis is known to augment the incidence of neonatal respiratory distress syndrome and congenital pneumonia (Tabor and Alfirevic 2010). Nevertheless, early amniocentesis increases risk of developing talipes equinovarus, a birth defect in which the foot is twisted out of shape due to a reduction in amniotic fluid (Tabor and Alfirevic 2010). Moreover, risks of musculoskeletal deformities may be amplified in cases where amniocentesis was performed before 14 weeks of gestation (Tabor and Alfirevic 2010). CVS has also been associated with limb defects and placental disruption (Tabor and Alfirevic 2010). Therefore, alternative methods such as the use of maternal biomarkers are required (Midgley, Niswender et al. 1969). The following Table gives an overview of the key characteristics of clinically valuable biomarkers.

2.2 Techniques Commonly Used in the Identification of Biomarkers
There are two main techniques which are used in the identification of biomarkers: Proteomics and Metabolomics (Sahab, Semaan et al. 2007). Each of these should be considered when investigating potential biomarkers for use in early fetal brain damage detection and are therefore explored below.
Proteomics
Proteomics involves separating and identifying proteins from crude biological samples (Sahab, Semaan et al. 2007). The identification of differentially expressed proteins between two samples in differing conditions allows for characterization of biological roles, clarification of biological mechanisms, and discovery of therapeutic targets and biomarkers (Sahab, Semaan et al. 2007). Proteins can be discovered by using electrophoresis and chromatography for the separation of proteins, followed by evaluation via mass spectrometry to identify each specific protein (Sahab, Semaan et al. 2007).
Metabolomics
Metabolomics refers to phenotypic analysis of metabolites of an isolated organism, cell system, or biological fluid (Monteiro, Carvalho et al. 2013). It is based on presumptions that some diseases alter biochemical reactions, producing an array of changes in individual metabolites that serve as markers (Monteiro, Carvalho et al. 2013). Metabolomics require nuclear magnetic resonance spectroscopy and mass spectrometry (Monteiro, Carvalho et al. 2013).
Part 2: Causes of Fetal Brain Damage
Intrauterine Growth Restriction
Intrauterine Growth Restriction (IUGR) is frequently associated with peri-natal brain damage. IUGR refers to the inability of the fetus to reach its genetic growth potential (Vandenbosche and Kirchner 1998). This is commonly caused by poor maternal nutrition, placental insufficiency, and/or lack of adequate oxygen supply to the fetus (Vandenbosche and Kirchner 1998). Of the 4 million neonatal mortalities, approximately 60% are associated with low birth weight (LBW), many of which can be attributed to IUGR (Lawn, Cousens et al.).
Causes of hypoxic-ischemic brain lesions in neonates
Acute hypoxic-ischemic brain lesions in neonates originate through a reduction of blood flow in the uterine or umbilical circulations, which render the fetus hypoxic (Parer 1980). When the oxygen deprivation becomes severe, fetal metabolism changes from aerobic to anaerobic, this results in the accumulation of lactic acid, and free radicals of oxygen and nitrogen which are highly cyto-toxic (Berger and Garnier 1999). Acute fetal hypoxia may also rise from abruption (i.e. partial separation) of the placenta from the uterine wall, prolonged contraction of the uterus, maternal vena cava occlusion syndrome, or compression of the umbilical cord (Parer 1980).
Fetal cardiovascular response to hypoxia
When the fetus is exposed to hypoxia, fetal breathing movements cease and heart rate falls (Giussani 2016). Both responses enable a decrease in oxygen consumption and lessen the fetal demand for oxygen, and are thereby adaptive (Giussani 2016). Reduction in heart rate slows end-diastolic filling, increases end-diastolic volume, and allows for the maintenance of cardiac output and perfusion pressure despite the presence of bradycardia (Giussani 2016). Consequent increases of ventricular stretch will enhance sarcomere length, tension, and contractility through the Frank-Starling Mechanism (Giussani 2016). As a result, left and right ventricular stroke volumes are relatively maintained in the presence of increases in after-load, with the left ventricle having an increased reserve capacity for increases in after-load (Giussani 2016). Although there are compensatory mechanisms such as elevations in pre-load and ventricular pressure in the fetus, the Frank-Starling mechanism is limited for increasing cardiac output above baseline levels (Giussani 2016). This is due to the fact that the fetal blood volume (~120 ml/kg) is high compared to postnatal life (Dawes 1968), so that ventricular volume is high and close to the maximum of ventricular function curve. This limits the degree to which increases in ventricular stroke volume can lead to a rise in end-diastolic filling pressure (Giussani 2016). However, the decrease in fetal heart rate can slow down the passage of blood flow through the systemic circulation, increasing the time available for gas exchange in essential vascular beds (Giussani 2016).
Circulatory centralization and cerebral perfusion
It has long been known that an acute decrease in arterial oxygen saturation in the late gestation fetus triggers a sympathetic nervous system response, which serves to redistribute blood flow to central organs such as the brain, heart, and adrenal glands (Dawes 1968). The consequence is that blood volume (and flow) is shifted away from the gut and the body (mainly, muscle) where vasoconstriction is most profound for the purposes of maintaining blood flow to the heart and brain where very little constriction occurs. If hypoxia is mild, cerebral flow is largely unchanged (Allison, L. Brain et al. 2016), except if hypoxia results in metabolic acidosis, cerebral hyper-perfusion can occur which can be further exacerbated by the post-asphyxial increase in cardiac output (Allison, L. Brain et al. 2016). This can lead to intra-cranial and/or intraventricular hemorrhage (IVH) (Allison, L. Brain et al. 2016). Initial hyper-perfusion of the brain is directly followed by a period of hypo-perfusion. Post-ischemic hypo-perfusion occurs through a dissociation of the CO2 cerebrovascular–reactivity from the auto-regulation of the cerebral vascular bed (Berger and Garnier 1999). This results in vasoconstriction and an uncoupling of blood flow and metabolic activity. This can also be caused by the production of oxygen radicals during the reperfusion phase following ischemia (Berger and Garnier 1999). A phenomenon known as no-reflow (also known as failure of reperfusion) can occur after severe cerebral ischemia (Ames, Wright et al. 1968). No-reflow in varying brain areas is a result of the greater viscosity of stagnant blood, compression of the smaller blood vessels through the swelling of the peri-ventricular glial cells, formation of endothelial microvilli, increased intra-cerebral pressure, post-ischemic arterial hypotension and heightened intravascular coagulation (Ames, Wright et al. 1968).
Energy metabolism and calcium homeostasis
Neural transmission of the electrical impulses and biosynthetic reactions require metabolism of glucose via the aerobic respiration pathway, whereby glucose is catabolized into two molecules of pyruvate (du Plessis 2009). Pyruvate is then broken down further through the citric acid cycle (du Plessis 2009). The release of electrons produces energy in the form of adenosine triphosphate (ATP) as they pass down the respiratory chain in mitochondria (du Plessis 2009). In mild hypoxemia, the fetus is able to conserve cerebral metabolic functions and adequate levels of intracellular ATP (Musaeva, Omarov et al. 1980). An acute reduction in the fetal oxygen supply will lead to a decrease in oxygen consumption in the cerebral cortex within minutes (Musaeva, Omarov et al. 1980), yet if this is prolonged ionic gradients (including Na+, K+, and Ca2+) can no longer be maintained due to the malfunction of the Na+/K+ pump through the lack of energy due to ATP depletion (Musaeva, Omarov et al. 1980). Energy depleted cells consume Na+ and consequent decrease in membrane potential causes an intake of Cl- ions (Musaeva, Omarov et al. 1980). Hence, intake of these two ions causes swelling of the cells as water travels through the cell via osmosis (Musaeva, Omarov et al. 1980). Lack of a membrane potential can cause elevated calcium levels in the cell and increased intracellular calcium concentrations can lead to cell damage by activating proteases, lipases, endonucleases, and induction of apoptosis (Berger and Garnier 1999). Some changes in the citric acid cycle also affect prostaglandin synthesis, gene expression, protein synthesis, increased free radical production and obstruction of axonal transport system via disintegration of microtubule (Berger and Garnier 1999). These metabolic changes can lead to brain damage, either before birth or during the birth process. The result is Neonatal Encephalopathy (NE).
Part 3: Maternal Biomarkers
2.3.1 Maternal S100β
S100β is an acidic calcium-binding protein located in glial cells, astrocytes, and in the villous and intermediate trophoblast cells of the human placenta (Gazzolo, Marinoni et al. 2006). At a micro-molar level, higher concentrations of extracellular S100β cause harmful effects in-vivo including enhancing the secretions of pro-inflammatory cytokines (Gazzolo, Marinoni et al. 2006). Additionally, it can cause apoptosis of astrocytic cells through activation of nitric oxide synthase (iNOS) and a subsequent production of nitric oxide (NO) (Garnier, Frigiola et al. 2009). Its low molecular weight means it can readily cross the placenta and travel into the maternal circulation (Gazzolo, Marinoni et al. 2006). Research has shown that higher maternal concentrations of S100β during the third trimester of pregnancy can lead to IUGR and IVH in the fetus (Gazzolo, Marinoni et al. 2006). IUGR and IVH are the results of hypoxic conditions, which suppress fetal neurological development (Gazzolo, Marinoni et al. 2006). Serum S100β values in healthy individuals range from 0.02 to 0.15 μg/L, as determined by immunoluminometric analytical methods (Ben Abdesselam, Vally et al. 2003)
2.3.2 Placental Carbonic Anhydrase
Carbonic Anhydrase (CA) is highly expressed in the placenta (Ridderstråle, Persson et al. 1997). It is an enzyme involved in inter-converting carbon dioxide (CO2) to bicarbonate (H2CO3) and, therefore, maintains acid-base equilibrium within the blood and tissue (Kaufmann, Mühlhauser et al. 1994). It also plays a major role in the removal of CO2 (Kaufmann, Mühlhauser et al. 1994). Severe hypocapnia (decreased CO2) and hypercapnia (increased CO2) can cause neonatal brain damage (Zhou and Liu 2008). Therefore, a question of interest is that whether placental CA protein expression is related to fetal brain damage, perhaps brought about by unphysiologic levels of severe hypocapnia and hypercapnia?
2.3.3 Placental Kynurenine
Kynurenine is a neuro-active metabolite that is derived from the amino acid, tryptophan (Opitz, Litzenburger et al. 2011). It is produced by the placenta under conditions of infection, inflammation, or severe hypoxia. Kynurenine itself is the substrate for the production of many other metabolites that are neurotoxic, the most important being quinolinic acid, all of which readily enter maternal and fetal blood (Manuelpillai, Ligam et al. 2004). This can cause infection-mediated fetal cerebral brain injury (Manuelpillai, Ligam et al. 2004). Hence, this raises the question as to whether a higher concentration of kynurenine or high placental expression of enzymes involved in tryptophan catabolism (including Indoleamine 2,3- dioxygenase and tryptophan 2,3 dioxygenase) during the infection can be used as a biochemical predictor of fetal brain injury (Notarangelo and Pocivavsek 2017).
2.3.4 Fetal Genes in Maternal Blood
Free cell fetal DNA has been identified in maternal blood (Kagan, Hoopmann et al. 2012). Therefore, by sequencing a maternal plasma DNA sample, it is possible to map out and determine the presence of fetal genetic mutations (Lo, Chan et al. 2010). This could lead to an early diagnosis and intervention including repairing the mutated DNA (Lo, Chan et al. 2010). However, in this project, we ask the question: does the amount of fetal cells or DNA in maternal blood relate to pregnancy outcomes that include adverse peri-natal neurological outcomes (Reitsma, Glas et al. 2005).
Chapter 3: Methodology
3.1 Search Strategy
Through background reading of the biomarkers, relevant search terms were selected. MeSH was also used for the understanding and retrieval of search terms. Two individuals then ran some test searches and recorded data in excel. This comprised of the category, concepts and related terms, and number of existing literature related to a particular term. They excluded duplicate terms. Results were refined and reviewed after discussions with a field specialist. Conversely, search terms varied according to the controlled vocabulary of individual databases (see Appendix 1 for the list of search terms). Databases including PubMed, Embase, CINAHL, Web of Science (BIOSIS), Scopus and Science Direct were searched. Proquest Thesis Dissertations and Thesis Global were also searched to include unpublished Thesis Dissertations. The full search strategy is documented as Appendix 2. Given time constraints and limited funding, the project management decided that it would be reasonable to focus specifically on S100β. This is because S100β presented the highest number of results on PubMed and demonstrated a high relevance to brain pathology (Malamitsi-Puchner 2010). Moreover, S100β originated in the placenta and can travel from the placenta into the maternal blood and therefore, abnormal levels could lead to perinatal brain damage (Marinoni 2002). Increases in S100β in the maternal circulation, in a compromised pregnancy where fetal brain damage is clearly evident (Gazzolo 2006).
3.2 Study Selection
Results were downloaded to the EndNote software for management. A single person reviewed and selected studies under the advice of field specialists. The first step after downloading and combining results from databases is the removal of duplicates. Then screening results based on title and abstract eliminated irrelevant literature. Relevant citations proceeded to the next stage of full-text retrieval and were screened against inclusion criteria. Inclusion criteria for S100β were studies that met all of the following criteria:
Are classified as case studies, cohort studies, case-control studies, and intervention studies. That measured S100β in the blood of the pregnant mother during their 1st, 2nd, or 3rd trimester at least once, yet one of those measures should have been measured in the 2nd or 3rd trimester. One of the measures for S100β should originate from the maternal side.
Other inclusion criteria were articles in English with no restriction on publication date. Animal studies, studies completed during delivery or after pregnancy, measured s100β via amniocentesis or chronic villus sampling, which sampled s100β in cord blood, explored the location of s100β in the placenta, and that were identified as conference abstracts were excluded. Of the 7085 articles, 4 were included.
3.3 Data Extraction
A single person conducted data extraction which was checked for accuracy by a field expert. Information on the study design, study setting, number of participants, trimester of time of study inclusion, age of mothers, country where study was conducted, the location of blood collection in the mother, statistical significance, and maternal S100β concentration for control and experimental groups was extracted.
3.4 Assessment of Methodological Quality
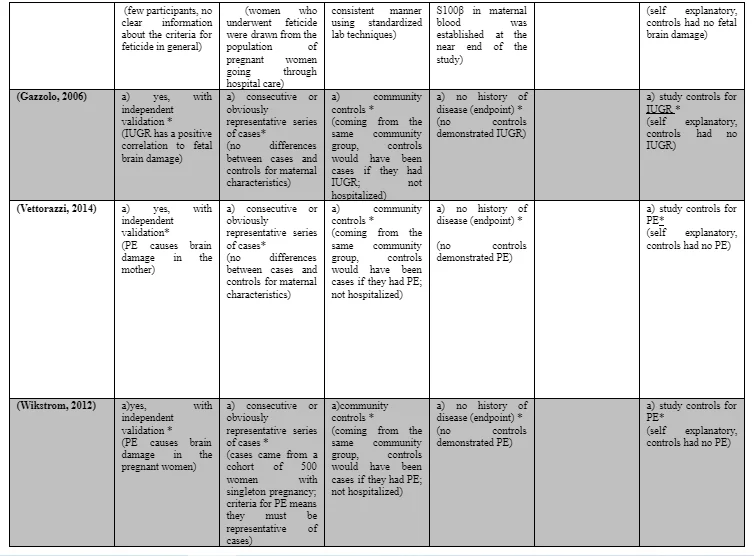
The Newcastle – Ottawa Scale was used to assess the quality of methodology for human studies (Deeks J 2003). Using this tool, each study was judged on eight items classified into three major groups; the selection of the study groups, the comparability of the groups, and the ascertainment of either the exposure or outcome of interest (Deeks J 2003). Stars were awarded for each quality item (Deeks J 2003). The highest qualities of studies are awarded up to nine stars (Deeks J 2003). This was deemed to be the most appropriate considering the duration and nature of this systematic review.
3.5 Data Analysis and Synthesis
Given the likelihood that selected studies would examine the relationship of s100β with clinical measures (e.g. IUGR) of disease severity (e.g. fetal brain damage); we were aware that any data synthesis would most likely be qualitative in nature.
Chapter 4: Results
The electronic searches identified 7,085 articles. After removing duplicates, 5,288 unique articles were screened. The full text of 23 articles was then assessed for eligibility, and of those, 19 articles were excluded (see Appendix 4). Finally, data were extracted from a total of 4 articles (see Table 2).

Contrary to prior expectations, PubMed displayed a larger number of results for the four biomarkers. When two individuals combined and searched the concepts of brain damage and IUGR with each biomarker on PubMed, the results portrayed 954 for s100β, 594 for kynurenine, 281 for carbonic anhydrase and 57 for fetal cells. Yet, when they combined the above concepts with maternal blood, they obtained an increase in results including 959 for S100β, 606 for kynurenine, 291 for carbonic anhydrase, and 484 for fetal cells. Furthermore, when the entire set of biomarkers and concepts were searched together, this conferred a greater result of 25,728. Raw data from test searches on PubMed are recorded in Appendix 3. Upon discussions with a field specialist, the term ‘brain injury’ was replaced by a more appropriate term called ‘Hypoxic ischemic encephalopathy’. On Scopus, when they combined and searched all search terms with an (AND) cord blood and in all fields, it bought narrowed and relevant results (234). Conversely, to be consistent with the other search strategies used from other databases, they used (OR) cord blood which resulted in a larger number of results (3707).
4.1 Study Characteristics
Four studies involving 440 numbers of women were included (see Table 3 for study characteristics). All studies were conducted in hospital departments, two focused on PE and others reported fetal brain damage.



4.2 Study Quality
The mean total score produced by applying the quality questionnaire to each of the included studies was 8 (see Appendix 3 for detailed information). There was no evidence to indicate quality scores for newly published papers were better than those published in the past. All studies were selected and represented cases and controls in a satisfactory manner. Moreover, there was a clear distinction between cases and controls in each study. Furthermore, the data that was acquired was relevant and consistent and were measured through standardized means.



4.3 Study Findings
Most studies were of European descent. Gazzolo (2006) demonstrated a higher maternal S100β concentration in Groups B and C whereas Beharier (2012) found S100β levels within normal ranges prior to and after fetal brain damage. Both studies were conducted at different trimesters but evaluated mothers in similar age groups. Gazzolo (2006) had larger participant groups than Beharier (2012). Gazzolo had a relatively higher number of participants in the experimental groups than the controls. Beharier (2012) did not have a control group. Vettorazzi (2012) and Wikstrom (2012) presented high S100β levels in women with PE. Both studies had similar sample sizes except differing numbers in the experimental and control groups. Wikstrom (2012), had more experimental participants. Wikstrom (2012) was conducted during the first to third trimester while Vettorazzi (2012) was conducted in the third trimester. Beharier (2012) collected maternal blood from the cubital vein where other studies collected it from the peripheral vein.
Chapter 5: Discussion and Analysis
Beharier (2014) demonstrated contrary to what Gazzolo, 2006 found (Beharier 2014). This study presented maternal S100β levels for fetuses with acute brain damage were within normal range (Beharier 2014). These differences were possibly due to methodological variations between the models (Beharier 2014). Whilst Gazzolo, 2006 did not impair the cardiovascular function of the fetus via injection of potassium chloride to impede the heart, Baharier, 2014 did (Beharier 2014). Hence, the transport of S100β from the damaged brain to the placenta may have been blocked, leading to a significant reduction in an S100β ratio from fetal to a maternal compartment of the placenta (Beharier 2014). Furthermore, there are ethical dilemmas raised from Beharier, 2014 as laws of many countries oppose feticide, as a consequence, those countries would not be able to participate in studies as such (Beharier 2014). PE is a medical condition of pregnancy characterized by high maternal blood pressure and protein in the urine (Al-Jameil, Aziz Khan et al. 2014). It often starts after 20 weeks of pregnancy (Al-Jameil, Aziz Khan et al. 2014). Severe PE complications involves red blood cell breakdown, a low blood platelet count, kidney dysfunction, swelling and shortness of breath due to fluid in the lungs, or visual disturbances (Al-Jameil, Aziz Khan et al. 2014). It is associated with varying degrees of damage to the fetus (Mendola, Mumford et al. 2015). The primary impact is under-nutrition due to uteroplacental vascular insufficiency (Mendola, Mumford et al. 2015). Infants born preterm due to PE demonstrate increased risk of long-term health effects including learning disability, cerebral palsy, epilepsy, deafness, and blindness (Cosmi, Fanelli et al. 2011). Wikstrom, 2012 indicated that S100β plasma levels elevate during pregnancy in women with PE and eclampsia (Wikstrom 2012). More significantly, these levels are higher several weeks prior to the onset of clinical symptoms in women developing PE when compared to healthy controls (Wikström 2012). Noteworthy, the actual origin of S100β in women with PE is unknown (Wikström 2012). Nevertheless, PE and eclampsia are associated with blood-brain barrier disruption which makes it possible for high S100β content to pass over to the maternal circulation (Wikström 2012). S100β levels in women with PE is secondary to cerebral vascular damage and thus, reveals the degree of cerebral involvement in the disease (Lehmann, Picas et al. 2017). This was supported by a participant in this study whereby exceedingly high S100β levels were found in them a couple of hours after an eclamptic seizure (Wikstrom 2012). Surprisingly enough, patients with epilepsy do not have increased levels of S100β and hence, the seizure was not responsible for elevated concentrations of S100β, but rather the severe cerebral vascular changes associated with endothelial dysfunction, primarily impacting permeability of the brain blood barrier (Wikström 2012). Furthermore, their study could not eliminate the prospect of S100β in women with PE originating from extra-cerebral resources (Wikström 2012). As we denoted earlier, S100β has a placental origin and therefore the source may have come from the uteroplacental compartment (Wikström 2012). In addition as previously discussed, there is evidence to suggest there is increased S100β in intrauterine growth-restricted fetuses and in pregnancies with chronic fetal hypoxia, there is an increased amount of S100β in amniotic fluid observed (Parker and Cubitt 1999). Nonetheless, none of the infants born in this study’s population had experience of IUGR and thus, this infers that increased S100β in women with PE was not caused by fetal contribution to the maternal circulation (Wikström 2012). For similar reasons as above, Vettorazzi, 2012 also showed that women with severe PE had higher levels of S100β compared to those with mild PE and normotensive pregnant women (Vettorazzi 2012).

CONCLUSION AND RECOMMENDATION
Conclusion
To sum up, the research points at the danger of developing hypoxic-ischemic encephalopathy that consumes millions of lives of the infants. HIE leads to serious complications such as mental retardation, epilepsy as well as cerebral palsy among others. This raised the idea of conducting early diagnosis of brain damage in the fetus, which paves way for precautionary measures that can enhance the cognitive condition of the infants. Biomarkers are thought to be most immediate solution towards rectifying possible chances of brain damage. Based on this, the research aimed at conducting systematic evaluation of different pieces of evidence behind the maternal biomarkers such as kynurenine, carbonic anhydrase and S100β. A significant look at the systematic literature review invested time on the definition of biomarkers, while observing the behavior of the maternal fetal biomarkers. The review also took note of the techniques applied in identifying the biomarkers, which include the metabolomics and proteomics. Metabolomics is realized in the analysis of metabolites while proteomics separates as well as identify proteins. Another area of interest was the causes of the fetal brain damage where the review looked at the intrauterine growth restriction, circulatory centralization, cerebral perfusion and the fetal cardiovascular response. On the other hand, the vast look at maternal biomarkers included a purview of maternal S100β, placental carbonic anhydrase, placental kynurenine and the fetal genes. In realizing the findings that could be connected to the review, methodology is thought to have played a significant role. The search strategy became pertinent as search terms could be selected in relation to biomarkers. The search involved the concepts and categories related to the existing literature. Databases such as CINAHL, PubMed and Embase also played a key role in establishing key findings connected to the essence of biomarkers in saving lives. Study selection and data extraction basically relied on the study design and the study settings, while data analysis and synthesis focused more on the relationship between the clinical measures and S100β. With the research process in place, the European studies established higher maternal S100β concentration across the significant cases. As much as some of the acute damages could feature within the normal range, the scales of damage need attention and intervention at the same time. This is based on the fact that most of the studies could not establish the severity of the condition. In conclusion, there is some evidence to suggest that a high concentration of S100β in the maternal bloodstream can predict fetal brain damage. However, more comprehensive research needs to be done to examine diagnostic potential of maternal S100β as a prospective biomarker.
Recommendations
Dried blood spot (DBS) sampling are conducted in every Australian newborn which is a type of bio-sampling whereby blood samples are blotted and dried on filtered paper. Thus, a retrospective study is more recommendable and need to be completed through dried spot protein quantification using liquid chromatography-mass spectrometry (LC-MS). Researchers have access to clinical data of the mother and foetus of each DBS stand-print. This means that they should do an analysis of results of LC-MS S100β quantification and existing clinical data of the mother and foetus. They could then charter the information together and make effective conclusions concerning the potential of whether maternal S100β could be a biological signature of fetal brain damage, based on the evidence they obtained.
Limitations
One of the major limitations of this systematic review was that there was an insufficient amount of time to evaluate the other maternal biomarkers and hence, researchers were unable to draw meaningful comparisons between them. Therefore, they were not able to comment on which was the best for detection of fetal brain damage.
Future Research
Henceforth, future research should constitute two trials for the determination of whether maternal S100β is an effective biomarker for fetal brain damage. These include a prospective and retrospective study. Since the prevalence of fetal brain damage is above 2 per 1000 live births, a larger cohort of pregnant women needs to be recruited (Odding, Roebroeck et al. 2006). Hence, we propose 100,000 pregnant women be enlisted for this prospective study in order to recruit a sample size of approximately 200 fetuses with brain damage. An appreciably larger participant number would allow for enhanced transparency between results and an effective and thorough evaluation of the research interest.
References
Al-Jameil, N., F. Aziz Khan, M. Fareed Khan and H. Tabassum (2014). "A Brief Overview of Preeclampsia." Journal of Clinical Medicine Research 6(1): 1-7.
Allison, B., K. L. Brain, Y. Niu, A. Kane, E. Herrera, A. Thakor, K. Botting, C. Cross, N. Itani, K. Skeffington, C. Beck and D. Giussani (2016). Fetal in vivo continuous cardiovascular function during chronic hypoxia.
Beharier, O. S., E.Eshcoli, T.Szaingurten-Solodkin, I.Aricha-Tamir, B.Weintraub, A. Y.Sheiner, E.Holcberg, G.Hershkovitz, R. (2014). "Detection of S100B in maternal blood before and after fetal death." Prenat Diagn 34(1): 94-97.
Deeks J, D. J., D'Amico R, Sowden A, Sakarovitch C. (2003). "Evaluating non-randomised intervention studies." Health Technol Assess 7(27).
Garnier, Y., A. Frigiola, G. L. Volti, P. Florio, R. Frulio, R. Berger, S. Alm, M. U. v. Duering, A. B. C. Coumans, F. M. Reis, F. Petraglia, T. H. M. Hasaart, R. Abella, H. Mufeed and D. Gazzolo (2009). "Increased Maternal/Fetal Blood S100B Levels Following Systemic Endotoxin Administration and Periventricular White Matter Injury in Preterm Fetal Sheep." Reproductive Sciences 16(8): 758-766.
Gazzolo, D., E. Marinoni, R. Di Iorio, M. Lituania, M. Marras, M. Bruschettini, P. Bruschettini, R. Frulio, F. Michetti, F. Petraglia and P. Florio (2006). "High Maternal Blood S100B Concentrations in Pregnancies Complicated by Intrauterine Growth Restriction and Intraventricular Hemorrhage." Clinical Chemistry 52(5): 819-826.
Irwin, M. (2014). "A systematic review evaluating non-invasive techniques to diagnose genetic disorders in a human fetus and the ethical implications of their use." Australian Medical Student Journal 1(1).
Kaufmann, P., J. Mühlhauser, C. Crescimanno, M. Castellucci, H. Rajaniemi, S. Parkkila and A. P. Milovanov (1994). "Immunohistochemistry of carbonic anhydrase in human placenta and fetal membranes." Histochemistry 101(2): 91-98.
Lo, Y. M. D., K. C. A. Chan, H. Sun, E. Z. Chen, P. Jiang, F. M. F. Lun, Y. W. Zheng, T. Y. Leung, T. K. Lau, C. R. Cantor and R. W. K. Chiu (2010). "Maternal Plasma DNA Sequencing Reveals the Genome-Wide Genetic and Mutational Profile of the Fetus." Science Translational Medicine 2(61): 61ra91-61ra91.
Marinoni, E. I., R. D.Gazzolo, D.Lucchini, C.Michetti, F.Corvino, V.Cosmi, E. V. (2002). "Ontogenetic localization and distribution of S-100β protein in human placental tissues." Obstetrics and Gynecology 99(6): 1093-1099.
Midgley, A. R., G. D. Niswender and R. W. Rebar (1969). "PRINCIPLES FOR THE ASSESSMENT OF THE RELIABILITY OF RADIOIMMUNOASSAY METHODS (PRECISION, ACCURACY, SENSITIVITY, SPECIFICITY)." Acta Endocrinologica 62(1 Suppl): S163-S184.
Opitz, C. A., U. M. Litzenburger, F. Sahm, M. Ott, I. Tritschler, S. Trump, T. Schumacher, L. Jestaedt, D. Schrenk, M. Weller, M. Jugold, G. J. Guillemin, C. L. Miller, C. Lutz, B. Radlwimmer, I. Lehmann, A. von Deimling, W. Wick and M. Platten (2011). "An endogenous tumour-promoting ligand of the human aryl hydrocarbon receptor." Nature 478(7368): 197-203.
Ridderstråle, Y., E. Persson, V. Dantzer and R. Leiser (1997). "Carbonic anhydrase activity in different placenta types: A comparative study of pig, horse, cow, mink, rat, and human." Microscopy Research and Technique 38(1-2): 115-124.
Spittle, A., J. Orton, P. J. Anderson, R. Boyd and L. W. Doyle (2015). "Early developmental intervention programmes provided post hospital discharge to prevent motor and cognitive impairment in preterm infants." Cochrane Database of Systematic Reviews(11).
Wikström, A. K. E., L.Karlsson, M.Wikström, J.Bergenheim, M.Kerud, H. (2012). "Plasma levels of S100B during pregnancy in women developing pre-eclampsia." Pregnancy Hypertension 2(4): 398-402.



- 24/7 Customer Support
- 100% Customer Satisfaction
- No Privacy Violation
- Quick Services
- Subject Experts