Interagency Support for Frail Elderly
Introduction
The Interagency working is referred to the care system in which different agencies and families of the patients are combined together for creating an interdependent problem-solving approach which focuses to enhance the health and care of the patient (Pugh, 2017). The interagency working is essential because it lowers duplication of services and provides greater efficiency in use of public resources to promote the health of patients, including healthcare dissertation help. It also benefits to create data system which helps to track and monitor the process of the health of the patients across agencies and provides for creating a unified voice to legislate on the unmet requirements of the patients (Gustafson et al., 2016). Thus, effective interagency working leads to create permitting circumstances where better management and functioning of care by the front-line staff occurs for the patients. However, the challenges related to interagency working includes facing obstacles with commitment from interagency individuals which creates barriers in delivering effective care. This is because while of the agency professionals executes hindered care delivery it leads to deteriorate the health condition of the patient and they show lack of effective response to other care or intervention provided at the time by other agencies (Clouston et al., 2018). The present movement in the health and social integration in Scotland is ensuring effective anticipation, prevention and self-management of diseases or illness so that overall quality of health and living is improved among the individuals. The driver towards this present move in health and social care integration in Scotland is due to various factors such as demographic changes in population, higher inequalities in health, changing patterns of health and illness, need of skilled professionals and others (gov.scot, 2019). In Scotland, the Community Care and Health (Scotland) Act 2002 is amended in 2018 which led to the move of extending free personal care to adults who are under 65 years of age along with the previous action of providing free care to the elderly irrespective of the income of the individuals (careinfoscotland.scot, 2019). The move was made under the context that in Scotland, the UK, 560,000 of the population of 65 years and over is frail due to which they have restricted mobility and require assistance for everyday work. The frailty is able to be controlled from progression if effective care from early stage is provided (ihub.scot, 2019). Thus, the amended move was made so that the elderly before entering the age of 65 years can be provided adequate care support to lower their chances of developing frailty in the older age. In this study, the key aim is to explain the way improved interagency working enhances person-centred care for the frail elderly group who have vulnerable health condition leading them to require everyday care assistance.

Inter-agency support for Frail elderly
The frail elderly people are referred to individuals who are over 65 years of age and have become dependent on others for their everyday living and often require institutional care (ihub.scot, 2019). One of the key causes of frailty among elderly is the loss of muscle mass due to ageing which leads them to face hindrance and strength in making string moves such as walking, running and others (Tanaka et al., 2018). The symptoms of frailty include unintentional weight loss, weakness, unexplained exhaustion, lower physical activity and slow walking speed (Soysal et al., 2016). In Scotland, the UK nearly 10% of the population who are above 65 years of age is found to be severely frail along with 42% of the population in pre-frail stage (ihub.scot, 2019). This indicates that a considerable part of the elderly population in Scotland, UK are suffering from frailty issues and require effective person-centred care approach to enhance their health and well-being. The inter-agency working is found to create effective person-centred care integration for frail elderly as well as others as it leads to include professionals from different agency with wider expertise to plan and deliver quality and improved care. In the study by O’Donnell et al. (2019), it is mentioned that improved inter-agency collaboration and working is consistently effective to deliver integrated and person-centred care for frail older people. This is because improved intervention supported through inter-agency working such as developing frailty index to improve common understanding of associated risk among people regarding frailty, developing direct referral pathway for the general care practitioners to Rapid Access Treatment in the hospital, maintaining bi-directional flow between acute care settings and rehabilitation sites and integrated community care teams are effective to promote enhanced care support for the patients. It is evident as the general care practitioners are the primary healthcare professionals who detect extent of frailty and assumes required support for the elderly patients. The connection of the primary general care practitioner in referring frail adults to the hospital would create effective person-centred care for the patient through inter-agency working in timely manner (Greco et al., 2019). This is because detail institutional care support is to be received by the frail elderly which is specific to their health condition under supervision of the team of specialist in the hospital. Moreover, this would be provided based on the initial report of their frailty by the general practitioners who are not alone knowledge to the extent to deliver person-centred institutional care to the frail elderly.
The bi-directional care flow between hospital and rehabilitation centre for the frail elderly as mentioned by O’Donnell et al. (2019) is an active inter-agency working approach to provide person-centred care to the individuals. This is because severely frail adults undergo specific treatment in the hospital based on their health complication those on recovering to some extent require transfer to rehabilitation centred or community centre and again on deterioration are to be transferred to the hospital. This chain is to be continued so that hospital beds can be vacant to provide care to other frail elderly and continued person-centred support can be provided to the frail elderly on recovery and discharge from the hospital. It is evident as rehabilitation centre help meeting frail elderly individual’s specific daily needs after recovery from health complication as they are unable to gain full physical efficiency irrespective of their treatment in the older age (Vigorito et al., 2017).
Looking for further insights on Sociodemographic Traits of Risk Families? Click here.
The frail elderly people are seen to have reduced mobility and balance due to which they are prone to experience fall. The fall among the elderly leads to create physical damage such as fracture of limbs, hips and others along with pain in the muscles making them experience deteriorated health condition (Fhon et al., 2016). In the study by Gagen and Bulzacchelli (2020), it is mentioned that improved interagency working between local hospital and community care workers are effective interagency working collaboration in providing person-centred care to the frail elderly in preventing and managing falls among them. This is evident as the local hospitals act as the institutional care responders in delivering support to patients (Hubbard et al., 2017). However, the community care workers play the role to detect, ensure and support effective living condition of the patients (Chen et al., 2018). Thus, through interagency working, the community care workers would be first responders in detecting risk of fall among the frail elderly which would lead to transfer the patients to the local health department for providing them institutional care to avoid chances of further fall. This in turn ensures enhance care support for the frail elderly in getting person-centred care to avoid and prevent fall. In the study by Ward-Griffin (2016), the working between the community nurses and family caregivers for negotiating and managing care of the frail elderly was supported as the action of improved interagency working. This is evident as community nurses are recruited by the local community healthcare authorities who interact with the family members acting as the caregiver for the elderly to share care duties and co-design person-centred care plan for the frail elderly to ensure them utmost quality care and satisfaction. The family caregivers in case of frail elderly often lack concept regarding the way to support the individuals on everyday purpose as they lack effective health education regarding care management of frail individuals. The community nurses educate the family members regarding the way to continue person-centred care for the elderly in their absence (Llano et al., 2016; Bélanger et al., 2017). Moreover, by working in connection with the family caregiver, the community nurses learns regarding the cultural preferences and customs to be maintained in care for the frail elderly to offer them enhanced person-centred care which meets all their basic needs without violating their cultural preferences and customs (Bélanger et al., 2017).
The family support along with implication of telephone support service creates an improved inter-agency working activity which is able to support improved person-centred care for the frail adults. This is because the family members are closely related to the frail elderly and they have effective perception of the personal needs of the patients. However, the family members due to lack of health education are seen to show inability in providing care as per personal needs of the frail elderly. In this condition, the telephone support services which are provided by the local healthcare can be used to access immediate assistance for physical care for the frail elderly to avoid any deterioration of their health and enhance their well-being by meeting their specific person-specific needs (Ploeg et al., 2016). Moreover, the telephone assistance services can be used as respite care to report any health deterioration of the frail elderly to ensure them emergency temporary care to be received with active involvement of the family members and the local health authorities (Ploeg et al., 2016). Thus, interagency working of the implementing telephone support by the community healthcare to work in line with family carers in support frail elderly patients is an effective interagency working approach that enhances effective person-centred care to be received by the patients.
he Adult Support and Protection (Scotland) Act 2007 is one of the legislative policy that support improved interagency working to be implemented to provide care to the frail elderly. The Act mentions that the Adult Protection Committees must review practices and procedures of the public bodies such as relevant local Health Boards, Police Services of Scotland and others and work in collaboration with them to ensure safeguarding of adults under all purpose within the country. The Act also mentions that it is duty of the Scottish Ministers to develop an improved code of practice that is to be followed by health professionals along with public officers in delivery care and support to the frail elderly so that they are avoided to get harmed under any condition (legislation.gov.uk, 2007). According to the Act, a public guardian is to be recruited for looking after finances and funds of the frail elderly so that they can be financially protected from any fraud by others who would execute harassment by trying to taking advantage of their frail condition (legislation.gov.uk, 2007). In the study by Shao et al. (2019), it is mentioned that frail elderly due to their health condition often face harm and abuse from others in the society as well as experience financial fraud as people take advantage of their frail condition. However, the current principles of the Adult Support and Protection (Scotland) Act 2007 ensures creating an effective protective interagency working to ensure holistic safeguarding of the elderly in turn assuring them better health condition. This is evident as the Act mentions the way different local agencies are to work with the government to ensure protective care for the elderly in Scotland.

Conclusion
The above discussion mentions that different between multi-agency and inter-agency working is that the later involves more than one agency which collaborates in planning and delivering care whereas the multi-agency working involves joint planning and coordinated delivery of care to patients for enhancing their well-being. In Scotland, UK, it is seen that the number of frail elderly represented 10% of the population making them a significant vulnerable group who require effective care assistance. This is because frail elderly are often seen to be unable to take their own care out of physical weakness. In this condition, the improved inter-agency working is seen to be effective. This is because collaborative working of the hospitals with the rehabilitation centre helps to create an effective approach where the frail elderly after recovery from any health issues in the hospital is able to get continued and enhanced person-centred care at the rehabilitation centre. Moreover, improved interagency working involving the family carers and community nurses is seen to create enhanced person-centred care support for the frail elderly. This is because the family carers share personal needs of the elderly and the nurses educate the family members to accordingly deliver person-centred support to the patient where the care services meet the key needs of the patients. Moreover, it also leads nurses to get educated about the way cultural aspects to be abided in the person-centred care for the frail elderly making them deliver satisfactory care to the individuals where their cultural and religious needs are at met.
References
Bélanger, L., Bourbonnais, A., Bernier, R. and Benoit, M., 2017. Communication between nurses and family caregivers of hospitalised older persons: a literature review. Journal of clinical nursing, 26(5-6), pp.609-619.
careinfoscotland.scot 2019, Legislation protecting people in care, Available at: https://careinfoscotland.scot/topics/your-rights/legislation-protecting-people-in-care/community-care-and-health-scotland-act-2002/#:~:text=The%20Act%20was%20amended%20in,condition%2C%20by%201%20April%202019. [Accessed on: 8 September 2020]
Chen, C.Y., Gan, P. and How, C.H., 2018. Approach to frailty in the elderly in primary care and the community. Singapore medical journal, 59(5), p.240.
Clouston, T.J., Whitcombe, S.W., Jenkins, J. and Mears, J., 2018. Evaluation of interprofessional working on a therapist/nurse-led rehabilitation ward for older people in Wales. International Journal of Therapy And Rehabilitation, 25(4), pp.193-197.
Fhon, J.R.S., Rodrigues, R.A.P., Neira, W.F., Huayta, V.M.R. and Robazzi, M.L.D.C.C., 2016. Fall and its association with the frailty syndrome in the elderly: systematic review with meta-analysis. Revista da Escola de Enfermagem da USP, 50(6), pp.1005-1013.
Gagen, T.M. and Bulzacchelli, M.T., 2020. Improving Local Service Delivery to Prevent Falls in Community-Dwelling Older Adults: Translating Research to Practice. The Gerontologist.221.pp.20-34.
gov.scot 2019, A National Clinical Strategy for Scotland, Available at: https://www.gov.scot/publications/national-clinical-strategy-scotland/pages/4/ [Accessed on: 8 September 2020]
Greco, E.A., Pietschmann, P. and Migliaccio, S., 2019. Osteoporosis and sarcopenia increase frailty syndrome in the elderly. Frontiers in endocrinology, 10, p.255.
Gustafson, D.R., Shi, Q., Thurn, M., HOLMAN, S., Minkoff, H., Cohen, M., Plankey, M.W., Havlik, R., Sharma, A., Gange, S. and Gandhi, M., 2016. Frailty and constellations of factors in aging HIV-infected and uninfected women-the women's interagency HIV study. The Journal of frailty & aging, 5(1), p.43.
Hubbard, R.E., Peel, N.M., Samanta, M., Gray, L.C., Mitnitski, A. and Rockwood, K., 2017. Frailty status at admission to hospital predicts multiple adverse outcomes. Age and ageing, 46(5), pp.801-806.
ihub.scot 2019, The Frailty at the Front Door Collaborative, Available at: https://ihub.scot/media/6870/201912-frailty-at-the-front-door-collaborative-impact-report-v10.pdf [Accessed on: 8 September 2020]
legislation.gov.uk 2007, Adult Support and Protection (Scotland) Act 2007, Available at: https://www.legislation.gov.uk/asp/2007/10/section/58 [Accessed on: 8 September 2020]
Llano, P.M.P., Santos, F.D., Rodrigues, M.C.T., Lemões, M.A.M., Lange, C. and Santos, S.S.C., 2016. The family in the care process of an elderly after a fall accident. Revista de Pesquisa: Cuidado é Fundamental Online, 8(3), pp.4717-4724.
O’Donnell, D., Shé, É.N., McCarthy, M., Thornton, S., Doran, T., Smith, F., O’Brien, B., Milton, J., Savin, B., Donnellan, A. and Callan, E., 2019. Enabling public, patient and practitioner involvement in co-designing frailty pathways in the acute care setting. BMC Health Services Research, 19(1), p.797.
Ploeg, J., Biehler, L., Willison, K., Hutchison, B. and Blythe, J., 2016. Perceived support needs of family caregivers and implications for a telephone support service. Canadian Journal of Nursing Research Archive, 33(2).pp.43-61.
Pugh, M., 2017. A Recipe for Justice: Support for a Federal Food Group Justice Interagency Working Group. Food & Drug LJ, 72, p.341.
Shao, J., Zhang, Q., Ren, Y., Li, X. and Lin, T., 2019. Why are older adults victims of fraud? Current knowledge and prospects regarding older adults’ vulnerability to fraud. Journal of elder abuse & neglect, 31(3), pp.225-243.
Soysal, P., Stubbs, B., Lucato, P., Luchini, C., Solmi, M., Peluso, R., Sergi, G., Isik, A.T., Manzato, E., Maggi, S. and Maggio, M., 2016. Inflammation and frailty in the elderly: a systematic review and meta-analysis. Ageing research reviews, 31, pp.1-8.
Tanaka, T., Takahashi, K., Hirano, H., Kikutani, T., Watanabe, Y., Ohara, Y., Furuya, H., Tetsuo, T., Akishita, M. and Iijima, K., 2018. Oral frailty as a risk factor for physical frailty and mortality in community-dwelling elderly. The Journals of Gerontology: Series A, 73(12), pp.1661-1667.
Vigorito, C., Abreu, A., Ambrosetti, M., Belardinelli, R., Corrà, U., Cupples, M., Davos, C.H., Hoefer, S., Iliou, M.C., Schmid, J.P. and Voeller, H., 2017. Frailty and cardiac rehabilitation: A call to action from the EAPC Cardiac Rehabilitation Section. European journal of preventive cardiology, 24(6), pp.577-590.
Ward-Griffin, C., 2016. Negotiating care of frail elders: Relationships between community nurses and family caregivers. Canadian Journal of Nursing Research Archive, 33(2).pp.63-81.
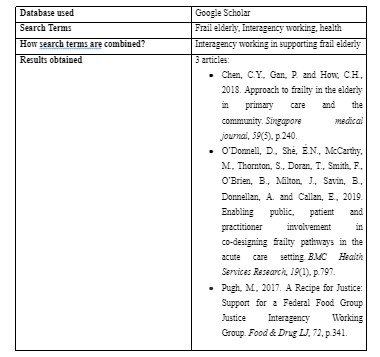
Appendix 1:
Continue your exploration of Integrating Behavioral And Cognitive Theories with our related content.



- 24/7 Customer Support
- 100% Customer Satisfaction
- No Privacy Violation
- Quick Services
- Subject Experts