Quality Assurance in Health Care Management

Figure displays the PRISMA diagram which depicts the search results and outcomes in each stage of review (Liberati et al, 2009). The initial search produced a total of 121 studies, with 6 additional records from other databases, as indicated in the methodology used in this study. After careful selection and removal based on repetition of the studies, 64 studies remained. This called for a further scrutiny, which prompted the screening of the records. Using the inclusion and exclusion criteria, a further examination on the records was conducted and 55 texts were excluded from the review. CASP was also used to eliminate some of the studies, this resulted into a final 5 articles. This method of appraisal incorporates the use of checklist queries in the evaluation of articles to be reviewed, especially those which adopt quantitative methods of research. This method ensured the validity, credibility and the quality of the articles used in this study. If you need quantitative dissertation help, then this is the method that can assist in ensuring the quality of your research.
Five studies met all the qualities that were necessary to tackle the research topic. The inclusion and exclusion criteria provided a strong foundation that helped arrive at this conclusion. The application of this criterion (as shown in the methodology section as well as the PRISMA diagram), enabled the exclusion of a number of potential studies and factored the arrival at the number 5. Those five studies used are as shown in the table; table 1.

Critical Appraisal tool
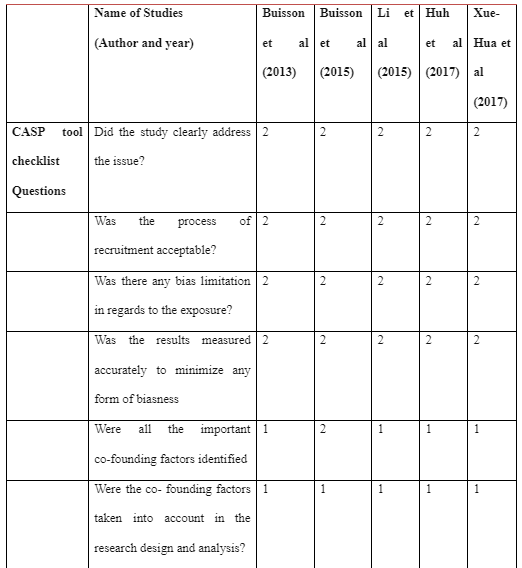
The CASP tool was used in analyzing the quality and credibility of the articles for review. This method confirmed the suitability and validity of the methodology of the selected records. This tool of analysis is always considered the most appropriate and suitable for cohort studies as it provides for a checklist which ensures that the evaluation conducted results into the best quality, concurrent with validity. In order to facilitate easy comparison and reading, the CASP evaluation entailed more closed- end questions. Diffusion weighted MR Enterography studies, as selected, prove to be specific and of quality methodology and findings. Study no. 2 scored the highest with 18 upon the application of this tool (See table 2)

Aims and Research design
For the purposes of the current study, randomized controlled trials were not suitable. Although randomized controlled trials are considered as the gold standard designs for clinical research, it was necessary to adopt prospective quantitative research in this review. The fact that the studies selected were prospective in nature ensured their credibility and applicability of the findings. This prospective nature also restricted the possibility of biasness and assured the results of the validity, due to the acquisition of data in real time (Euser et al, 2009). However, prospective studies always require careful interpretation because of the data that may be collected in the absence of follow up data (Song & Chung, 2010). Prospective studies often lack follow up, thereby making the long term effects of the study difficult project, necessitating careful interpretation of the present data.

Study by Buisson et al (2013) conducted cohort trials on patients with Crohn’s disease. Within a span of around 3 months, these participants were prospectively and consecutively involved in the process. Through these trials, the study sought to examine the apparent diffusion coefficient threshold. The study sought to estimate the inflammation in the small bowel Crohn’s disease by looking at and comparing two main factors: diffusion weighted MR Enterography and the conventional MR Enterography through inter- observer agreements.
In the 2nd study, Buisson et al (2015), the study looked at an ileocolonoscopy and a much more informative ileocolonoscopy with the presence of the Index of Severity and a simplified score for the condition endoscopically. In doing so, they aimed at evaluating the accuracy and efficacy of diffusion- weighted MR Enterography in patients with Crohn’s disease in instances of neither rectal enema nor bowel cleansing. Patients in this case were also carefully selected, the patients selected underwent diffusion weighted MR Enterography consecutively and prospectively.
Huh et al (2017) conducted controlled studies which were undertaken following a period of 1- 2 years of therapy or psychological treatment. The patients selected prospectively went through MRE, which also included MRE including Diffusion weighted imaging (b= 900 s/mm2). Index lesions were prospectively defined; this referred to a contiguous inflamed area selected from the bowel segments of the inflamed anatomy; 1-4 index lesions per person. This was meant to systematically evaluating the performance of diffusion weighted imaging in the monitoring of inflammation in the bowel taking into account the treatment methods on Crohn’s disease. Li et al (2015) in their study assessed how diffusion weighted MR imaging is effective in the evaluation of inflammatory activity in people with Crohn’s disease. Controlled studies were also undertaken in this study. Patients with pain in the abdomen underwent MRE and CD was confirmed in all cases through criteria, such as that which includes endoscopic, histological and clinical aspects. Xie- hua et al (2017) opted to compare diffusion weighted MRI to conventional MRE so as to obtain a validated conclusion on the efficiency of diffusion weighted MRE in the evaluation of Crohn’s disease aimed at assessing the accuracy of Diffusion weighted MRI when it comes to evaluating ileocolonic Crohn’s disease inflammation. The study adopts a prospective and systematic observational study. The selected population underwent both ileoconoloy. Findings from the study were respective in segments and the score by simplification was prospective and qualitative in its own nature.
Population
The participants used in the study were chosen in line with the inclusion criteria (see methodology section). For instance, none of the participants chosen were children. The reviewed studies also excluded patients with different other conditions, this is in regards to beneficence and the preservation of the quality of life of the participants. The sample population and size of a study enables the determination of the reliability of the study. There is a larger degree of certainty where there is a larger population sample used (Hobart et al, 2012).
In study 1, Buisson et al (2013) used a total of 31 adult participants. 31 patients with Crohn’s disease were prospectively and consecutively involved in the study within a period of around three months. In the 2nd study, Buisson et al (2015) involved a total of 44 adult patients in their research. These patients with Crohn’s disease were involved in prospective and consecutive diffusion weighted MR Enterography in the quest to determine its efficiency in the evaluation of the condition.
The prospective study conducted by Huh et al (2017) involved the random selection of 18 adult patients; 13 male and 5 female. In Li et al (2015), 92 patients were initially included in the process, these participants’ selections were based on abdominal pains. 45 patients were, however, excluded from the final study on the basis of relevance to the Crohn’s disease. A total of 47 adult participants were, therefore, used in the study; 29 men and 18 women. These participants had Crohn’s disease confirmed by endoscopic, standard clinical or histologic methods and were therefore involved in the prospective study. In the last reviewed study, Xie- hua et al (2017), 43 consecutive participants were subjected to both MR Enterography with Diffusion Weighted imaging and ileocolonoscopy.
Imaging criteria
The imaging criteria used in all the reviewed studies were several. These differences were as a result of the different points of focus of the studies. Buissons et al (2013), focused on the detection of digestive segments with the most severe lesions. After the detection of such segments, the apparent diffusion coefficient would then be calculated from the process. The results collected, both qualitative and quantitative in nature, would then be compared with conventional MR Enterography with independent activity predictors and score calculations involved. These score calculations and predictors of activity constituted the Magnetic Resonance Index of Activity. The examinations were done independently from each other and interpreted by two different radiologists. Buisson et al (2015) in evaluating the accuracy of diffusion weighted magnetic resonance enterography calculated the Clermont score calculation and the apparent diffusion coefficient. In regards to ileocolonoscopy, calculation was done on the simplified Endoscopic score for Crohn’s disease (SES-CD) and the disease Endoscopic Index of Severity (CDEIS).
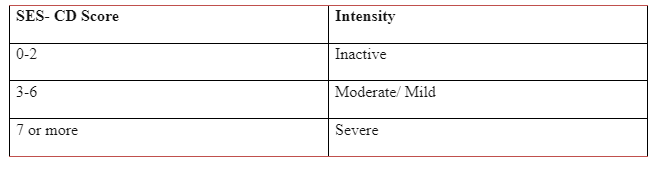
Huh et al (2017) focused on prospectively defining index lesions, these lesions were assessed before and after treatment in MR Enterography and endoscopy. The Crohn’s disease MR Enterography activity index and the endoscopic results were used as the reference standards of the study. The study conducted visual assessments of the treatments and the responses on Diffusion weighted Imaging in three basic stages; changes in inflammation, remission and the changes in the apparent diffusion coefficient. The study by Li et al (2015), used conventional MR Enterography findings and the Diffusion Weighted Imaging signal intensities in coming up with the overall findings. The Diffusion weighted imaging intensities were qualitatively scored so as to determine the efficacy of the procedure. These intensities were qualitatively scored within a range of 0 and 3 and there was a consequent analysis of the correlation between both the apparent diffusion coefficient (ADC) and MR imaging scores and the Crohn’s disease activity index (CDAI). Xue- Hua et al (2017) subjected the same intensity ranges; simplified endoscopic score was used in respective segments endoscopic disease activity; for Crohn’s disease (SES- CD). Activity for most of these studies was graded in the following manner:
Reference standard
For study 1, Buisson et al (2013) the reference standard used for the participants was the apparent diffusion coefficient threshold which was used to differentiate between active and non- active Crohn’s disease. In the 2nd study, the reference standard used was both enterocolonography and ileocolonoscopy findings. All 44 participants consecutively and prospectively underwent diffusion weighted magnetic resonance enterocolonography and ileocolonoscopy. Study 3 also referred to apparent diffusion coefficients of the normal and the inflamed bowels. In study 4 by Huh et al (2017), the reference standard was prospective MR Enterography including DWI and ileocolonoscopy. The final study used ileocolonoscopy as the reference standard as they assessed the accuracy of DWI in evaluating ileocolonic CD inflammation.
Imaging Interpretation and Diagnostic Accuracy
Throughout the reviewed studies, examination interpretation was done independently by radiologists blinded for clinical assessments. In the 1st study; Buisson et al (2013); two radiologists in the clinical assessment, conducted independent interpretations of the findings. In Huh et al (2017), the examination and interpretation of the treatment before and after was performed by 2 independent readers. In Buisson et al (2015), independent radiologists evaluated the results and aided in the conclusion making. In Xue- hua et al (2017), the changes in values of measurements of the apparent diffusion coefficients were monitored and evaluated by independent radiologists. This portrayed a similar circumstance in Li et al (2015). The reference standards used were the endoscopic findings and the MR Enterography Activity index obtained in the procedure.
On diagnostic accuracy, the test varied in differentially throughout the five studies. The accuracy of the diagnosis percentages and validity greatly depend on the assessment specificity and sensitivity (Preston et al, 2015). In Li et al (2015) the diagnostic accuracy of the activity of the Crohn’s disease was determinable through analysis of the receiver- operating characteristic curve. General specificity rates varied from 78-100% and sensitivity rates from 86-100%; the table below expounds on the rates

Discussion
Overall findings
The methodology implemented in this review selected all the relevant studies in relation to the research statement. Specificity and sensitivity rates were used in all studies reviewed to measure the diagnostic accuracy of the Diffusion weighted MR Enterography findings. The aim of this study was to determine the efficiency of diffusion weighted MR Enterography in the evaluation of Crohn’s disease.
High rates of specificity and sensitivity were recorded in an analysis of all the studies. Furthermore, the overall analysis indicates high accuracy and effectiveness of diffusion weighted MR Enterography in the evaluation of the Crohn’s disease in the adult participants. These findings have been supported by further literature on the same and even in comparison analyses with other alternative methods of evaluation, such as ileocolonoscopy. There were significant positive correlations between scores of Diffusion Weighted Imaging and the Crohn’s disease Activity indices across all studies; r=0.74, P0.001 in Li et al (2015).
Comparison of the findings
The 1st study, Buisson et al (2013) selected a total of 31 adult participants. 54.8% of the participants had active Crohn’s disease with the score of either 7 or more as in the Magnetic Resonance index of activity. Activity evaluated using conventional MR Enterography (p= 0.001) depicted high correlations with DWI hyper intensity. DW sequences through qualitative analysis presented values of 94.4% on the positive predictive values and 100% on the negative predictive values. Both quantitative and qualitative analyses depicted high values of sensitivity and specificity. Buisson et al (2015) present an inverse correlation on apparent diffusion coefficients with the segmental Crohn’s disease Endoscopic Index of Severity (-0.48; p< 0.001). This correlation also reflects on the Simplified Endoscopic Score for Crohn’s disease (-0.44; p0.001). As the ulcerations increased, the segmental apparent diffusion coefficients decreased (p=0.0001). The higher the ulcerated segments, therefore, the higher the Clermont score (23.3 +/-8.4). These detections and evaluations still reflected high levels of sensitivity and specificity.
From the 3rd study, Huh et al (2017) display significant differentiations between unimproved and improved lesions (p=0.022 for reader 1 and p=0.025 for reader 2). The diagnostic accuracy of DWI in the study in improved lesions; diagnosis on improved inflammation and complete remission; had the range of 76% to 84% (28/37 and 31/37). Both readers also noted a significant negative correlation between Crohn’s disease MR activity index and the apparent diffusion coefficient (-0.461 and -0.438 respectively, p<0.05). 166.93+/- 100.89 was the mean of the Crohn’s disease Activity index in Li et al (2015) (<150 in 22 participants and >149 in 25 participants). The signal intensity of DWI was significantly higher in active Crohn’s disease compared to that of inactive Crohn’s disease (median= 3, compared to median= 1). Xue- hua et al (2017), had accumulated 185 bowel segments which included inactive, mild and severe ileo- colonic segments. These were retrieved from 43 adult participants. The Simplified Endoscopic Score in regards to Crohn’s disease correlated strongly with the apparent diffusion coefficient values (r= 0.880). Across all results, the specificity and sensitivity values were highly recognizable and the accuracy of the results was clinically acceptable.
Application to clinical practice
This method; Diffusion weighted MR Enterography; has been widely applied in the evaluation of Crohn’s disease. Diffusion weighted MR Enterography assess the activity of Crohn’s disease from a more direct level (Hordonneau et al, 2014). Inactive Crohn’s disease depict higher ADCs and lower b value Diffusion Weighted Imaging levels with less markedly reduced diffusion, compared to the bowel segments of active Crohn’s disease. This is based on hyper intensity. Reductions in extracellular space from factors such as granuloma formation, increased cell density and lymphatic channels that are dilated constitute the mechanism in which there is restricted diffusion of the water molecules.
DWI, as a tool, is increasingly attractive in the assessment of Crohn’s disease (Yu et at, 2019). This tool is both a noninvasive and radiation free tool and as an optional sequence to the MR Enterography, it has proved its effectiveness in clinical research in its quantitative modality for the evaluation of bowel inflammations.
The result from these prospective longitudinal studies have indicated that Diffusion weighted MR Enterography is a feasible tool in the monitoring of inflammations in the bowel. This is even more accurate when it comes to patients with Crohn’s disease. This is possible because of the linear manner of change of ADC in accordance with the bowel inflammation changes that occur as a result of treatment.
The accuracy of the diffusion weighted MR Enterography is however limited to the extent of its nature. Diffusion weighted MR Enterography is more expensive, compared to other alternatives methods of evaluation. This process is also limited as to availability, for instance the general application of MR Enterography in Crohn’s disease as shown by Castiglione et al (2013). DWI facilities are more difficult to access and often neurology, orthopedic or rheumatology departments have priority as to the access. According to Greenup et al (2016), there are also other possible limitations such as the possibilities of bowel distensions and reduced quality of the images that come up on evaluation.

Study limitations
The inclusion and exclusion criteria used in the study pointed towards the use of only English- language studies. This concept or criteria may have been bias to the extent of only English language studies. In as much as the criteria enables the clarity and unambiguity of findings as only those studies in the English language have been looked at, the study is also limited as to relevance. Relevant data and information on the topic may have been overlooked.
The study only focused on cohort prospective reviews. This is disadvantageous in as far as applicability of the findings is concerned. From an applicability point of view, prospective studies often have no follow up findings. This would mean that the long term effects of the research or reviews are usually not determined. This fact makes it hard to interpret and protectively conclude on the findings. As earlier stated, data on all the prospective studies have to be more critically analyzed so as to come up with conclusive information on the research topic.
Recommendations to future research and clinical practice
Evidently, there are various areas in which research and practice on the effectiveness of MR Enterography may be improved. The clinical significance of Diffusion weighted MR Enterography must first of all be acknowledged. Diffusion weighted MR Enterography is notably very effective in the evaluation of Crohn’s disease and this fact should therefore be foundationally embraced in clinical practice. This applies to both clinical research and practice
The reference standards of prospective studies should be improved to increase the possibility of collection of more data, suitable in details in clinical research. RCT studies, with the gold standard of methodology in clinical research, should be accommodated in diffusion weighted MR Enterography research so that the data collected may be regarded as the highest quality data and the applicability be assured in clinical practice (Houle, 2015). Furthermore, in order to ascertain the inclusion of scientific techniques and procedures in standard imaging techniques, more prospective studies should be conducted with appropriate reference standards (Greenup et al, 2016).
Conclusion
According to Buisson et al (2013) the detection and assessment of inflammation in the small bowel Crohn’s disease is well done by MR Enterography. Its effectiveness entails a well-tolerated and non- time- consuming method of assessment which presents a very degree of accuracy. In the indirect detection of endoscopic ulcerations, using he Clermont scores and apparent diffusion coefficients in diffusion weighted MR Enterography is very effective (Buisson et al, 2015)
Diffusion Weighted MR Enterography quantitatively and qualitatively monitors bowel inflammation in Crohn’s disease both before and after medical treatment. As a result of DWI, inflammatory activity is accurately graded in patients with ileocolonic Crohn’s disease. The activity of Crohn’s disease may therefore be best monitored through this process (Xue- hua et al, 2017). Summarily, therefore, the usefulness and effectiveness of DWI covers a great length in the detection and localization of active Crohn’s disease. Across all studies, the apparent diffusion coefficients and DWI correlate well with the activity of Crohn’s disease during the evaluation. As a result, the specificity, sensitivity and accuracy of the results were excellent in the differentiation of active Crohn’s disease from inactive Crohn’s disease (Li et al, 2015).
References
- Buisson A., Joubert A., Montoriol F., Ines D., Hordonneau C., Pereira B., Garcier J., Bommelaer G., Petitcolin V. Diffusion‐weighted magnetic resonance imaging for detecting and assessing ileal inflammation in C rohn's disease. Alimentary pharmacology & therapeutics. 2013 Mar;37(5):537-45.
- Buisson A., Hordonneau C., Goutte M., Boyer L., Pereira B., Bommelaer G. Diffusion‐weighted magnetic resonance imaging is effective to detect ileocolonic ulcerations in Crohn's disease. Alimentary pharmacology & therapeutics. 2015 Aug;42(4):452-60
- Castiglione F., Mainenti P., De Palma G., Testa A., Bucci L., Pesce G. Noninvasive Diagnosis of Small Bowel Crohn’s Disease. Inflamm Bowel Dis. 2013
- Euser A., Zoccali C., Jager K., Dekker G. Cohort Studies: Prospective versus Retrospective. Nephron Clin Pract. 2009; 113 (3): c214-7. Doi: 10.1159/000235241
- Greenup A., Bressler B., Rosenfeld G. Medical Imaging in Small Bowel Crohn’s Disease- Computer Tomography Enterography, Magnetic Resonance Enterography and UltraSound. Inflamm Bowel Dis. 2016
- Hobart J., Cano S. Warner T., Thompson A. What sample sizes for reliability and validity studies in neurology? J Neurol. 2012: 259 (12): 2681- 94
- Hordonneau C., Buisson A., Scanzi J. Diffusion- weighted magnetic resonance imaging in ileocolonic Crohn’s disease: validation of quantitative index of activity. Am J Gastroenterol. 2014
- Houle S. An introduction to the fundamentals of randomized controlled trials in pharmacy research. Can J Gastroenterol Hepatol. 2016
- Li H., Sun H., Mao R., Zhang W., Jiang S., Pui H., Chen H., Li ZP. Assessment of activity of Crohn disease by diffusion-weighted magnetic resonance imaging. Medicine. 2015 Oct;94(43).
- Liberati A., Moher D., Tetzlaff J., Altman D. Preferred Reporting Items for Systematic Reviews and Meta Analyses: The PRISMA statement. Ann Intern Med. 2009; 151 (4): 264. Doi 10.7326/0003-4819-151-4-200908180-00135
- Huh, J., Kim, K.J., Park, S.H., Park, S.H., Yang, S.K., Ye, B.D., Park, S.H., Han, K. and Kim, A.Y. Diffusion-weighted MR enterography to monitor bowel inflammation after medical therapy in Crohn's disease: a prospective longitudinal study. Korean journal of radiology. 2017, 18(1), pp.162-17
- Song J., Chung K. Observational studies: cohort and case control studies. Plast Reconstr Surg. 2010; 126 (6)
- Preston L., Carrol C., Gardois P., Kaltenthaler E. Improving Search Effciency for Systematic Reviews of diagnostic test accuracy: an exploratory study to assess the viability of limiting to MEDLINE, EMBASE and reference chencking. Syst Rev. 2015
- Xue-hua Li, Can-hui Sun, Ren Mao, Si-yun Huang, Zhong-wei Zhang, Xu-feng Yang, Li Huang, Jin-jiang Lin, Jian Zhang, Shomron Ben-Horin, Shi-ting Feng, Min-hu Chen, Zi-ping Li, Diffusion-weighted MRI Enables to Accurately Grade Inflammatory Activity in Patients of Ileocolonic Crohn's Disease: Results from an Observational Study, Inflammatory Bowel Diseases, Volume 23, Issue 2, 1 February 2017, Pages 244–253
- Yu H., Shen Y., Tan F., Zhou Z., Li Z., Hu D., Morelli J. Quantitative diffusion- weighted magnetic resonance enterography in ileal Crohn’s disease: a systematic analysis of intra and interobserver reproducibility. World Journal of Gastroenterology. Baishideng Publishing Group Inc. 2019
Dig deeper into Mechanism of Homeostatic Glucose Control with our selection of articles.



- 24/7 Customer Support
- 100% Customer Satisfaction
- No Privacy Violation
- Quick Services
- Subject Experts