Environmental Decontamination in Healthcare
Introduction
As it is established that organisms are shed from both infectious and colonised patients into the environment (Donskey, 2010), a great emphasis has been given by the Infection Prevention and Control (IPC) team on decontamination of environment and of re-usable equipment to reduce the rate of healthcare associated infections (HCAI). Environmental decontamination has been supported by various studies (Weber et al. 2010; Otter et al. 2011; Rutala and Weber, 2011; Donskey, 2013). The organisation I work for has acknowledged the importance of providing a safe environment for the patient by focusing on the quality of care delivered to them.
The IPC team plays an important role in attaining this goal by performing yearly audits that are established on the recommendations by the Infection Prevention Society (IPS) to assess compliance against key policies to reduce HCAIs. IPS is a robust system that was put in place to ensure the set standards are met while carrying out decontamination of equipment and environment (Health and Social Care Act, 2008). It also ensures that a safe system is in place to protect the patient, staff, and others from the risk of cross infection (Health and Safety at Work etc. Act, 1974). Permanent and contract staff functioning on behalf of the trust in both community and hospital settings are expected to comply with the policy and guidelines to minimise the risk of transmission of infections.
Audit reports illustrated that decontamination of the patient environment and re-usable medical equipment were not performed appropriately due to many decontamination wipes available for use. The choice of three complicated the situation especially for new staff members, doctors, and auxiliary staff. There was also poor ordering of appropriate wipes due to misunderstanding. This was reflected in the audit reports and was assumed as a reason for not meeting the national targets for C. Diff and MRSA blood stream infection. Considering the audit findings, the IPC team looked for different ways of resolving the issue. The innovative plan that was established aimed to reduce the number of wipes that would improve the quality, productivity, and economic growth (Department of Health, 2011).
It would also reinforce the responsibility of the Trust to improve the quality of care provided to the society and to reduce the risk of HCAIs which will, consequently, reduce the associated costs (Health and Social Care Act 2008; NICE, 2011; Care Quality Commission (CQC), 2017). The new and innovative ways to tackle the situation encouraged the Infection Prevention and Control Nurse (IPCN) to think critically (Tidd and Bessant, 2014). As an IPCN, I looked particularly at some of the levers that we could use. The uncomplicated model of innovation process (Figure 1) enabled for consideration of the decontamination wipes which are used in the neighbouring health care facilities. Accordingly, The Director of Infection Prevention and Control (DIPC) commissioned a cross-over trial of 2 different types of wipes. A pilot project was developed that could be done at pace with the plan to make it as a roll out project if successful. The project plan (Part A) I developed exhibited the overall aim and the scope of the project. It demonstrated the ability to choose appropriate decontamination wipes by downsizing the number of available wipes through carrying out a comparison study on the benefits and detriments. By the end of the pilot project, the plan was to implement the roll out process of new decontamination wipes. This essay will go through the reflections on the knowledge and skills that I have learned while developing a business case and the process through which the project progressed. The emerging themes that I encountered during the process were leadership, stakeholder analysis, communication, and importance of collaborating and networking with other teams. Continue your journey with our comprehensive guide to Developing Subject Knowledge.


Emerging themes
Leadership:
Accepting this role was both exciting and challenging for me. The successful practice of innovation demanded interaction and integration at the individual and collective levels of management (Tidd and Bessant, 2014). I was a little bit stressed and anxious when I realised that most of the individuals who were part of the core team were seniors in the organisation. I realised that it is important to make sure that the level of stress that I undergo throughout this project had to be controlled as it might affect the performance. While I had some element of stress, being a novice, the support from my lead nurse was very reassuring and motivating. She advised me to use my ability to speak in front of a group, be poised and innovative and to be self-confident (Bass, 2008; Dunphy et al. 2009; Day, et al. 2011; Yulk, 2013).

I took the opportunity to use my knowledge on emotional intelligence to self-assess myself and make some necessary changes in my behavioural pattern so that I can work beyond my area of expertise to become an Advanced Practitioner (National Health Service, Scotland, 2018). Making decisions and disseminating them was another important aspect during the life cycle of the project (Yulk, 2006). This involved reviewing circumstances; selecting new stakeholders into the core team, choosing different strategies; allocating resources and responsibilities to different people; and organising. Keeping the stakeholders in the loop while analysing situations or changing strategies helped to deal with difficult situations easily.. Meetings were organised as teams and as individuals to analyse the individual output and progress. This helped to inspect the circumstances and apply appropriate leadership styles to handle them (Muller and Turner, 2010). I looked into team participation which was visible while I used Tannenbaum and Schmidt model, 1958 (figure 3) to make decisions. There were instances where I had to take decisions and announce it to the team (Roe, 2017). Yammarino’s (1993) view on this was to be charismatic as well as to understand the followers’ needs and situations and approach it in a different style if necessary. However, in certain cases, the leader has to work by thinking beyond the emotional connection to the followers mixed with collective dedication to a noble cause (Diaz-Senz, 2011). This helped my thought process in analysing decisions.
Continue your journey with our comprehensive guide to Environmental Awareness and Teamwork among Children.

Using different leadership styles, I was able to demonstrate team participation in decision making. The use of transactional style and participative style demonstrated different effects at different circumstances. This paved a way to build interpersonal relationships and to maintain the group’s focus in attaining the goal. It helped to communicate well with the team, provide instructions, delegate duties, and co-ordinate them (James, 2011). As a result, the staff actively participated in this project as the benefits of transitioning to new decontamination wipes were precisely understood and instructions on how to perform the task were provided in advance. This project helped me to understand that the relation between the leader and the followers becomes fruitful only if both sides are understood, influenced and appreciated (Kouzes and Posner, 2011; Day and Antonakis 2012).
Communication
Interaction between stakeholders is vital for the success of the project (Stirman et al. 2012; Butt et al. 2016). Communication plays a vital element in conveying the mission and vision, reinforcing values, following up, discussing, and offering training. Watson (2014) believes that poor communication skill does not go along with innovative and creative decision-making. Communicating the attainable vision in a creative way by the end of this project went beyond emails and team meetings. The IPC team volunteered to meet the staffs who work at the pilot wards, to communicate the vision, and to educate and support them. Thus, I was able to make stakeholders participate well in the project (Gill, 2011). Advance practice professionals are expected to work as a team and to delegate duties appropriately (Department of Health, 2010 a). With many options available such as organising catch-up meetings, one to one meetings, providing training and support for staff created great opportunities to build my communication skill beyond simply growing my contact list. It also made me reflect on the leadership quality that I possess and my level of communication. I have used these opportunities to develop my skills as a leader and speak with confidence. Being confident assisted me in disseminating information, voice concerns, and to uphold integrity at high level (Schwartz et al. 2011). Communicating at the right time is also vital for the success of implementation of any project (Gluyas, 2015; Vermeir et al. 2015). If communication does not occur at the right time, it can lead to crisis and makes it necessary to put in extra effort to sustain a project (Taran, 2011). This happened in my project when there was an unexpected shortage of wipes in one of the departments due to ineffective communication between the staff and the Ward Manager to make an order for the extra supply that they needed for the weekend. Moreover, the road block due to heavy snow made it impossible to bring a new stock. I observed that engaging different players and aligning them with the core vision is always difficult. I made a solitary decision to advise the staff to use the previous set of trial wipes to cover the period. Upon reflection, it was reckoned that poor communication could have led to untoward circumstances. As there was a break in the trial period, I felt that the time of this set of testing must be extended.
Take a deeper dive into Equality Diversity and Inclusion in Healthcare and Workplace Settings with our additional resources.
Collaborating and networking
A manager’s role is considered to be a complex one and a few characteristics are expected from you when you are holding that position (Hales, 2001). Part of the role which I had to work on was collaborating and networking with other members. As a novice, I felt initiating networks to be daunting. Even though I was not new to the profession and I had a well-established career, developing and nurturing my network beyond a few immediate contacts seemed to be intimidating at the beginning. As the project took its shape, I realized that it is not a low-return investment of my limited time. Martin et al. (2010) suggests that managers can interact with the team members either formally or informally. I preferred informal relations with team members as that was the culture of the organization. I also felt that this would allow them to approach me whenever they wanted to without hesitation (Mueller, 2015). As different stakeholders possess different experience, personality and individual ability (Mosadeghrad, 2012), it was necessary to be mindful of how I maintained relations with the focus group and with others (Mosadeghrad, 2014). I was under the impression that individuals would own up responsibilities related to their job profile. This belief put me into a situation where the deadlines were not met by one of the stakeholders. The decision to commence the trial on 2nd of February had to be postponed by another week due to issues related to delivery of chosen products to 3 different sites at the same time. I felt the need to be more mature, observant, and to manage the situation without compromising my professional integrity or quality of work. At this point, I made an effort to see what worked for others and how to shape my own leadership style and management over time. I reminded the soft facilities management (fm) representative about the date we had chosen to start the trial and requested to make arrangements to deliver the products at the earliest time possible. Working collaboratively with stakeholders, delegating tasks, and using my networking skills assisted me to work towards achieving the title of advance practice. (Department of Health, 2010a; Nursing and Midwifery Council, 2015). I was conscious that my performance as a project manager will be evaluated based on the outcome of this project. This awareness motivated me to closely monitor and track the progress of the project (Turner, 2014). I made sure that the project adhered to the high ethical standards of my profession. I recognized that throughout the project cycle, different measure will be undertaken to sustain the project and the characteristics of remaining ethical is vital (Muller et al. 2013; Eskerod et al. 2015). This project can be considered to be a clinical trial because it involved trying to determine the appropriate wipes for the decontamination process (Turner, 2014). One way of evaluating how effective a certain set of wipes is in decontaminating the equipment and environment is to assess the rate of infection among patients when the wipes are used.
Take a deeper dive into Ethical Standards and Legislative Compliance in Quality Control Management with our additional resources.
Since the project involved patients, there were a number of ethical issues that emerged. One of the ethical issues that emerged in the project was the safety of patients during trials (Ulrich et al., 2010). The trials were aimed to determine which wipers were best suited for the decontamination process. However, the trials jeopardized the safety of patients since it put them at a risk of increased infection as a result of failure of a certain set of wipes to decontaminate the equipment or the environment (Fouka and Mantzorou, 2011). Another ethical issue that emerged during the project was the involvement of patients in the trials without their consent. It was realized during the project in trying to determine which wipes are appropriate for the decontamination process patients were inadvertently involved in the trials (Huston, 2013). This is because the decontamination process was aimed to make equipment and the environment safer for patients and, as indicated before, one way of evaluating the level of safety of equipment and the environment is to assess the level of inflections among patients (Burkhardt and Nathaniel, 2013). However, while patients were indirectly involved, they were not informed nor were their consent sought. After analysing the ethical implications of the project, I realized that the project had the potential of violating various ethical principles. There are seven main ethical principles. These are truthfulness, confidentiality, autonomy, informed consent, beneficence, nonmaleficence, and justice (Judkins-Cohn et al., 2014). Truthfulness involves telling a patient the truth about their condition or informing participants in a clinical trial what exactly the trial is about. This allows them to make an informed decision. Confidentiality is an ethical principle which requires practitioners to keep information about patients secret (Avery, 2013). In a clinical trial, it involves researchers avoiding divulging personal information of participants in the study. Autonomy, on its part, is an ethical principle which requires patients or participants in a clinical trial to be provided with the right and freedom of self-determination (Ulrich et al., 2010). It means that healthcare practitioners or researchers are not supposed to influence decision making among patients or participants. Informed consent is an ethical principle which requires practitioners to provide patients with accurate information so that the patients can provide an informed approval on the kind of treatment or procedure that needs to be carried out on them (Burkhardt and Nathaniel, 2013). Consent provided by patients should thereby be based on accurate information.
Beneficence is an ethical principle which requires practitioners to act in a way that would benefit patients. Nonmaleficence, on the other hand, is an ethical principle which requires practitioners to act in a way that does not result in harm to patients (Huston, 2013). Lastly, justice is an ethical principle which indicates that practitioners should act in a way that promotes fairness for all patients. In this project, the principles which were violated or were at a risk of being violated, albeit inadvertently, are beneficence, autonomy, and nonmaleficence (Judkins-Cohn et al., 2014). The patients were not informed of the trial and how it would affect them. In this case, they were not provided with an opportunity to make an autonomous decision concerning the trial (Avery, 2013). With respect to beneficence and nonmaleficence, the project was aimed to benefit patients in the long term. However, in the short, it was likely to cause harm as a result of infections due to failure of wipers to decontaminate equipment or the environment. To deal with the ethical issues that emerged, I discussed with the team involved on the best way to approach. We agreed that the trial had to be carried in a way that had limited effect of patients (Huston, 2013). For example, we resolved that using infections among patients as a way of evaluating the effectiveness of wipes was not appropriate since it put patients at a risk. To evaluate the effectiveness of a certain type of wipes, I instructed for used equipment to be tested in the laboratory after being cleaned by a certain type of wipes to determine whether they were still contaminated (Ulrich et al., 2010). I also decided to designate a study area that would help evaluate the effectiveness each type of wipes. By ensuring that patients were involved in a very limited proportion, I was able to resolve most of the ethical issues that the project faced. I also discussed and secured an agreement from the lead nurse that if I encountered any ethical issues that I could not deal by myself, I would seek her assistance to provide an appropriate response (Jonasson and Ingason, 2013). Therefore, she was always updated about the progress of project cycle.
Stakeholder analysis
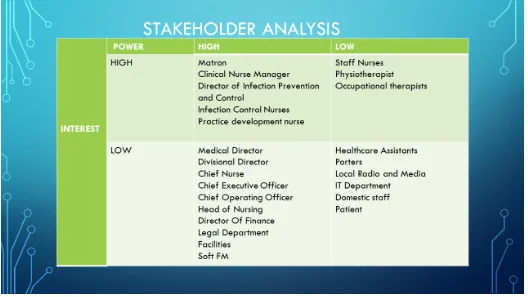
As part of trialling new decontamination wipes in pilot wards, stakeholder analysis was performed to achieve maximum engagement by the stakeholders within the set period of time. This helped me to identify the people who will be participating and supporting the project, build relationships between different stakeholders, mitigate risks, and attain stakeholder engagement (Littau et al. 2010). As stakeholder analysis is a very crucial element, it was performed at the earliest stage of project cycle with great importance given to the selection of members (Niemeijer et al. 2013). To identify the stakeholders, I started by brainstorming and making a list of people and groups that would be affected by the outcome of the project (Beringer et al. 2013). I arranged a meeting to meet the stakeholders and agreed with them that there will be subgroups in the team that will step in as their phase comes and provide assistance. A list of stakeholders was then made and analysed in terms of power, influence and extent to which they will be affected by the project (Figure: 4). An agreement was made to keep the rest of the subgroups informed of the progress. I then focused on making a well-calculated plan as well as use effective leadership skills (Hodin, 2013) to get them to participate.
Since change is hard (Allock et al. 2015), it is necessary to motivate stakeholder engagement with a clear vision of change. Being committed and being a respectable leader enabled me to achieve this (Dixon-Woods et al. 2012; West et al. 2014; Kaplan et al. 2014; Dixon-Woods et al. 2014) by keeping stakeholders informed of the decisions made (Muller and Turner, 2010). The project process was communicated to members on a weekly basis. Even though the IT department belonged to the low power-low interest group, they were contacted at the beginning since linking the project to information systems was found to be very dynamic. The use of informatics is useful in today’s technological healthcare environment. Linking IT professionals was pivotal to the project’s success as it helped me to learn more than the basic skill that I possessed (Kelly, 2012). Nevertheless, at this point of the project, their involvement was minimal as their service was more in the second part of the project. Nonetheless, their support to create a generic email id for the project team, data base storage, and creating flyers was requested. It was decided in the meeting that the National Health Service (NHS) systematic six-stage service improvement methodology (NHS Institute for Innovation and Improvement, 2011) (Appendix: 1) will be used as the framework to develop the plan. The decision to use the six-stage service improvement methodology was informed by how elaborate the methodology is dealing with each aspect of service improvement. The contribution by each stakeholder was appreciated in each phase of the project (The NHS Institute for Innovation and Improvement, 2011).
Conclusion
Department of health (2010) suggests that there is need to develop a safe system of work to prevent transmission of infections by contact with contaminated equipment and/or the environment. While project management was entirely new to me, my role as an IPC nurse in the organisation meant that I could influence and educate staff to work towards achieving this goal. This title also helped me to understand the influence of contextual factors on leadership and how it affects each stage of the project. As a leader, I was mindful of the environmental context in which tasks were taking place. Stakeholder analysis helped me to get commissioners, managers of different departments, matrons, healthcare workers, allied workers, multi-disciplinary team (MDT) engaged in this project. Their ability to add input and to think and take action for the attainment of the common goal (Elton, 2015) was the main ingredient towards the success of the trial. Throughout the process, I was highly engaged as the responsibility of planning, running, revisiting, arranging meetings, and collecting feedbacks fell on me. Dealing with untoward circumstances was new to me. However, I learned to rely on others to help me deal with such circumstances. All the same, the awareness of being accountable for the outcome of the project made it exciting. Apart from the inevitability of dealing with conflicts and confusions, this project helped me to realise that my reaction to such situations is very crucial and that I should not deal with it in anger or in a harsh manner. The ability to delegate duties to the senior members in the organisation was a challenge. As such, I must continue to build on it while handling future projects.
Outcomes
Introduction
Being a nurse by profession and holding the project manager title made me step into the unknown world of project management. Project management is about planning, organising, and controlling people, money, and resources (Lock, 2013) till the end of the assignment. Participating in this project enabled me to understand that I should be competent and use all my skills and talents in leading a group of people and maintaining relations (Nursing and Midwifery Council (NMC), 2015). Considering this as an opportunity to progress myself as an Advanced Practitioner, I had to look for ways of developing the skills that were important in leading and influencing others to generate change in the organisation. The NHS Leadership Quality Framework, (Department of Health, 2014) affirms that leaders must possess the ability to lead and inspire others by evaluating information and connecting the need to change with the vision of the organisation. In addition to this, the challenges of assessing risks at each phase of the project cycle and resolve issues were inevitable. The cross over trial of the new decontamination wipes were welcome by the HCWs due to the benefits it brought along with it. The part of selecting the most user-friendly wipes depended on the information the evaluation sheets which were filled in by the HCWs and which provided a comparison of different types of wipes. In this part of the essay, I will be concentrating on the outcomes of the project and the emerging themes that played a significant role in influencing its success. The role of emotional intelligence, managing risks, and engaging stakeholders using leadership skills and sustaining the change were the key items that I used to develop my role as an Advanced Practitioner (West, 2012). This section will also address the reasons for the likelihood of abandoning the project even after the successful completion of cross-over trial.
Emerging themes:
Emotional intelligence (EI)
As the project manager’s role has changed significantly over the past decade and changes are occurring at a faster pace, it is necessary to win the hearts and minds of the workforce rather than just commanding them. To succeed in such a situation, the project manager must possess both technical skills and the ability to make good relations with the followers (Joseph et al. 2014). Building interpersonal relationships, collaborating and networking, and developing good leadership skills helped me to do my best in this profession. Goleman’s (1996) proposed that relationship management along with technical skills is essential for successful project planning and implementation. I learned that EI was essential in helping to monitor the pulse of the project management profession, and gain insight into what organizations want in their leaders and managers. As a leader, I had to be very empathetic in nature, listen to the concerns of the team members as well as the stakeholders. I had to understand other people’s perspective to manage conflict constructively. I also learned that to get more staff engagement, the benefits in participating in the project have to be explained well ahead of the process. HCWs were assured that upon successful completion of the roll over process, they would benefit by improving their efficiency level with less confusion on which wipes to be used and also it will make their job easy. This did not only support the project in a positive manner, it also provided motivation for the staff to provide their sincere comments in the evaluation sheets. Association between collaborative behaviour and transformational leadership became evident while I developed my skills in providing support to individual followers, communicating the vision, and transforming as a charismatic person (Schlaerth et al. 2013, Harms and Crede, 2010). While Walter et al. (2011) and Cote et al. (2010) suggest that EI has the potential of helping one to understand characteristics of leadership, Weinberger (2009) declines the fact that EI and task efficacy have any relation. I personally agree that being mindful and recognising emotions and controlling it will help to lead others (Gilbert-Smith, 2003, Chapman-Clarke 2016).
Risk Management:
This part of the essay will deal with the processes and activities that have allowed the project to attain its objective with very low level of threats. Burke (2013) recommends that risks must be managed by classifying, measuring, reacting, and controlling it at the early phase of project management itself, and also to perform this as an ongoing process throughout the project cycle. With the use of PESTLE analysis, the potential problems that can be encountered while upgrading the existing system of decontamination were discussed in the meeting and listed down in the project charter (Appendix 2) with the aim to avoid these risks completely. Plans were then made to mitigate them and communicate among core team members (Wysocki, 2014). While risk analysis was performed, the likelihood of an environmental hazard was not considered and compared to the data from previous projects which were carried out in the organisation. Unexpected heavy snow put the delivery of wipes on hold and because of poor communication there was an instance where the pilot ward suffered from shortage of trial wipes. Upon reflection, it was reckoned that natural hazards are part of life and measures should have been adopted to mitigate the impact of disaster. The failure in delivering materials could be considered as a failure at the procurement side which was an avoidable one. Communication failure led to misjudged supplies, uncertain aims, and unsuccessful planning. As a developing Advanced Practitioner, I managed to solve this problem by considering this as a challenge. The ability to think creatively and innovatively, assign tasks, and the ability to lead the team in such a difficult situation provided me the strength to be imperative (Iglehart, 2013). Even though I was an inexperienced project manager, I had to try and influence and persuade stakeholders to sustain the pilot study. Reflecting back, I understand that if I undertake a project in future, the first thing that would come into my mind on risk management will be considering weather conditions. It must be mentioned that the impact of this event was high as the patients were put under the potential risk of transmitting infections. However, it was also noted the incidence of road block due to snow was very minimal as it does not occur on a daily basis Therefore this has been classified and documented as a high impact low frequency risk. (Kerzner, 2017). In the following meeting, this incident was mentioned and brought up for discussion which allowed me to determine each member’s feeling on it. Furthermore, plans were formulated to avoid such instances. The use of the live Gantt chart enabled to keep the plan clear and simple for other members to follow. The staff members in the respective wards were then made aware of the importance of performing the study and how they should foresee any shortage in future and respond to it.
Stakeholder Engagement
Once stakeholders have been acknowledged, the means of collaboration and dealing with them have to be considered. Both strategic and operational level support is vital to improve quality and sustain the change in an organisation (The Health Foundation, 2010). The project manager has to remain proactive and put effort to manage and maximize stakeholder involvement (Heagney, 2016). Interacting with different stakeholders and speaking to them at their level of understanding (Heagney, 2012) felt like a tiresome job at the initial phase. However, I came to appreciate the importance of interacting with them since it provided an opportunity to exchange ideas and get their views about the project. The project plan was discussed at their comfort zone and an execution plan was made during the meeting. A common decision was taken to create a share drive with the help of IT department that could be accessed by the core team members. Communication plans were then designed to keep the rest of the stakeholders informed and involved in the project. A Gantt chart was then set up to document the progress of each stakeholder. This chart and the minutes of the meeting were then saved into a common share drive which could be accessed by the core team members. This meeting personally helped me to build relationships and share values with the group to perform tasks competently. Thereafter, a meeting was arranged to meet with all the stakeholders to understand how they feel about the project (Larson and Gray, 2014). This allowed me to find out how they would like to communicate information. This also helped me to identify at what stage each stakeholder will be involved in the project, for how long, and how they would contribute to the success. In this project, the stakeholder group involved Chief Executive Officer, DIPC, soft facilities management representatives, infection control team, chief nurse, ward managers and matron of pilot wards, staff nurse, doctors, allied health care professionals, health care assistants, and administrative staff members. Kurt Lewin’s theory indicates that involving staff members, doctors, and auxiliary staffs are crucial to the success of the project. This helped to reduce worker’s resistance (Dawson and Andriopoulos, 2014). As the success merely depended on how well the MDT members committed themselves in performing the trial, I ensured that the authorities with higher responsibility were involved wherever possible to influence and motivate others. The ward managers were persuaded to influence the MDTs and also to work on their attitudes and actions (Boddy, 2002). Evaluation was performed to analyse the impact of the project-based change upon completion of first phase. This was to ensure that stake holder needs are met (Harris et al. 2016). As different stake holders have different interest in profit, the initial measurement was performed at the stakeholder level. The questions on the evaluation sheets were compared with each other and data stored in the dash board. Analysing the data was very difficult both conceptually and practically as the staff had to be constantly reminded of filling in the evaluation sheets at the expected period of time. Great attention was given on how and where this information was stored and maintained. Data collected was based on the opinion of core team members and was collected in a uniform manner. It was stored in a dashboard which was easily accessible by them and was cost- effective (Hall and Rousell, 2014). This also helped with reviewing and measuring the impact throughout the duration of the project. Graphic presentation of the data in a dashboard was found useful in comparing and contrasting the evaluation questions. This decision-science tool will help with the pending decision making process and evaluation process. (Carroll et al. 2013)
Comparison of the outcomes was valued by checking if stakeholder’s needs were met. It involved looking into few aspects like how much time the staff members saved while performing the job, did it simplify their job, did it improve efficiency and compliance, and did it help to improve job outcomes by avoiding confusion. During the second stage of the project, comparison of the cost of all categories of wipes will be made in relation to the current wipes which are in use in the rest of the wards to ensure cost effectiveness.

Sustaining project:
It is a pre-requisite for an advanced nurse practitioner to identify the needs to develop or improve service in an organisation (National Health Service, Scotland, 2018). The NHS institute for Innovation and Improvement model (NHS Improving Quality, 2014) was used to determine the key positive and negative aspects of the implementation plan and to predict the likelihood of sustainability of the project (Doyle et al. 2013) (Appendix 3). This showed a success rate of 85.4%. As I was working towards advanced practitioner role, I had to put in several steps to support the project by focusing on the weaknesses. To sustain it, it was vital to have good leadership skills that encourage stakeholder engagement, appropriate communication, and build trust from others. Discussion was arranged on the lessons learned and the mistakes made. It was agreed that communication among the key stakeholders went well without much misunderstanding and they engaged well to attain the goal. The key element that I learned was to look into risk management in a much wider perspective in order to avoid repeating it in future. Edkins et al. (2013) indicate that the success of a project is dependent on the social and political influence as well as on the organisation’s goals. During the trial process, MDT engagement was the supreme priority since it was vital in sustaining the service (Kings fund, 2012). I had to be ethical when there was a glitch in attaining HCW’s participation in the initial stage due to the negative opinions spread by some of HCWs. I had to arrange a meeting and explain to them how important they were in the project and how the project was dependent on them (Stevens and Buechler, 2013). To support them, soft facilities management representative provided them with the required training as the new wipes were introduced. The benefit of using those wipes and how it outweighed the previous ones was explained in detail. The method of decontamination was explained and supported with the use of audio-visual slides. Staffs were provided with the opportunity to raise their concerns and queries. It was projected to them that the final outcome totally depended on the evaluation sheets that they would be filling in. It was interesting to note how well the new wipes were welcome by the HCWs. As cost implications are being considered and compared, the chances of abandoning the project at the roll out stage seemed high.
Conclusion
Reflecting back on the project that I was involved in there was a lot of learning happening at each stage of the process. I found myself looking deep into the infection control aspect more as an Advanced Practitioner rather than as a Project Manager. I had to remind myself to refrain from that. There were times where the project had its challenges. Even though plans were made to commence the project by February 2nd it had to be delayed as the stocks did not arrive at the same time in all the 3 sites. On the other instance due to communication breakdown between the manager and the staff and due to natural hazards, the stock was not ordered and brought in on time. This put patients at risk of developing infections. What I learned from this opportunity is that great importance must be given to natural hazards while performing risk assessment. This learning will help me to contribute to success in any future projects I take up.
References:
Allock, C., Dormon, F., Taunt, R. and Dixon, J. (2015) Constructive comfort: accelerating change in the NHS. Policy Analysis. London: The Health Foundation.
Bau, M.S., Brandao, M., Lakshmi, A. and Yale, L. (2008). ‘Mitigating natural hazards through project management’, PMI Global Congress 2008- EMEA. St. Julian’s, Malta. 19 May. Newtown Square, PA: Project Management Institute.
Beringer, C., Jonas, D. and Kock, A. (2013) ‘Behavior of internal stakeholders in project portfolio management and its impact on success’, International Journal of Project Management, 31(6), pp. 830-846.
Butt, A., Naaranoja, M. and Savolainen, J (2016) ‘Project change stakeholder communication’, International Journal of Project Management, 34(8), pp. 1579-1595.
Chapman-Clarke, M. (2016) Mindfulness in the workplace. An evidence-based approach to improving wellbeing and maximizing performance. London, United Kingdom: Kogan Page limited.
Cote, S., Lopez, P, N., Salovey, P. and Miners, C. T. H. (2010) ‘Emotional intelligence and leadership emergence in small groups’, The Leadership Quarterly, 21(3), pp. 469-508.
Dawson, P. and Andriopoulos, C. (2014) Managing Change, Creativity, and Innovation. 2nd ed. London: CPI group Ltd.
Day, C., Sammons, P., Leithwood, K., Hopkins, D., Gu, Q. and Brown, E. (2011) Successful School Leadership: Linking with Learning and Achievement. Maidenhead: McGraw Hill Open University Press.
Diaz-Senz, H. R. (2011) ‘Transformational Leadership’, in Bryman, A., Collinson, D., Grint, K., Jackson, B. and Uhl-Bien, M. (ed.) The Sage Handbook of Leadership. London: SAGE Publications, pp. 299-311.
Dixon-Woods, M., Baker, R., Charles, K., Dawson, J., Jerzembek, G. and Martin, G. (2014) ‘Culture and behavior in the English National Health Service: Overview of lessons from a large multi-method study’, BMJ Quality and Safety, 23(2), pp. 106-115.
Eskerod, P., Huemann, M. and Savage, G. (2015) ‘Project Stakeholder Management-Past and Present’, Project Management Journal, 46 (6), pp. 6-14.
Garcia-Morales. J. V, Jimenez-Barrionuevo, M . M . and Guttierrez -Guttierrez. L. (2012) ‘Transformational leadership influence on organizational performance through organizational learning and innovation’, Journal of Business Research, 65 (7), pp. 1040-1050.
Goleman, D. (1996) Emotional Intelligence: Why It Can Matter More Than IQ. London: Bloomsbury Publishing Limited.
Hamstra, M. R. W., Van Yperen, N. W., Wisse, B. and Sassenberg, K. (2011) ‘Transformational-transactional leadership styles and followers’ regulatory focus: Fit reduces followers’ turnover intentions’, Journal of Personnel Psychology, 10(4), pp.182-186.
Harms, P. D and Crede, M. (2010) ‘Emotional Intelligence and transformational and transactional leadership: Meta-analysis’, Journal of Leadership and Organisational Studies, 17 (1), pp. 5-17.
Institute of Medicine (US) Committee on the Robert Wood Johnson Foundation Initiative on the Future of Nursing, at the Institute of Medicine (2011). The Future of Nursing: Leading Change, Advancing Health. Washington (DC): National Academies Press.
Jordan, P. J., Ashkanasy, N. M. and Daus, C. S. (2008) ‘Emotional intelligence: Rhetoric or reality?’, In Cartright, S. and Cooper, C. L. (ed.) The Oxford handbook of personal psychology. New York: Oxford University Press, pp. 37-58.
Kaplan, G., Patterson, S. H., Ching, J. M. and Blackmore, C. C. (2014) ‘Why lean doesn’t work for everyone’, BMJ Quality and Safety, 23(12), pp. 970-973.
Littau, P., Jujagiri, N.J. and Adlbrecht, G. (2010) ‘25 years of stakeholder theory in project management literature’, Project Management Journal, 41(4), 17–29.
Lopes, P., Grewal, D., Kdais, J., Gall, M. and Salovey, P. (2006) ‘Evidence that emotional intelligence is related to job performance and affect and attitudes at work’, Psicotherma, 18(1), pp. 132-138.
Mellifont, D., Smith-Merry, J and Scanlan, N. J. (2016) ‘Pitching a Yerkes-Dodson curve ball?: A study exploring enhanced workplace performance for individuals with anxiety disorders’, Journal of workplace Behavioural Health, 31(2), pp. 71-86.
Mok, Y. K., Shen, Q. G. and Yang, J. (2015) ‘Stakeholder management studies in mega construction projects. A review and future directions’, International Journal of Project Management, .33(2), pp. 446-457
Muller, R., Andersen, E. S., Kvalnes, O., Shao, J., Sankaran, S., Turner, J. R. and Biesenthal, C. (2013) ‘The Interrelationship of Governance, Trust and Ethics in Temporary Organisation’, Project Management Journal, 44(4), pp. 26-44.
Niemeijer, G.C., Flikweert, E.R., Trip, A., Does, R. J. M. M., Ahaus, K. T. B., Boot, A.F. and Wendt, K.W. ( 2013 ) ‘The usefulness of lean six sigma to the development of a clinical pathway for hip fractures ‘, Journal of Evaluation in Clinical Practice, 19(5), pp. 904 – 914.
Otter, J.A., Yezli, S. and French, G. L. (2011) ‘The role played by contaminated surfaces in the transmission of nosocomial pathogens’, Infection Control and Hospital Epidemiology, 32 (7), pp. 687–699.
Rutala, W. A. and Weber, D.J. (2011) ‘The role of the environment in transmission of Clostridium difficile infection in health care facilities’, Infection Control Hospital Epidemiology, 32 (3), pp. 207–209.
Schlaerth, A., Ensari, N. and Christian, J. (2013) ‘A meta-analytical review of the relationship between emotional intelligence and leaders’ constructive conflict management’, SAGE Journals, 16(1), pp.126-136.
Shapiro, L. S., Wang, M. C. and Peltason, E. H. (2015) ‘What is mindfulness and why should organizations care about it?’, in Reb, J. and Atkins, P. W. B. (ed.) Mindfulness in Organisations: Foundations, research, and applications. Cambridge: Cambridge University Press, pp. 17-42.
The Health Foundation (2010) Quality improvement made simple: what every board should know about health care quality improvement. London, The Health Foundation.
Vermeir, P., Vandijck, D., Degroote, S., Peleman, R., Verhaeghe, R., Mortier, E., Hallaert, G., Van Daele, S., Buylaert, W. and Vogelaers, D. (2015) ‘Communication in healthcare: A narrative review of the literature and practical recommendations’, International Journal of Clinical Practice, 69 (11), pp. 1257-1267.
Watson, G. (2014) ‘Effective decision making and problem solving’, in Watson, G and Reissner, S. C. (ed.) Developing skills for business leadership. London: Chartered Institute of Personnel and Development, pp. 427-457.
Weber. D. J., Rutala, W. A., Miller, M. B., Huslage, K. and Sickbert-Bennett, E. (2010) ‘Role of hospital surfaces in the transmission of emerging health care-associated pathogens: norovirus, Clostridium difficile, and Acinetobacter species’, American Journal of Infection Control, 38 (5), pp. 25–33.
West, M.A. (2012) Effective teamwork: Practical lessons from organizational research. 3rd ed. Malden, MA: Wiley-Blackwell (an imprint of John Wiley & Sons Ltd).
Yammarino, F. J. (1993) ‘Transforming Leadership Studies: Bernard Bass’ Leadership and Performance Beyond Expectations’, Leadership Quaterly, 4 (3), pp. 379-382.
Ybarra, O., Rees, L., Kross, E. and Sanches-Burks, J. (2012) ‘Social context’, In Cameron, K. S. and Spreitzer, G. M. (ed.) The Oxford handbook of positive organisational scholarship. New York: Oxford University Press, Inc, pp. 201-214.
Ulrich, C. M., Taylor, C., Soeken, K., O’Donnell, P., Farrar, A., Danis, M., & Grady, C. (2010). Everyday ethics: ethical issues and stress in nursing practice. Journal of advanced nursing, 66(11), 2510-2519.
Judkins-Cohn, T. M., Kielwasser-Withrow, K., Owen, M., and Ward, J. (2014). Ethical principles of informed consent: Exploring nurses’ dual role of care provider and researcher. The Journal of Continuing Education in Nursing.



- 24/7 Customer Support
- 100% Customer Satisfaction
- No Privacy Violation
- Quick Services
- Subject Experts