Non-Adherence to Haemodialysis Treatment: Barriers, Consequences
Introduction
According to National institute of Health and care excellence (NICE) guidelines kidney disease is a worldwide public health problem. Dialysis is the supportive treatment for patients with CKD which requires patients’ commitment and considerable time for their treatment. Dialysis facilitates the excretion or removal of the toxic and harmful metabolic from the human body. However, the poor compliance of patients negatively influences its effects (J.W and P.Y. 2017) Noncompliance to prescribed treatment among patients receiving haemodialysis is very common and is associated with significant mortality and morbidity. At least 50% of haemodialysis patients believed to be non-adherent to some part of them treatment. (Ibrahim S,Hossam M,Belal D.,2021). Non-adherent to dialysis treatment results in irreversible consequences such as bone demineralisation, Pulmonary embolism, and metabolic disorders and which leads to the development of cardiovascular disorders and finally, death. (Denhaerynck et al.,2003) If you require assistance with a healthcare dissertation help, do not hesitate to reach out to us for support.
The World health organisation defines adherence as the extend which a person’s behaviour (taking medications, following the recommended diet and or executing lifestyle changes) corresponds with the agreed recommendations of the health care provider. (WHO, 2020; p:13) According to National kidney foundation dialysis outcome and quality initiative (KDQI) guidelines the measures for non-adherences include missed treatment, shortened dialysis time, Interdialytic weight gain (IDWG), serum phosphorus, treatment adequacy (Kt/V) and serum albumin. Worldwide nonadherence rates range from 8.5% to 22%and have been reported as high as 86%. (Haemodialysis international 2010). During clinical work as a staff nurse in a haemodialysis unit in Northern Ireland Nonattendance to dialysis or shortening dialysis times are very common and several factors identified to be the reasons this noncompliance, which include health belief, illness perceptions, social and family support etc (Chenitz et al., 2014) (Appendix 1). Assessing adherence among haemodialysis patients will allow healthcare providers to implement interventional methods to minimise health and economic consequences of non-adherence. (Naalweh et al; 2017). Therefore, it is important to identify the barriers of noncompliance to haemodialysis treatment and explore interventions to improve compliance.

RATIONALE
Haemodialysis is the procedure performed by using a special filter and dialysis machine to remove impurities from the blood in people with chronic kidney disorder (CKD) as their kidney fail to perform the function of filtering waste from the blood (). As of 2020, there are nearly 3000 people considered to be suffering from CKD in the UK and nearly 30,000 of them involve in accessing dialysis as part of the treatment of the disorder (kidneycareuk.org, 2020). It is informed that many people in UK show hindered compliance to haemodialysis required for treatment of CKD condition in patients. This is because the uncertain fluctuations in the physical and cognitive well-being along with increased restriction and emotional effect of haemodialysis makes them show non-compliance in accepting the treatment (Jones et al., 2018). In global condition, the non-compliance towards haemodialysis widely extends. This is evident from the study of Alhawery et al. (2019) which is performed in Saudi Arabia with 265 patients included from different hospitals in the country and who are suffering from CKD. The data revealed that non-adherence or non-compliance rate for participants who entirely avoided the dialysis session is 25% and those that missed at least one session of haemodialysis was 75%. The rate of non-compliance for haemodialysis is identified in mostly men than women and who are smokers. This indicates that high non-compliance among CKD patient are faced in global context for haemodialysis instead it is the effective treatment available for them to manage CKD efficiently.
The non-compliance of patients towards accessing haemodialysis is an issue because the lack of dialysis causes build-up of toxins in the body which with times create a condition known as uremia. The presence of uremia gradually causes kidney failure and leads individuals to experience seizures, heart attack, lack of consciousness and others (Gerogianni et al., 2018). The uremia development as a result of hinder haemodialysis causes acidosis as increased acids are build-up in the blood because they not being removed leading individuals to face fatigue, vomiting and others along with breathing problem as symptoms of acidosis (Gagnebin et al., 2020). As argued by ), hindered compliance to haemodialysis among patients with CKD leads them to experience early need of kidney transplant. This is because lack of timely haemodialysis leads to cause damage to both the kidneys leading them required to be replaced through transplantation for living. The lack of effective haemodialysis among the patients leads them to experience issues such as hyperkalemia, hypothyroidism, anaemia and others (Ciceri and Cozzolino, 2021). Thus, the hindered compliance for haemodialysis in patients are focussed to be improved so that they can have better well-being and health. For this purpose, the current study is important to be performed because effective identification of intervention to resolve non-compliance towards haemodialysis in CKD patient would make nurses aware of the actions to be taken for such patient’s good health and well-being.
METHODS
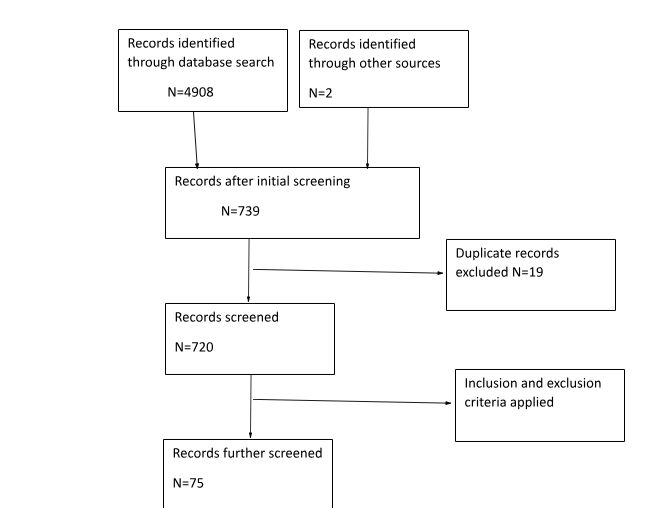
In performing the current study, the electronic search strategy is to be implemented. This is because it is cost-effective as free articles are available in potential medical and healthcare platforms. Moreover, is time-effective as intense manual search are not required and simple use of keywords leads to load of similar articles regarding the topic to identified (). The platforms to be used for performing the search are CINHAL, Embase, Science direct and Medline. This is because the following sites contains wide number of relevant articles regarding any topic related to medical or healthcare aspects. The inclusion criteria considered for the study are articles containing information about haemodialysis patients, written in English, published between 2010-2021 and fully accessible. The exclusion criteria include patients in peritoneal dialysis, published before 2010, not written in English and contains only abstract or proposal. Initially research papers included from Northern Ireland, however this narrowed the search due to the limited study papers. The search is further extended to wider range which lead to obtained 4908 articles from these 4 databases. The search was further refined to 75 by using inclusion and exclusion criteria. These were Embase=20, Medline=9, cinhal=7 and science direct=1. A manual title and abstract scan were used to find papers more relevant to the topic and finally 7 articles were chosen. The Critical Appraisal Skill Programme (CASP) tool is used to critically analyse the papers and determine its credibility to be included in the study. (See appendix 2 and 3)
FINDINGS
In the study, out of the sevemn articles choose it is found that 2 of them are qualitative studies form Philadelphia and United states, 2 are quantitative studies from Jordan and Greece. Qualitative and Quantitative approach to research is grounded in different paradigms (Pilot, Beck&Hungler.,2001) The reliability of quantitative research is enhanced due to its objective nature, (Holland and Rees.,2010) whereas Qualitative research follows a natural paradigm based on reality. (Pilot et al.,2010) and 3 randomized control trial studies are also used in study which are from Australia, Leeds, and Missouri. Out of seven 3 articles focused on the influence of education and quality of life to patient’s adherence to dialysis treatment and 2 papers argued that there was no significant correlation between knowledge and adherence score after the intervention (Alikari et al., 2018, Clark et al., 2014). However some correlation between demographic factors like education level, mental status, quality of life and perceived seriousness of illness to adherence has been identified by Nabolsi et al., 2015.
Take a deeper dive into Socioeconomic Determinants and Patient Profiles with our additional resources.
A quasi-experimental study conducted by Alikari et al (2018) in Western Attica were randomly assigned into intervention. The aim of this study was to test the hypothesis that a nurse-led education intervention may affect the level of knowledge to adherence to treatment regimen. For this study education sessions conducted for patients based on their individual needs in the form of face-to-face through information booklets. This study showed that the education interventions may improve knowledge adherence and health-related quality of life by way of improving information’s and limiting misconceptions about the disease (Alikari et al.,2018). This study emphasised the importance of patient centred approach and mentioned the patients to be considered as partners and is to be effectively informed regarding health issue to make effective clinical decision regarding acceptance kid haemodialysis (Alikari et al., 2018).
A descriptive correlated study was conducted in Jordan to investigate the relationship between quality of life, depression, seriousness of illness and adherence to treatment among patients on maintenance haemodialysis. For this purpose, 244 adult patients were participated in this study and it consisted of 3 phases. First part included identifying sociodemographic factors and Second phase involved socioeconomic factors influence on the haemodialysis while the third phase was to measure the severity of depression in haemodialysis patients (Nabolsi et al.,2015). According to Nabolsi et al (2015) there was a significant relationship between depression and quality of life with no significant relationship found between marital status and quality of life. They mentioned higher the depression the lower the quality of life. Thus, indicating Patients with high quality of life are more adherent to treatments. This study also highlighted that the more patients perceived the seriousness of illness are more adherent to their treatment regimens haemodialysis (Nabolsi et al., 2015).
Murali and Lonergan (2020) tried to explore the barriers to dialysis treatment adherence and interventional strategies to improve adherence. According to this randomized control trial study, the barriers to adherence and interventions depend on 5 different factors that are socio economic, health care system, disease and therapy related factors. This intervention expected to have considerable impact on patient’s adherence to treatment due to socio-economic factor. In healthcare system related intervention, adherence behaviour is evaluated through active monitoring which indicated it would affect patient’s adherence nature. Disease related intervention related to depression which showed management of depression through cognitive therapy and counselling showed a significant improvement in patients’ adherence to treatment. Patient related intervention focused on individual needs person centred care. Murali and Lonergan concluded that better evaluation of adherence barriers helps to plan and implement appropriate interventions.
The effect of motivational interviewing technique in adherence to haemodialysis treatment regimen was evaluated in a pilot study conducted in US. 29 adults participated in this pre and post design study. Adherence date collected from patients for 3 months then motivational interviewing intervention was implemented for 3 months. Out of 29 patients 10 participants excluded due to serious illness of due to lack of guardian approval. Out of 19 participants 5%improvemnat noticed in missed treatments and 9%improvement noticed in shortened treatments. In finding motivational interviewing influence dialysis attendance and shortened treatments. (Nephrology nursing journal., 2011).
Another Quantitative study conducted in Philadelphia during July 2012 and January 2013 including 30 adult participants on HD,15 adherent and 15 non-adherents to determine the patient perception of risk barriers and recommendations to incentre haemodialysis attendance. Patients from both groups mentioned that realise that it is a lifesaving treatment and they are aware of the risk associated with missed treatments (Chenitz et al., 2014). Unreliable transport was the main barrier to attend in centre dialysis treatment mentioned by people from both groups. Family and social support are found to be another barrier to attendance to treatment. Simultaneously in a qualitative study by Clark et al., (2014). the fact is supported by mentioning low social and family support impact upon poor outcome and associated with increased destress and nonadherence to treatment like haemodialysis. The interventions to improve attendance to dialysis suggested by this group are well organised transport system, motivational interviewing, and peer support. This study finding was limited due to small sample size and single geographic region (Clark et al., 2014).
The impact of electronic interventions has been evaluated by Will R Ross in his randomised control trial study conducted in Missouri in 2015 where 22 adult patients participated in the interventional study. The aim of this study was to assess the effect of electronic intervention and compare the number of emergency department visit hospitalisations between groups during intervention. (Will R Ross 2015). The individual’s nonadherence nature was identified prior to intervention and then divided into 2 groups. Group A with occasional nonattendance nature and Group B with frequent nonattendance nature. During this study group A received electronic notifications like messages or calls stating appointment time and details whereas Group B received no notifications. After 8 weeks the cross over took place and study continued for additional 8 weeks. Studies showed that this intervention may improve patient’s adherence to scheduled treatment and increase patients’ satisfaction with their treatments and prevent medical complications associated with missing or shortening of dialysis treatments. (Will R Ross, 2015).
DISCUSSION
Nonadherence to haemodialysis treatment is a major problem among patients undergoing haemodialysis and most studies has focussed on identifying the factors leading to the action but have not determined intervention to manage the action. This review emphasised on patient’s nonadherence to dialysis treatment and interventions which could help to improve adherence behaviour. The health belief and risk perception regarding missed treatments, perception of barriers to haemodialysis attendance and patient’s attitude towards illness are found to be associated with their adherence (Murali et al., 2020). Few other main barriers to patient’s nonattendance to dialysis treatment are depression and associated problems, unreliable transport and lack of motivation to attend scheduled treatments and lack of knowledge about the seriousness of illness and the consequences of missing treatments (Clark et al., 2014). The interventions which help to break these barriers and to improve adherence are discussed in this review.
The patient’s enhanced knowledge on illness and treatment are associated with their higher level of adherence to haemodialysis treatment and thus educational intervention for the treatment is key to limit their non-adherence to treatment (Murali et al.,2020). This is because educational interventions inform patient about their own health status and treatment plans which provides them enhanced understanding to reason and adapt to the disease, treatment, and changes to quality of life (Yangoz et al., 2020). Education intervention enriched with study materials, information booklets, brochures, posters, and video clips are key aspects in making patient interest in participating in the intervention which is helpful for them to show compliance in treatment later. Patient education required to start from the first day of their treatment where they are to be informed about the outcome of every dialysis treatment including the amount of blood volume dialysed, and net fluid removal achieved on each occasion and the importance to attend for next session may help their attendance to next treatment. Regular meeting with patients and their families is important to create awareness in patients. This should include the treatment outcome in monthly basis and monthly bloods results, this may help to improve their knowledge and alleviate misperception regarding illness (Yangoz et al., 2020).
A general consensus has been identified by Nabolsi et al (2015) and Chilcot et al (2013) that poor illness perception and understanding in haemodialysis patients are associated with depression and it hinders their quality of life as well as intent to participate in treatment (Nabolsi et al.,2015). Early diagnosis and effective management of depression and anxiety has shown a significant impact in patient’s nature of compliance to dialysis treatment. (Clark et al., 2014). Thus, depression diagnosis is patients are to be made compulsory and techniques like Cognitive Behavioural therapy, counselling and integrated motivational interviewing are to be used in managing depression and anxiety (Westra et al., 2016).
The lack of motivation is found to be another barrier to patient’s adherence to treatment. Motivational interviewing has shown to be an effective approach to improve and maintain treatment adherence. (Clark et al., 2014). The goal of motivational interviewing is the healthcare provider establish a good rapport with the patient, through an open communication and with the patient and the healthcare provider support individual autonomy creates a desire to change their behaviour. (Miller & Rollnick ,1991). Studies highlighted that a marked improvement in skipped or shortened dialysis treatments through motivational interviewing to adult patients by staff in the dialysis unit. In this approach the health care provider express empathy towards the patient and then helps the patient develop discrepancy between current behaviour and goal or values that are important to the patient. (Nephrology Nursing Journal 2011) Motivational communication by staff in the treatment unit is seemed to be a promise as an intervention to improve adherence in adult patients receiving HD.
The atmosphere of the dialysis unit, attitude of the healthcare provider and the peer group dialysed along with patients is also a factor for their attendance to treatment as they spend average of 15-20 hours per week in the dialysis unit. Thus, effective therapeutic relationships are to be developed between patients and nurses where alternative therapeutic means of adherence can be discussed and follow-up can be planned (Sabate et al., 2001). The entertainment activities like Music, Television, painting or art and craft work while on treatment helps to improve mental status and create interest in patients. Patient empowerment and encouraging them to participate in their own care (shared care) and decision making also helps to promote patient’s autonomy and it is linked to better clinical outcomes and symptom management. Thus, they are to be included to increase patient’s adherence to haemodialysis. Patient-centred approach is necessary in patients with chronic diseases. Main factors to consider are quality of life, life expectancy and management of symptoms. A multidisciplinary team involvement ensures best care to chronically ill patient with complex treatments and difficulty with optimising benefits (Chenitz et al,2014).

CONCLUSION
In conclusion, this literature review explored that early identification of barriers of nonattendance to dialysis treatment and implementation of intervention depending on the nonadherence nature of patients can improve patient’s compliance to dialysis. The better management of symptoms, Education, counselling, motivational interviews and patients support are the most important interventions identified to improve patients attendance to treatment. Patient centred approach is essential to apply these interventions. Regular meeting with Patient and family with healthcare professionals and patient preference questionnaires are beneficial improve patient’s adherence to treatment and for optimisation of treatments.
REFERENCES
Alhawery, A., Aljaroudi, A., Almatar, Z., Alqudaimi, A.A. and Al Sayyari, A.A., 2019. Nonadherence to dialysis among saudi patients–Its prevalence, causes, and consequences. Saudi Journal of Kidney Diseases and Transplantation, 30(6), p.1215.
Asha,P.Nair.,J Silvia Edison.,(2013). Effect of Planned Nursing Interventions on Compliance among Persons Undergoing Maintenance Haemodialysis’, International journal of Nursing education.5(1) pp15-19.
at: https://docs.wixstatic.com/ugh/dded87_25658615020e427dal94a325e773d42.pdf [Accessed:10 November 2021]
Bondemark,L.,Ruf,S.,(2015)`Randomized controlled trials: The gold standard or an unobtainable fallacy’, European journal of Orthodontics,37(5) pp457-461.
CASP UK (2017), Clinical Appraisal Skills programme Quantitative research, available
Ciceri, P. and Cozzolino, M., 2021. Expanded Haemodialysis as a Current Strategy to Remove Uremic Toxins. Toxins, 13(6), p.380.
Cynthia,L.Russel.,Nikole,J.Cronk.,Norma,Knowles.,Michelle,L.Matteson.,Leanne,Peace.,Leonor,Ponferrada.,(2011)`Motivational Interviewing in Dialysis Adherence Study’, Nephrology Nursing Journal,38(3) pp229-236.
Esperanza,Velez-Velez.,Richardo,J.Bosch.,(2015)`Illness perception, coping and adherence to treatment among patients with chronic kidney disease’, Informing Practice and Policy Worldwide through Research and Scholarship, pp849-860.
Gagnebin, Y., Jaques, D.A., Rudaz, S., de Seigneux, S., Boccard, J. and Ponte, B., 2020. Exploring blood alterations in chronic kidney disease and haemodialysis using metabolomics. Scientific reports, 10(1), pp.1-9.
Gerogianni, G., Kouzoupis, A. and Grapsa, E., 2018. A holistic approach to factors affecting depression in haemodialysis patients. International urology and nephrology, 50(8), pp.1467-1476.
Henny, Westra., Michael, J. Constantino.,Martin,M.Antony(2016)`Integrating motivational Interviewing with Cognitive-Behavioural Therapy for Severe generalized Anxiety Disorder: An Allegiance-Controlled Randomized Clinical Trials’, Journal of Consulting and Clinical Psychology, pp1-16.
Holland,K.,Rees,C.,(2010)`Nursing evidence based practice skills,Newyork’,Oxford university press.
Jing,Wang.,Peng,Yue.,Jing,Huang.,Xiaodong,Xie.,Yunhua,Ling.,Li,Jia.,Yunjin,Xiong.,Fang,Sun., (2018). Nursing intervention on the Compliance of Haemodialysis Patients with End-stage Renal Disease: A Meta-Analysis’, Blood purification,45pp102-109.
Jones, D.J., Harvey, K., Harris, J.P., Butler, L.T. and Vaux, E.C., 2018. Understanding the impact of haemodialysis on UK National Health Service patients’ well‐being: A qualitative investigation. Journal of clinical nursing, 27(1-2), pp.193-204.
Kalam,Sh.Naalweh.,Mohammad,A.Barakat.,Moutaz,W.Sweileh.,Samah,W.Al-Jabi.,Waleed,M.Sweileh.,Saed,H.Zyoud.,(2017)`Treatment adherence and perception inpatients on maintenance haemodialysis: a cross sectional study from Palestine’,BMC Nephrology18:178pp109.
Kara,B.Chenitz.,Michael,Fernando.,Judy, A.Shea.,(2014)`In-centre haemodialysis attendance: Patient perceptions of risk, barriers, and recommendations., Haemodialysis international18(2) pp364-373.
Karumathil,Murali.,Maureen,Lonergan.,(2020)`Breaking the adherence barriers: Strategies to improve treatment adherence in dialysis patients’, Seminars in Dialysis,33pp475-485.
kidneycareuk.org 2020, Facts and Stats: Kidney care, Available at: https://www.kidneycareuk.org/news-and-campaigns/facts-and-stats/ [Accessed on: 16 November 2021]
Lais,Margan.,(2001). A Decade review:Methodes to improve adherence to the treatment regimen among haemodialysis patients’, ETDNA/ERCA JOURNAL,xxv11.pp7-12.
Michelle,L.Matteon.,Cynthia,Russel.,(2010)`Interventions to Improve haemodialysis adherence: a systemic review of randomized-controlled trials’, Haemodialysis international,14pp370-382.
Nabolsi,MM.,Lina,Warden.,Jehad,O Al-Halabi.,(2015)`Quality of life, depression, adherence to treatment and illness perception of patients on haemodialysis’, international journal of nursing practice,21, pp1-10.
Sarah,Clark.,Ken,Farrington.,Joseph,Chilcott.,(2014). Non adherence in Dialysis patients: Prevalence, Measurement, Outcome, and physiological Determinants’, Seminars in Dialysis,27(1), pp.42-49.
Sefika,T.Yangoz.,Zeynep,Ozer.,Ilkay,Boz.,(2020)`Comparison of the effect of educational and self management interventions on adherence to treatment in haemodialysis patients: Systemic review and meta-analysis of randomized controlled trials’, international journal of clinical practice,75(e) pp1-19.
Shabu,Abraham.Varghese.,(2018)Socialm Support: An Important factor for treatment Adherence and Health-related Quality of life of patients with End stage renal disease’, Journal of social service research,44(1) pp1-18.
Victoria,Alikari., Maria,Tsironi., Vasiliki,Matziou., Foteini,Tzavella., John,Stathoulis., Fotoula,Babatsikou., Evangelos,Fradelos., Sofia,Zyga.,(2018).The impact of education on knowledge, adherence, and quality of life among patients on haemodialysis’, Springer Nature SwitzerlandAG 2018.
Will,R.Ross.,(2016)`Improving adherence in Renal Dialysis Patients Through Electronic Interventions’, Clinical Trials.gov U.S.National Library of Medicine,pp1-8.
Youngmee, Kim.,Lorraine,S.evangelista.,(2010)`Relationship between illness perception, treatment adherence, and Clinical Outcomes in Patients on Maintenance Haemodialysis’, Nephrology Nursing Journal,37(3) pp271-281.


Dig deeper into Navigating the Seas of Knowledge with our selection of articles.



- 24/7 Customer Support
- 100% Customer Satisfaction
- No Privacy Violation
- Quick Services
- Subject Experts