Bone Structure and Osteoporosis
INTRODUCTION
Osteoporosis is a disease characterized by weak bones making it easy for the bones to break. Bones are tissues found in the body and they are responsible for providing support in terms of structure, storing calcium, and protecting one’s vital organs (Ringle, 2009). The makeup of a bone is comprised of three types of cells with distinct functions namely; osteocytes and osteoblasts which are responsible for support, osteoclasts which are responsible for remodeling and osteoid cells which are mainly responsible for storing calcium. (Sterling, 2000). For students delving into the realm of biology, exploring the aspects of bone structure and diseases such as osteoporosis can be enlightening. Seeking a biology dissertation help offer valuable insights into this area of study.
Bone mineral density (BMD) on the other hand, is the amount of mineral contained in the tissue of a bone. Its test is used to identify the presence of Osteoporosis through a BMD test (N.I.H. 2018). It is important to note that a BMD test is meant to measure a person's results against that of a young and healthy grown-up.
The results of such a test isare what is commonly known as a T-scores. The purpose of a T-score is to determine the level of a person's bone density through units referred to as standard deviations. Below is a table portraying the recommended method by the World Health OrganisationOrganization demonstrating the different bone density levels used to diagnose Osteoporosis.

Table 1: Bone density measurements used to analyze the severity of Osteoporosis in a normal human being (Normal, Osteoporosis and severe Osteoporosis). Their T-scores are compared to that of a healthy adult not suffering from Osteoporosis, if within 1 (more or less) they are considered normal, if within 2.5 (more or less) they are considered to be suffering from Osteoporosis, if within 2.5 (more or less) and they have suffered from one or more fractures, they are considered to be suffering from severe Osteoporosis. Osteoporosis has proved to be a major problem in different ethnic populations. Asian populations generally have lower BMDs, compared to other ethnic groups (Thambiah and Yeap, 2020). According to various researchers, there are various ethnic differences in BMD. S., n.d.). It is a disease that develops as time progresses (N.I.H, 2018).
tThere are different studies that identity gender as a predisposing factor of Osteoporosis by bone mineral density. For instance, (Alswat 2017), indicates that women are easily predisposed to Osteoporosis as compared to men with the onset of the illness occurring early in the life of a woman.
The aim of this study is to critically analyze gender predisposition to osteoporosis within the context of South Asian descent. In doing so, the study will focus on the following objectives: To assess the meaning and clinical pathophysiology of Osteoporosis. To assess the prevalence of osteoporosis within the South Asian descent, compared to other populations. To analyze the predisposition of gender as a factor influencing the prevalence of osteoporosis within the South Asian population.
In a study comprising 769 men and women, the researchers found that the annual bone loss, specifically at the femoral neck was less in men than in women as it was 0.96% for women compared to 0.82% for men (Alswat, 2017). In another cohort study comprising a sample of 317 men and 362 women, all within the age bracket of 21-89, the rate of femoral strength reduction was higher in women than in men as it was 55% for women and 39% for men (Keaveny, Kopperdahl, Melton IIIII… et al., 2010).
Dig deeper into Are Portugals Policis Towards Drugs More Preventative with our selection of articles.
As such, Alswat's (2017) and Keaveny et al.'s (2010) studies clearly show that the rate of prevalence of Osteoporosis by bone mineral density is higher in women than in men due to the difference in the rate of bone loss between the two genders.
Additionally, the survey by Keaveny et al. (2010) showed that the onset of the condition of Osteoporosis in women begins in their 40s while that of men begins a whole decade later in their 50s. However, it is important to note that the N.I.H. (2018) point out that after the age of 65-70 the rate of bone deterioration tends to be similar for both men and women.
 Bandera, Munagapati, Karnati, Venkata, and Nidudhur (2015), identify two types of Osteoporosis namely, primary-which has no known cause- and secondary which is also known as age-related Osteoporosis. The onset of secondary Osteoporosis for both genders is at age 70 and it usually has a major impact on the cortical bone and trabecular (Bandela et al., 2011). Nonetheless, the above discussion indicates that risk factors for Osteoporosis are actually higher in women than in men.
With regard to ethnicity Thambiah and Yeap, 2020: Engine, Prentice, and Ward, (2015) acknowledge that the prevalence of Osteoporosis may differ in different regions and ethnic groups. In addition, in Nam (2013), race and ethnicity are identified as one of the risk factors of Osteoporosis. In another study, Nam et al. (2010) found prevalence differences between Chinese, Caucasian and African American women. The study indicates that Chinese and African American women have a higher rate of Osteoporosis compared to Caucasian women. In a study on Osteoporosis among South Asian women, Shakil et al. (2010) found that the prevalence of Osteoporosis also varies with age as shown below.
Table 2: Age and Prevalence of Osteoporosis
Bandera, Munagapati, Karnati, Venkata, and Nidudhur (2015), identify two types of Osteoporosis namely, primary-which has no known cause- and secondary which is also known as age-related Osteoporosis. The onset of secondary Osteoporosis for both genders is at age 70 and it usually has a major impact on the cortical bone and trabecular (Bandela et al., 2011). Nonetheless, the above discussion indicates that risk factors for Osteoporosis are actually higher in women than in men.
With regard to ethnicity Thambiah and Yeap, 2020: Engine, Prentice, and Ward, (2015) acknowledge that the prevalence of Osteoporosis may differ in different regions and ethnic groups. In addition, in Nam (2013), race and ethnicity are identified as one of the risk factors of Osteoporosis. In another study, Nam et al. (2010) found prevalence differences between Chinese, Caucasian and African American women. The study indicates that Chinese and African American women have a higher rate of Osteoporosis compared to Caucasian women. In a study on Osteoporosis among South Asian women, Shakil et al. (2010) found that the prevalence of Osteoporosis also varies with age as shown below.
Table 2: Age and Prevalence of Osteoporosis
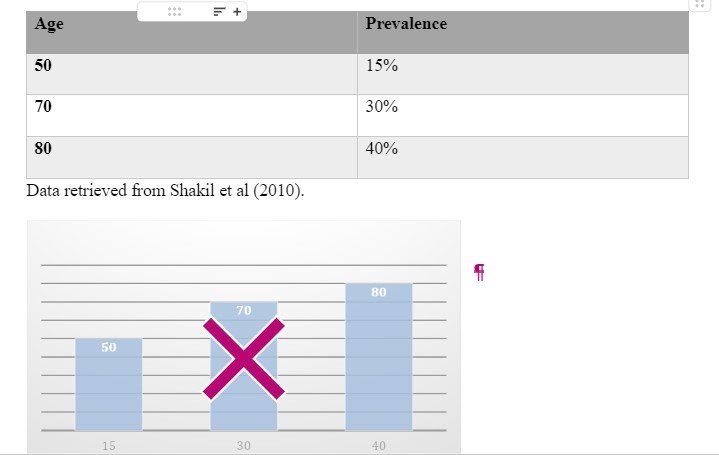 Table 2: Age in South Asian women is used to analyze whether it plays a role in the prevalence of Osteoporosis. The older the group, the higher the prevalence.
Ethnicity also plays a significant role with respect to fractures. Hip fractures in particular are highly prevalent among people in North America and Scandinavian countries while the same is lower among Asian and Latin Americans (Cooper et al., 2011). In Cauley (2011), the researcher showed that Caucasian women demonstrated the highest prevalence of hip fractures compared to Asian, African American and Hispanic women as shown in the table below
Table 2: Age in South Asian women is used to analyze whether it plays a role in the prevalence of Osteoporosis. The older the group, the higher the prevalence.
Ethnicity also plays a significant role with respect to fractures. Hip fractures in particular are highly prevalent among people in North America and Scandinavian countries while the same is lower among Asian and Latin Americans (Cooper et al., 2011). In Cauley (2011), the researcher showed that Caucasian women demonstrated the highest prevalence of hip fractures compared to Asian, African American and Hispanic women as shown in the table below
Table 3: Prevalence of Hip Fractures


Table 3: Ethnicity data between 100,000 (each) Caucasian, Asian, African American and Hispanic women used to analyze the prevalence of Osteoporosis in the aforesaid groups. Prevalence was highest in Caucasian women, followed by African American women and subsequently Hispanic women. Asian women portrayed the least prevalence. While the research by Thambiah et al (2020) and Nam et al (2013), indicates that South Asians are highly predisposed to Osteoporosis compared to other ethnic populations such as Caucasians, this is not the case with hip fractures. As can be observed from the data provided in the table above, Caucasian groups are highly exposed compared to other groups. Perhaps the reason for the discrepancy is an area for further research.
Risk factors for Osteoporosis
The National Osteoporosis Foundation (2008) gives the definition of risk factors for Osteoporosis as the factors that increase the likelihood of developing the said condition. Stetzer (2011) identifies various distinct categories of risk factors that could predispose a person to suffer from Osteoporosis. The said categories include; age, genetics, gender, ethnicity, prolonged use of certain medication, presence of certain chronic conditions and lifestyle. Stetzer (2011) noted that lifestyle is the only risk category which could be determines and controlled by the person involved and that the rest fall under inherited which she also referred to as uncontrollable risk factors. Before the definition of Osteoporosis was developed, the said condition was in fact referred to as a disease of the old as it would normally affect the older population (Stetzer 2011). The N.I.H (2018) has also identified that as one becomes olderr, the process of bone resorption intensifies and it becomes higher than the rate of bone formation and this in turn increases the risk of being predisposed to Osteoporosis due to poor bone health. In any case, gradual bone loss is an extremely common occurrence as one advances in age (Alswat 2017). As such, age is a risk factor in the development of osteoporosis.
Genetics
J.I. and Yu (2015) note that genetic predisposition could lead to Osteoporosis. Stetzer (2011) clarifies that although Osteoporosis is not inherited directly, family history can lead to higher risks for future generations. For instance, women linked to a maternal history of hip fractures tend to be at a greater risk than those who are not linked to such family history (Stetzer 2011).
Gender
Gender as a risk factor is typically associated with hormonal deficiency. J.I and Yu (2015) note that estrogen deficiency at menopause is a common pathway for Osteoporosis. Women are therefore likely to undergo two phases of bone loss. The first bone loss occurs after menopause which is usually associated with the deficiency of estrogen, while the second happens as age advances which usually leads to impaired bone formation and increased bone resorption (Ji and Yu, 2015). Additionally, women often have an earlier onset and faster rate of bone loss compared to men. This was observed in a study that involved 769 men and women, where rapid decline in bone mineral density occurred between 65-69 years for women while that of men occurred much later between 74-79 years (Alswat 2017).
Ethnicity
]With respect to ethnicity, a study by Nam et al (2013) reveals that South Asian, as well as Caucasian populations, tend to have low bone mass, and thiswhich in turn increases their risk of suffering from Osteoporosis in comparison to Hispanic and African American populations who have more significant bone mass and better bone strength and health in general. Furthermore, in another study, it was observed that women from certain ethnic groups such as Caucasian and South Asian groups tend to have smaller bone size which makes them easily predisposed to Osteoporosis (Stetzer 2011). The study also reported that South Asian women tend to experience early menopause which consequently reduces their bone mineral density hence increasing their risk of getting fractures as well as Osteoporosis (Stetzer 2011).
Medication
The prolonged use of certain medication especially for persons affected by other risk factors can indeed increase the prevalence of Osteoporosis (Stetzer 2011). N.I.A.M.S (2018) identify that the use of certain medication increases the users’ susceptibility to Osteoporosis by contributing to rapid bone loss. The most common drugs posing such risk include; glucocorticoids used to treat conditions like arthritis, immunosuppressants used during chemotherapy to treat cancer and thiazolidinediones used to treat type II diabetes (Allport 2008).
Chronic conditions
There are certain diseases or illnesses that could predispose one to Osteoporosis. These illnesses tend to be chronic which means that they tend to exist for a significant extended period of time and are usually extremely difficult to treat or cure. Stetzer (2011) identifies some of the chronic illnesses that predispose the patient to a high likelihood of suffering from Osteoporosis as the following; gastrointestinal diseases which may include Irritable Bowel Disease, or Premature Ovarian Failure which only affects women, endocrine diseases which may include conditions such as Diabetes Mellitus, genetic diseases which mostly affect women such as Cystic Fibrosis, as well as other diseases such as HIV/AIDS, Anorexia nervosa, particular types of Cancer and even depression. These chronic conditions not only weaken the health status of the body in general as well as that of bone tissues, but they also expose the victim to prolonged use of the medications that increase susceptibility of Osteoporosis which have already been discussed above.
Lifestyle
The risk factors associated with lifestyle can be attributed to behaviors relating to diet, alcohol consumption and smoking. Pouresmaeili, Kamalidehghan, Kamarehei, and Goh (2018) note that certain dietary habits are linked to Osteoporosis. According to Cohen, Wakefield, and Cohn (2016), healthy diets lower the impact and risks of Osteoporosis. Sommer et al. (2013) identifies excessive consumption of alcohol as a risk factor for Osteoporosis. In another study, Nachtigall et al. (2013) observed that cigarette smoking and alcohol intake are risk factors for Osteoporosis. In fact, high alcohol intake is associated with hip fractures (Zhang et al., 2015). Additionally, Paccou et al. (2015), argued that alcohol avoidance improves the rate of bone development. Smoking as a significant risk factor of Osteoporosis was identified in a study by Kline, Tang, and Levine (2015).
LITERATURE REVIEW
According to Compston et al., (2017), Osteoporosis is not only a progressive but also systemic skeletal disease. Osteoporosis is associated with low bone mass and micro architectural deterioration of bone tissues, which consequently leads to an increase in bone fragility and susceptibility to fracture. Therefore, the clinical significance of Osteoporosis is based on the consequential fractures that occur (Compston et al., 2017).
South Asia has various ethnic populations, there are two countries with multi-ethnic populations: Singapore and Malaysia. South Asian ethnic populations include Malays, Indians and Chinese. Different fracture risks and BMD are associated with different ethnic populations. In Singapore, after adjustment for body mass index, height and age, Chinese women were found to have significantly lower femoral neck BMD and higher lumbar spine BMD compared to Indians and Malays (Lim et al, 2005).
According to Compston et al. (2017), approximately 536,000 fractures as a result of Osteoporosis are reported annually in the U.K. Amongst the reported fractures, 79,000 were hip fractures, 66,000 were vertebral fractures, and 69,000 were forearm fractures, while 322,000 were other kinds (Compston et al., 2017). Notably, the researchers have reported that fractures arising from Osteoporosis result in severe pain and even disability in dire situations. As of 2010, Compston et al. stated that the annual cost to the National Health Service as a result of Osteoporosis was over 4.4 billion euros (2017). In the systemic review, the researchers noted that an approximation of one in five men would sustain one or more fragility fractures in their lifetime (Compston et al., 2017). According to the study, fracture rates differ according to geographical locations, socioeconomic statuses, age, gender as well as ethnicity.
Compston et al. also reported an increase in hip fractures among women and an increase in vertebral fractures among men (2017). In less than a millennium, the researchers predict that the cases of fractures reported arising from Osteoporosis will double.
A study by Hardcastle et al. (2019) identifyies how gender can increase the risk of Osteoporosis as it examines pregnancy-associated Osteoporosis. The authors define the condition as a rare syndrome that affects women who are in late expectancy period or early postpartum period. After reviewing the clinical features of ten cases of PAO in U.K, the researchers concluded that all ten cases presented vertebral fractures (Hardcastle et al., 2019). Osteoporosis is directly proportional to the levels of bone mineral density. From a systemic review and meta-analysis by Compston et al. (2017), it is noted that the risk of fracture increases with the decrease in bone mineral density. The study describes Osteoporosis with reference to the level of bone mass. This is measured as bone mineral density (Compston et al., 2017). The study also identifies that the femoral neck has a high predictive value for fracture risks. Consequently, Compston et al. recommends an application of a dual-energy x-ray absorptiometry (DXA) to the femoral neck in the diagnosis of Osteoporosis (2017). The ideal assessment intervention for testing bone mass and Osteoporosis diagnosis is the measure of bone mineral density (Bombak & Hanson, 2016). In addition, studies show that Osteoporosis tends to have a greater impact on frail older women (Bombak & Hanson, 2016). The researchers note that Osteoporosis is one of the most significant health issues that affect elderly people (Hejazi et al., 2020). Furthermore, they add that the condition is one of the most significant contributors to morbidity and mortality among the elderly (Hejazi et al., 2020). Consequently, the researchers also argue that the situation is thus a huge financial burden to the healthcare system. According to aAccording to a study in the U.K. conducted by Puspita et al. (2017), the, susceptibility to Osteoporosis is relatively high for South Asian women compared to Caucasian women. This has been attributed to the fact that they experience a breakdown of bone and tissue at an extremely rapid rate (Puspita et al., 2017). In the study, bone resorption level rates were determined by measuring the level of urinary N terminal telopeptide. This is a by-product of bone resorption. This enables the assessment of the quantity and rate of bone breakdown. Premenopausal South Asian women had higher levels of this by-product in their urine (Puspita et al., 2017). This was an indicator of elevated levels of bone resorption. The noted levels were not only alarming but also higher than the actual expectation of such an age group. In addition, the rate at which osteoclast cells break down bones in premenopausal South Asian women is faster than the rate the bones are being reformed. This makes South Asian women more susceptible to Osteoporosis and fractures (Puspita et al., 2017). It is this inequality in the levels of bone breakdown and formation that causes bone thinning which leads to Osteoporosis. Moreover, the study found that fluctuation in vitamin D levels and insufficient Calcium in South Asian women also contributes to susceptibility to the condition (Puspita et al., 2017). In a different study by Thambiah & Yeap (2020), the researchers found that South Asian women had the lowest BMD compared to other ethnicities. For vertebral fractures, the authors noted that the prevalence rates for South Asian women were averagely 24%. According to Ford (2017), premenopausal South Asian women are at a greater risk of developing Osteoporosis in their life compared to white women. According to U.K. researchers, as cited by Ford (2020), South Asian women are susceptible to falling and fractures. In a study that involved over 370 pre-and postmenopausal South Asian and white Caucasian women living in the U.K., bone tissue breakdown by osteoclasts was examined. From the study, (Ford, 2020) it was noted that the levels of urinary N terminal telopeptide were relatively high in South Asian women thus indicating rapid bone breakdown levels similar to what had been observed in the study by Puspita et al. (2020). In a different quasi-study by Shakil et al. (2010), awareness of Osteoporosis prevention among pre-and postmenopausal South Asian women attending two community centers was examined. The mean age of the women in the study was 52.3 years, most of whom were college-educated. From the study, women expressed knowledge on the significance of adequate calcium intake as well as its sources. The results from the study indicated that educational interventions are effective in improving Osteoporosis awareness. In conclusion therefore it is evident from the reviewed studies that Osteoporosis is a matter of significant concern that needs to be stemmed.
Research gap
There lacks extensive research on the prevalence of Osteoporosis within the South Asian populations among women of South Asian descent. Such studies could provide evidence for the increased bone resorption in postmenopausal women in South Asia. The lack of such studies creates a research gap, which the present study seeks to fill.
METHODOLOGY
The proposed study will use a systematic review of literature methodology (Appendix 1). The literature search strategy will involve searching for literature across three databases, namely Pubmed, BioMed Central, and CINAHL, google scholar MEDLINE, EMBASE, AMED, and Sci-Finder. Articles revealed through database searching will be first assessed using the title whereby unrelated pieces will be eliminated. The second step will use abstracts to review studies that do not have empirical research aim and exclude data. Commentaries will also be banned. Studies that have a conceptual or theoretical approach will also be excluded. Student dissertations will also be excluded. Articles that review other classes will also be excluded. Articles that use case study approach and articles lacking a study protocol will be excluded. Full-text articles will proceed to the next stage of the review where the criteria above will be further employed. The remaining full-text articles and eligibly companion articles selected through the full-text review will be used in the qualitative synthesis.
Inclusion Criteria
- Reviews on different types of fractures related to Osteoporosis will be looked at.
- Studies structured in the quantitative design will be considered.
- Scholarly articles will be referred to.
- Authoritative articles with full-text journal articles will be referred to.
- Empirical studies will be considered.
- Studies looking atin Osteoporosis in Asian/South Asian women in comparison to other ethnic groups will be used for reference.
- Studies comparing Osteoporosis in Caucasian women and Asian women will be regarded.
- Research to evidence higher occurrence of Osteoporosis in relation to ethnicity and gender will be considered relevant.
- Studies by other researchers on the same for comparison.
- General research on Osteoporosis without specific information and comparison about prevalence among different gender and ethnicity will be disregarded.
- Research focused on other risk factors away from gender and ethnicity will be excluded.
- Phenomenological and ethnographic design studies will be excluded.
- Statistics with a small sample size below 600 will be excluded.
Exclusion Criteria
Expected Outcomes
With regard to climate and diet, Calcium and Vitamin D rich foods are the subject of concern in this area. General nutrition is important as wellNutrition plays a key role in the management of this problem. Current recommendations are for 1200mg Calcium daily, dietary sources are preferred with supplements if necessary, because again the risk with Calcium supplements is that they increase the risk of kidney stones and some reports have indicated an increased risk of cardiovascular events, which remains controversial and has not been conclusively determined in all research. With regard to climate and diet, Calcium and Vitamin D rich foods are the subject of concern in this area. General nutrition is important as wellNutrition plays a key role in the management of this problem. Current recommendations are for 1200mg Calcium daily, dietary sources are preferred with supplements if necessary, because again the risk with Calcium supplements is that they increase the risk of kidney stones and some reports have indicated an increased risk of cardiovascular events, which remains controversial and has not been conclusively determined in all research. With regard to vitamin D, it comes in two forms; vitamin D2 (ergocalciferol) that plants make and D3 (cholicalciferol), the kind that comes from animal sources and the kind that we make in our skin and when we are exposed to UVB radiation. Vitamin D3 is also available as a dietary supplement sold over the counter whereas D2 is a subscription medication. D3 is found in a number of natural foods like egg yolk and salmon and is added to cereal and milk. A number of factors affects the skin's ability to produce vitamin D including latitude, seasons i.e. change in weather/ climate, skin tone, whether a person uses sunscreen and aging. The skin becomes less efficient at producing vitamin D with age. With regard to weather and climate, geographically, tropical countries experience more sunshine in comparison to countries closer to the poles or in the Polar Regions. Women in tropical countries are able to get and consume vitamin D from the sun as those areas are largely hot and sunny, unlike the coolerlder countries further up or down. Also, in countries that snow, injuries occur through falls by slipping which increases the risk of fractures especially to the wrist and the hip. The skin is therefore also another factor that influences Osteoporosis in South Asian women. As compared to women of color i.e. darker skin, white and Asian women have a considerably lower ability to process UVB rays that are instrumental in the conversion and processing of vitamin D. Ultimately this reduces the sources of vitamin D for South Asian women that is important in regulation of bone loss and bone formation hormones in a person. The Institute of Medicine recommends around 600 (IU/d) consumption of vitamin D, with excessive intake being discouraged as it increases the risk of developing high blood calcium and ultimately the risk of contracting kidney stones. The balance between vitamin D and calcium is important in the formation and breaking down and the absorption of bones. With regard to lifestyle, a study by Sfeir JG et al. (2018) showed that some yoga poses are harmful especially to back muscles and can cause severe harm to Osteoporosis prone spines. Yoga is an especially famous form of exercise in Asia. Some of the poses put a lot of pressure on the spine and therefore should be avoided. Yoga is however not the only sport generally that is harmful for a person who is prone to Osteopenia. Other exercises such as crunches and sit-ups put a lot of strain and pressure on the spine increasing risk. However, in relation to South Asian women, yoga is most relevant as it entails extreme manipulation of stretches that the body is put through and in the process, engages many bones (Sfeir JG et al, 2018). With regard to gender, a study in Denmark (Warming et al. Osteoporosis Int. 2002) that looked at bone mass against age in healthy men and women who were not taking any medication for Osteoporosis. It showed bone density as a function of aging women in four sites; distal forearm, total hip, lumbar spine and the total body Premenopausal women results showed stable bone mass as compared to postmenopausal women results which showed a steady decline in bone mass, except the hip that showed a steady decline in both. On the other hand, men exhibited a uniform decline in bone mass throughout their adult life. Women were also noted to lose over 50% more bone mass in the forearm than the men. Berger et al. (2008) delved deeper into women premenopausal and postmenopausal who were not on any bone medication at the time. It showed mass gain of bone density during age twenty which stayed constant up to forty years after which there is a steady decline. The most rapid bone mass loss occurs during the transition from premenopause to postmenopause between the age of 45 and 60, according to that research. Postmenopause, the rate slows but there is still steady bone loss. Low body weight is another keyalso a risk factor for Osteoporosis. With regard to this, many women in South Asia are small-bodied or rather slightly built. This therefore means that they are more prone to Osteopenia or Osteoporosis as compared to women in other areas for example Africa. This is because of the fact that slight bodies are directly related to smaller bones and therefore lower bone densities. Now, low bone density in itself is an added risk to a person and makes it easy to develop Osteoporosis in a shorter span of time over a person with high bone density. A study taken of women across the USA Gourlay et al. (2012) aimed at finding out how long it took women who had Osteopenia to develop Osteoporosis showed that an initial scan that showed mild Osteopenia or normal bone density in a T-scan would normally mean that it would take a long time for that to develop into Osteoporosis 10% of normal bone density women took up to 17 years to develop Osteoporosis while those with mild osteoporosis took about 5 years for it to develop into full-blown Osteoporosis and lastly those with advanced Osteopenia took about 1 year before it developed into Osteoporosis. Various results in research including Mayo Clinic have cited the fact that being of White or Asian descent increases the risk of contracting Osteoporosis in women. In both areas, ethnicity and gender, there are factors that point to the occurrence of these resulting into cases of Osteoporosis. More research focusing on these key factors has to be done so that more control can be established with regard to Osteoporosis.
FINDINGS
The findings from the research conducted systematically as proposed above, reveal that Osteoporosis is actually prevalent among South Asian women. The results showed that these women are not only predisposed to Osteoporosis based on their gender, but also due to their ethnicity. The study arrived at this conclusion after anlysinganalyzing the prevalence of Osteoporosis in women belonging to other different ethnic groups compared to South Asian women. The first comparison was between South Asian and Caucasian women and based on the results of the research, South Asian women depicted high levels of urinary N terminal telopeptide in comparison to Caucasian women within similar age groups (Puspita et al., 2017). The most outstanding finding of this research referred to above was that unlike their Caucasian counterparts, the level of urinary N terminal telopeptide was high even in premenopausal South Asian women. Usually, the levels of urinary N terminal telopeptide often increase during menopause going forward (Gossiel, et al. 2017). As a result, Osteoporosis tends to be more prevalent in older women (Hejazi et al., 2020). Consequently, the study went ahead to acknowledge that this state of affairs was quite unexpected. The research by Puspita et al (2017) looked into the effect of having high levels of urinary N terminal telopeptide in relation to Osteoporosis. It revealed the reason behind the prevalence of Osteoporosis in South Asian women as poor bone health resulting from high levels of urinary N terminal telopeptide (Puspita et al., 2017). The study Pupsita attributed these alarming levels to the rate at which the process of bone resorption occurs in the said women. The process occurs naturally in all human beings with the sole purpose of transferring calcium from the bone tissues in one’s body to the bloodstream (Gossiel, et al. 2017). The findings of the research by Ford demonstrated that the rate of bone resorption in South Asian women is higher than the rate at which bone formation occurs (Ford, 2020). This is what leads to poor bone health as mentioned herein and consequently makes South Asian women more predisposed to Osteoporosis. In addition, the research also disclosed that the levels of Vitamin-D fluctuate over time and this fluctuation then results in rapid bone resorption (Puspita et al., 2017). However, studies reveal that the said fluctuation can be attributed to the fact that they are exposed to different seasons and are therefore exposed to different weather conditions (Gossiel, et al. 2017). In conclusion, through the analysis of South Asian women the findings of the research reveal that gender and ethnicity do indeed play a role in the prevalence of Osteoporosis specifically by bone mineral density.
Statistical Analysis
The first analysis focused on the pattern of bone mineral density among the Asian population considered to be apparently healthy. The statistics were derived through measuring the bone mineral density of the femoral neck and the lumbar spine. The said measurements were then calculated to establish the T-scores of the subject population thus revealing those with Osteoporosis and those at risk of suffering from the same. This was achieved through the method recommended by the World Health OrganisationOrganization which has already been discussed herein.
Table 4: Bone Mineral Density Levels
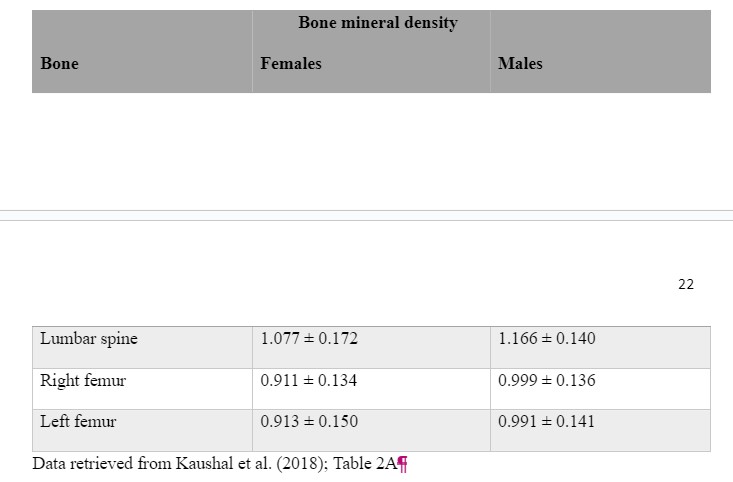
Table 4: Bone Mineral Density measured at g/cm2 of the Asian male and female population of an apparently healthy population suffering from Osteoporosis. The values presented are the mean ± standard deviation.
Table 5: T-Scores

T-scores of Asian Males were significantly higher at lumbar spine, right femur, and femur in comparison to their female counterparts. The values presented are the mean ± standard deviation.
The population analysedanalyzed above comprised of 216 women and 308 men. The male population portrayed higher bone mineral density which is inevitably associated with better bone health. Subsequently, it is evident that the prevalence of Osteoporosis is higher in women than in men.
The second analysis focused on the femoral neck, the lumbar spine and the total bone mineral density of women belonging to distinct ethnic groups namely; African-American, Caucasian and South Asian (Kaur et.al,.et.al, 2019).
Table 6: Femoral, lumbar spine and total bone mineral density levels
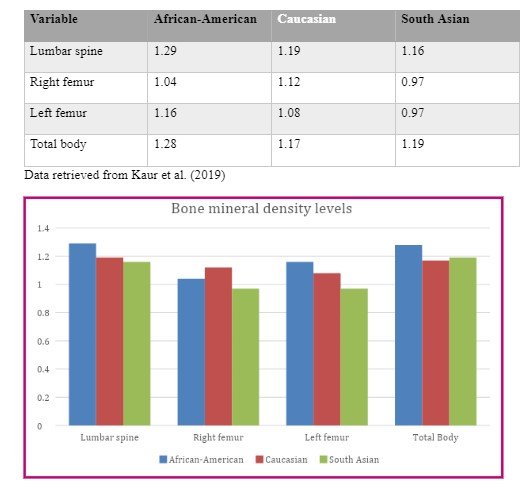 Table 6: Bone Mineral Density measurements of African-American women, Caucasian and South Asian women used to analyze the differences in ethnic groups. Measurements in gm/cm2.
The above statistics is evidence that bone mineral density levels vary from one ethnic group from another regardless of the gender since the analysis provided above focused on women only. This translates to different bone health status and ultimately different levels at which they are predisposed to Osteoporosis. While gender plays a role as has been established in the previous statistical analysis that has been provided above, ethnicity which is also usually involved with different races also comes into play in contributing to factors associated with Osteoporosis.
Table 6: Bone Mineral Density measurements of African-American women, Caucasian and South Asian women used to analyze the differences in ethnic groups. Measurements in gm/cm2.
The above statistics is evidence that bone mineral density levels vary from one ethnic group from another regardless of the gender since the analysis provided above focused on women only. This translates to different bone health status and ultimately different levels at which they are predisposed to Osteoporosis. While gender plays a role as has been established in the previous statistical analysis that has been provided above, ethnicity which is also usually involved with different races also comes into play in contributing to factors associated with Osteoporosis.
DISCUSSION
This section seeks to elucidate the findings of the research in relation to whether ethnicity and gender do indeed predispose the prevalence of Osteoporosis by bone mineral density while giving a critical appraisal and comparison of the work of other researchers in the said area. As stated above, the focal point of Osteoporosis by bone mineral density is the health status of the bone tissue which is usually determined by the amount of mineral contained in the bone (Compston et al., 2017).
The findings of this study point to the conclusion that difference in gender leads to differences in the bone mineral density. Therefore, gender has been found to be one of the key factors that influence the predisposition of osteoporosis. The same has been derived from the statistical analysis of this research which demonstrates that Asian men have a higher bone mineral density and are therefore less likely to suffer from Osteoporosis and fractures in comparison to their female counterparts.
Thambiah & Yeap (2020) arrived at this same conclusion in his their analysis of the difference in the rate of hip and vertebral fractures among the Asian population. The author in the said study acceded to the fact that age is not the only factor that leads to an increase in the aforementioned fractures. Consequently, Thambiah & Yeap (2020) attributed the prevalence of the fractures in women to their low bone mineral density and the lack thereof in men to their high bone mineral density.
One of the most informative literature on the prevalence of Osteoporosis in women is a paper by Alswat (2017). This paper refers to a study that was carried out on 28 elderly people which proved that despite the fact that both men and women lose bone mineral density as they advance in age, men tend to do much later and less rapidly than women (Alswat 2017). Additionally, in another study, the author further attributes the prevalence of Osteoporosis in women to the fact that men have lower urinary N-telopeptide and this therefore reduces the rate at which bone resorption occurs (Ferguson et al., 1997). The findings of this research are similar to those of the aforementioned study as they provide that South Asian women tend to be more predisposed to Osteoporosis as a result of the high levels of this hormone.
However, in another study by Cooper et al., (2011), the author cited that before the age of fifty, men tend to suffer from fractures more often compared to women as they are more physically active at this stage of their lives compared to women of the same age. Gender as a predisposing factor was also addressed in a study by Seeman (2005) who observed that the reason why bone resorption commences faster in women is due to the fact that they have smaller bones which leads to reduced bone strength at an early age. The findings of this research are in line with that of Seeman (2005) as they acknowledged that women have an early onset of factors such as bone resorption that leadled to Osteoporosis and are therefore at a higher risk.
Alswat (2017) therefore concludes that women are not only likely to suffer from fractures associated with Osteoporosis approximately five to ten years earlier, but they are also at a higher risk of being predisposed during their lifetime compared to men. From the above analysis, it is therefore evident that the findings of this research coincide to the findings of other researchers in relation to gender as a predisposing factor.
 The findings of the instant study also demonstrate that ethnicity plays a role in the prevalence of Osteoporosis by bone mineral density. This has been established by looking into the prevalence of Osteoporosis particularly in South Asian women in comparison to various other ethnicities (Lau et al., 2001). Other researchers such as Finkelstein et al., (2002) ranked the bone mineral density levels of the femoral neck and lumbar spine of women belonging to different ethnicities. As such, the study reported that African-American women had the highest levels, Caucasian women followed closely behind and South Asian women who are the subject of this research had the least bone mineral density.
From these statistics, Finkelstein et al., (2002) concluded that African-American women ran a significantly lower risk of Osteoporosis compared to Hispanic and South Asian women. Another study focusing on ethnic disparities in relation to the exposure of Osteoporosis particularly by bone mineral density reported that African-American women have a strong and powerful build and low bone loss rates which in turn protects them genetically speaking from experiencing Osteoporosis during their lifetime (Lee H, et al., 2013).
Suminski, Mattern & Devor ST (2002) acknowledge that the studies focusing on the ethnic differences of bone mineral density levels and bone health in general are quite limited. Nonetheless, the said authors admitted that ethnicity does indeed play a role in these differences. The same was reiterated in another study which noted that different researchers have observed that difference in ethnicity contributes to the difference in the bone mineral density (Leslie 2012).
In additionAdditionally, Thambiah & Yeap (2020) reported that Asian populations generally tend to have lower bone mineral density levels compared to other ethnicities. This study also identified that due to the different races of different ethnic groups, this then affects the ability of one’s ability to process Vitamin D which is essential in promoting bone strength and health in general Thambiah & Yeap (2020).
In another study mainly focusing on the prevalence of Osteoporosis in South Asian women, the researchers stated that this particular group had a high risk and were predisposed to Osteoporosis even before experiencing menopause (Puspita et al., 2017). As such, premonopausal South Asian women were compared to premonopausal Caucasian women and it was concluded that the former werewas more predisposed to Osteoporosis than the former.
One paramount study which focused on different groups within the same region was also considered. The said study by Thambiah & Yeap (2020) focused on the South Eastern Asian region as it has multiple distinct ethnic groups namely; Malays, Chinese and Indians. Thambiah & Yeap (2020) found that the Chinese had the lowest vertebral and hip bone mineral density in comparison to Malays and Indians and this therefore makes them more susceptible to fractures that occur due to Osteoporosis.
However, they also observed that low bone mineral density is not always equated to higher risks in relation to Osteoporosis. Despite the unexpected nature of the aforementioned observation, Thambiah & Yeap (2020) found that even though Asians had lower bone mineral density, they did not suffer from fractures related to Osteoporosis more than Caucasians who had higher bone mineral density levels.
It is therefore evident from the above analysis that different researchers have carried out investigations in different regions, as well as different ethnic groupsas well as even within different ethnic groups in similarwithin similar regions. These studies have and concluded that different ethnic groups genetically display different bone mineral density levels which then leads to different prevalence levels and risks of Osteoporosis.
The findings of this study are thus similar to those of other studies that have been carried out in relation to the issues that are the subject of this research. Looking at this concept while focusing on South Asian populations, this study demonstrates the influence of differences in gender and ethnic populations on the predisposition of osteoporosis. The same was observed in the statistical analysis which focused on women of similar ages but from three distinct ethnic groups. However, it is paramount to note that the research and studies surrounding the influence that gender and ethnicity have on the risk of suffering from Osteoporosis are quite limited. Regardless of such limited resources, this study has successfully deduced relevant conclusions through the analysis of various materials to determine how gender and ethnicity affect the prevalence of Osteoporosis by bone mineral density.
The main purpose of the study however, was to narrow down to South Asian women in an effort to provide specific statistics and observation with regard to the main issue related to this research. This is because there as previously identified in this study, there is little research on South Asian women and the reasons behind they tend to be more predisposed to Osteoporosis. This research has therefore looked into the factors that contribute to this phenomenon.
The findings of the instant study also demonstrate that ethnicity plays a role in the prevalence of Osteoporosis by bone mineral density. This has been established by looking into the prevalence of Osteoporosis particularly in South Asian women in comparison to various other ethnicities (Lau et al., 2001). Other researchers such as Finkelstein et al., (2002) ranked the bone mineral density levels of the femoral neck and lumbar spine of women belonging to different ethnicities. As such, the study reported that African-American women had the highest levels, Caucasian women followed closely behind and South Asian women who are the subject of this research had the least bone mineral density.
From these statistics, Finkelstein et al., (2002) concluded that African-American women ran a significantly lower risk of Osteoporosis compared to Hispanic and South Asian women. Another study focusing on ethnic disparities in relation to the exposure of Osteoporosis particularly by bone mineral density reported that African-American women have a strong and powerful build and low bone loss rates which in turn protects them genetically speaking from experiencing Osteoporosis during their lifetime (Lee H, et al., 2013).
Suminski, Mattern & Devor ST (2002) acknowledge that the studies focusing on the ethnic differences of bone mineral density levels and bone health in general are quite limited. Nonetheless, the said authors admitted that ethnicity does indeed play a role in these differences. The same was reiterated in another study which noted that different researchers have observed that difference in ethnicity contributes to the difference in the bone mineral density (Leslie 2012).
In additionAdditionally, Thambiah & Yeap (2020) reported that Asian populations generally tend to have lower bone mineral density levels compared to other ethnicities. This study also identified that due to the different races of different ethnic groups, this then affects the ability of one’s ability to process Vitamin D which is essential in promoting bone strength and health in general Thambiah & Yeap (2020).
In another study mainly focusing on the prevalence of Osteoporosis in South Asian women, the researchers stated that this particular group had a high risk and were predisposed to Osteoporosis even before experiencing menopause (Puspita et al., 2017). As such, premonopausal South Asian women were compared to premonopausal Caucasian women and it was concluded that the former werewas more predisposed to Osteoporosis than the former.
One paramount study which focused on different groups within the same region was also considered. The said study by Thambiah & Yeap (2020) focused on the South Eastern Asian region as it has multiple distinct ethnic groups namely; Malays, Chinese and Indians. Thambiah & Yeap (2020) found that the Chinese had the lowest vertebral and hip bone mineral density in comparison to Malays and Indians and this therefore makes them more susceptible to fractures that occur due to Osteoporosis.
However, they also observed that low bone mineral density is not always equated to higher risks in relation to Osteoporosis. Despite the unexpected nature of the aforementioned observation, Thambiah & Yeap (2020) found that even though Asians had lower bone mineral density, they did not suffer from fractures related to Osteoporosis more than Caucasians who had higher bone mineral density levels.
It is therefore evident from the above analysis that different researchers have carried out investigations in different regions, as well as different ethnic groupsas well as even within different ethnic groups in similarwithin similar regions. These studies have and concluded that different ethnic groups genetically display different bone mineral density levels which then leads to different prevalence levels and risks of Osteoporosis.
The findings of this study are thus similar to those of other studies that have been carried out in relation to the issues that are the subject of this research. Looking at this concept while focusing on South Asian populations, this study demonstrates the influence of differences in gender and ethnic populations on the predisposition of osteoporosis. The same was observed in the statistical analysis which focused on women of similar ages but from three distinct ethnic groups. However, it is paramount to note that the research and studies surrounding the influence that gender and ethnicity have on the risk of suffering from Osteoporosis are quite limited. Regardless of such limited resources, this study has successfully deduced relevant conclusions through the analysis of various materials to determine how gender and ethnicity affect the prevalence of Osteoporosis by bone mineral density.
The main purpose of the study however, was to narrow down to South Asian women in an effort to provide specific statistics and observation with regard to the main issue related to this research. This is because there as previously identified in this study, there is little research on South Asian women and the reasons behind they tend to be more predisposed to Osteoporosis. This research has therefore looked into the factors that contribute to this phenomenon.
CONCLUSION
Research was conducted to prove that amongst other factors, gender and ethnicity contribute to the occurrence of Osteoporosis in women, with a focus on South Asian women as has been stated above as compared to women of different ethnic descent. Gender was a primary focus in this study. Contrast was therefore drawn in various places between men and women and the occurrence of Osteoporosis in both to determine the theory sought to be proven. With regard to this, women across all ages were considered, taking into account all the issues related to gender and women in this regard. Research focused on premenopausal and postmenopausal women for the study as well as hormones occurring in women i.e. estrogen, weight, age and residence amongst other factors. These were some of the factors that influenced the gender aspect of the research. A significant difference was found as a result of this research between men and women relating to the study so that many more women suffer from the disease at an earlier stage in their lives as compared to men. In relation to ethnicity, the study focused on women of South Asian descent to the exclusion of all others except for comparison purposes. The study found that ethnicity is indeed a contributor to the risk factors of Osteoporosis amongst women. Research was conducted based on various factors in relation to ethnicity, taking due regard of issues that set them apart from women of other ethnic descent including diet, lifestyle and climate in the regions in which they live in. With regard to diet focus was on essential minerals for bone formation and breakdown in the body i.e. vitamins D and Calcium. Lifestyle focused on exercise and climate on weather patterns that have a direct impact on a person's ability to absorb and utilize the minerals aforementioned. Studies conducted on women across different ethnicities showed a significant difference in the occurrence of Osteoporosis among South Asian women as compared to White, Black, Hispanic or other women of different ethnic descent. The result being that through this comparison, ethnicity was proven to be a contributor to the risk factors of Osteoporosis in women in general. The study here generally showed a prevalence in specific ethnicities, with them facing a higher risk than in the others. Obtaining this information in relation to women of Asian descent was crucial because of the little research there is as relates to them specifically and the risk they face in relation to Osteoporosis. A lot of data is available on White women and women in general but this study focused on bringing the women of Asian descent into focus. This ended up demonstrating a significant difference between women of other ethnic descent as compared to those of Asian descent. The literature also brought into focus contributing factors in this regard that put them at an increased risk including nutrition. The limitation of this study is that it was pinned on desktop research and an opportunity to undertake field research was not available. However, the research used a broad range of authoritative material that managed to portray accurate results. Each study is crucial to the health community at large because of the stark differences in each ethnic community that makes them unique in their health concerns. Every study has the probability of showing results and statistics previously undiscovered or unknown. Further research should be done to allow for the education of women on these matters and as to the diagnosis, prevention and treatment options that are available to them. It can be concluded therefore that gender on an overall spectrum represents an increased risk in a population to develop Osteoporosis and that ethnicity specifically heightens these risks amongst a population of women.
APPENDIX
Appendix 1: PRISMA chart developed to illustrate the methodology for this project.

REFERENCES
Allport J. 2008. Incidence and prevalence of medication-induced osteoporosis: evidence-based review. Current Opinion in Rheumatology, pp. 435-441.
Alswat K. A. 2017. Gender disparities in osteoporosis. Journal of clinical Medicine Research, 9(5), pp. 382–387. https://doi.org/10.14740/jocmr2970w
Bandela, V., Munagapati, B., Karnati, R.K.R., Venkata, G.R.S. and Nidudhur, S.R., 2015. Osteoporosis: its prosthodontic considerations-a review. Journal of Clinical and Diagnostic Research: JCDR, 9(12), p.ZE01.
Bombak A. E., Hanson H. M. (2016) “Qualitative Insights from the Osteoporosis Research: A Narrative Review of the Literature", Journal of Osteoporosis, Article ID 7915041. https://doi.org/10.1155/2016/791504
Cauley, J.A., 2011. Defining ethnic and racial differences in osteoporosis and fragility fractures. Clinical Orthopaedics and Related Research®, 469(7), p.1891.
Cheung, C.L., Ang, S.B., Chadha, M., Chow, E.S.L., Chung, Y.S., Hew, F.L., Jaisamrarn, U., Ng, H., Takeuchi, Y., Wu, C.H. and Xia, W., 2018. An updated hip fracture projection in Asia: the Asian Federation of osteoporosis societies study. Osteoporosis and Sarcopenia, 4(1), pp.16-21.
Claudie Berger, Lisa Langsetmo, Lawrence Joseph, David A. Hanley, K. Shawn Davison, Robert Josse, Nancy Kreiger, Alan Tenenhouse, David Goltzman and ; and the Canadian Multicentre Osteoporosis Study Research Group 2008. Change in bone mineral density as a function of age in women and men and association with the use of antiresorptive agents. https://doi.org/10.1503/cmaj.071416
Cohen, J.E., Wakefield, C.E. and Cohn, R.J., 2016. Nutritional interventions for survivors of childhood cancer. Cochrane Database of Systematic Reviews, (8).
Compston, J., Cooper, A., Cooper, C., Gittoes, N., Gregson, C., Harvey, N., Hope, S., Kanis, J. A., McCloskey, E. V., Poole, K., Reid, D. M., Selby, P., Thompson, F., Thurston, A., Vine, N., & National Osteoporosis Guideline Group (NOGG) (2017). UK clinical
guideline for the prevention and treatment of osteoporosis. Archives of osteoporosis, 12(1), 43. https://doi.org/10.1007/s11657-017-0324-5
Cooper, C., Cole, Z.A., Holroyd, C.R., Earl, S.C., Harvey, N.C. and Dennison, E.M., (2011). CSA Working Group on Fracture Epidemiology. IOF CSA Working Group on Fracture Epidemiology. Secular trends in the incidence of hip and other osteoporotic fractures. Osteoporos Int, 22(5), pp.1277-88.
Elizabeth S. Stetzer (2011). Identifying Risk Factors for Osteoporosis in Young Women. https://nsuworks.nova.edu/ijahsp/
Ford. S. (2017). South Asian women in UK may have higher osteoporosis risk. NursingTimes. https://www.nursingtimes.net/news/research-and-innovation/south-asian-women-in-uk-may-have-higher-osteoporosis-risk-21-03-2017/
Greenspan SL, Dresner-Pollak R, Parker RA, London D, Ferguson L. Diurnal 1997. Variation of bone mineral turnover in elderly men and women. Calcif Tissue Int. 419-423
Darling AL, Hart KH, Gossiel F, 2017. Higher bone resorption excretion in South Asian Women vs. White Caucasians. D-Fines Cohort Study 47-53.
Hardcastle, S., Yahya, F. & Bhalla, A. 2019. Pregnancy-associated osteoporosis: a UK case series and literature review. Osteoporos Int 30, 939–948. https://doi.org/10.1007/s00198-019-04842-w
Ji MX, Yu Q. Primary osteoporosis in postmenopausal women. Chronic Dis Transl Med. 2015 Mar 21;1(1):9-13. doi: 10.1016/j.cdtm.2015.02.006. PMID: 29062981; PMCID: PMC5643776.
Joshua N Farr, Ming Xu, Megan M Weivoda, David G Monroe, Daniel G Fraser, Jennifer L Onken, Brittany A Negley, Jad G Sfeir, Mikolaj B Ogrodnik, Christine M Hachfeld, Nathan K LeBrasseur, Matthew T Drake, Robert J Pignolo, Tamar Pirtskhalava, Tamara Tchkonia, Merry Jo Oursler, James L Kirkland, Sundeep Khosla 2018. Targeting Cellular Senescence Prevents Age-Related Bone Loss. Nature medicine Volume 23.
Keaveny, T.M., Kopperdahl, D.L., Melton III, L.J., Hoffmann, P.F., Amin, S., Riggs, B.L. and Khosla, S., 2010. Age‐dependence of femoral strength in white women and men. Journal of Bone and Mineral Research, 25(5), pp.994-1001.
Kline, J., Tang, A. and Levin, B., 2016. Smoking, alcohol and caffeine in relation to two hormonal indicators of ovarian age during the reproductive years. Maturitas, 92, pp.115-122.
Lau, E., Lee, J.K., Suriwongpaisal, P., Saw, S.M., Das De, S., Khir, A., 2001. The incidence of hip fracture in four Asian countries: the Asian Osteoporosis Study (AOS). Osteoporosis Int, 12, pp. 239-43.
Leslie WD. Clinical review: Ethnic differences in bone mass--clinical implications. J Clin Endocrinol Metab. 2012 Dec; 97(12):4329-40.
Levis, S. and Lagari, V.S., 2012. The role of diet in osteoporosis prevention and management. Current Osteoporosis Reports, 10(4), pp.296-302.
Lim, P.S., Ong, F.B. Adeeb, N., Seri, S.S. Noor-Aini, M.Y., Shamsuddin, K. 2005. Bone health in urban midlife Malaysian women: risk factors and prevention. Osteoporosis Int, 16, pp. 2069-79
Margaret L. Gourlay, M.D., M.P.H., Jason P. Fine, Sc.D., John S. Preisser, Ph.D., Ryan C. May, Ph.D., Chenxi Li, Ph.D., Li-Yung Lui, M.S., David F. Ransohoff, M.D., Jane A. Cauley, Dr.P.H., and Kristine E. Ensrud, M.D., M.P.H. 2012. Bone-Density Testing Interval and Transition to Osteoporosis in Older Women. 10.1056/NEJMoa1107142
Marquez, M.A., Melton L., Muhs, J.M., Crowson, C.S., Tosomeen, A., O’Connor, M.K., O’Fallon, W., Riggs, B.L., 2001. Bone density in an immigrant population from South East Asia. Osteoporosis Int, 12(7), pp. 595-604.
Nachtigall, M.J., Nazem, T.G., Nachtigall, R.H. and Goldstein, S.R., 2013. Osteoporosis risk factors and early life-style modifications to decrease disease burden in women. Clinical Obstetrics and Gynecology, 56(4), pp.650-653.
Nam, H.S., Kweon, S.S., Choi, J.S., Zmuda, J.M., Leung, P.C., Lui, L.Y., Hill, D.D., Patrick, A.L. and Cauley, J.A., 2013. Racial/ethnic differences in bone mineral density among older women. Journal of Bone and Mineral Metabolism, 31(2), pp.190-198.
Neelam Kaushal Divya Vohora Rajinder K. Jalali Sujeet Jha 2018. Prevalence of osteoporosis and osteopenia in an apparently healthyIndian population - a cross-sectional retrospective study. Volume 4, Issue 2, Pages 53-60, ISSN 2405-5255, https://doi.org/10.1016/j.afos.2018.04.002
National Osteoporosis Foundation 2008 Washington, DC: Prevention: who’s at risk? Retrieved from https://nof.org/prevention/risk.htm NHS. n.d. Osteoporosis. https://www.nhs.uk/conditions/osteoporosis/
NIH. 2018. Osteoporosis in Men. NIH. Retrieved from https://www.bones.nih.gov/health-info/bone/osteoporosis/men
Paccou, J., Edwards, M.H., Ward, K., Jameson, K., Moon, R., Dennison, E. and Cooper, C., 2015. Relationships between bone geometry, volumetric bone mineral density and bone microarchitecture of the distal radius and tibia with alcohol consumption. Bone, 78, pp.122-129.
Pouresmaeili, F., Kamalidehghan, B., Kamarehei, M. and Goh, Y.M., 2018. A comprehensive overview on osteoporosis and its risk factors. Therapeutics and Clinical Risk Management, 14, p.2029.
Puspita, E. M., Siregar, M. F. G., & Adenin, I. (2017). Correlation of estradiol serum levels with classification of osteoporosis risk OSTA (Osteoporosis Self-Assessment Tools for Asian) in menopause women. Bali Med. J, 6(1), 52-55.
Putman MS, Yu EW, Lee H, et al. 2013. Differences in skeletal microarchitecture and strength in African-American and Caucasian women. J Bone Miner Res, 2177-2185.
Ringle, K. 2009. An Investigation of Bone Mineral Density and Bone Mineral Content among Hispanic Women by Lifestyle Factors.
Shakil, A., Gimpel, N.E., Rizvi, H. et al. (2010). Awareness and Prevention of Osteoporosis among South Asian Women. J Community Health 35, 392–397. https://doi.org/10.1007/s10900-010-9263-4
Solomon, D.H., Finkelstein, J.S., Polinski, J.M. et al. A randomized controlled trial of mailed osteoporosis education to older adults. Osteoporos Int 17, 760–767 (2006). https://doi.org/10.1007/s00198-005-0049-y
Sommer I, Erkkilä AT, Järvinen R, Mursu J, Sirola J, Jurvelin JS, Kröger H, Tuppurainen M. 2013. Alcohol consumption and bone mineral density in elderly women. Public Health Nutr. Apr; 16(4):704-12
Suminski RR, Mattern CO, Devor ST. 2002. Influence of racial origin and skeletal muscle properties on disease prevalence and physical performance. Sports Med. 2002, 667-673.
Wang XF, Duan Y, Beck TJ, Seeman E. 2005. Varying contributions of growth and ageing to racial and sex differences in femoral neck structure and strength in old age. pp. 978-986.
Warming, L., Hassager, C. & Christiansen, C. Changes in Bone Mineral Density with Age in Men and Women: A Longitudinal Study. Osteoporos Int 13, 105–112 (2002). https://doi.org/10.1007/s001980200001.
Thambiah, S.C. and Yeap, S.S., 2020. Osteoporosis in South-East Asian Countries. The Clinical Biochemist Reviews, 41(1), p.29.
Zengin A, Prentice A, Ward KA. 2015. Ethnic differences in bone health. Front Endocrinol (Lausanne).6:24.
Zhang, X., Yu, Z., Yu, M. and Qu, X., 2015. Alcohol consumption and hip fracture risk. Osteoporosis International, 26(2), pp.531-542.
Continue your journey with our comprehensive guide to Opportunities in the Adoption of Modern Construction Techniques in the UK.



- 24/7 Customer Support
- 100% Customer Satisfaction
- No Privacy Violation
- Quick Services
- Subject Experts